You might also like
- Open Letter To ICE From Medical Professionals Re COVID-19Document68 pagesOpen Letter To ICE From Medical Professionals Re COVID-19Jesus Garcia0% (1)
- Neurologic NursingDocument14 pagesNeurologic Nursingtheglobalnursing100% (6)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Homeopathy Liver Problems - British Homeopathic AssociationDocument10 pagesHomeopathy Liver Problems - British Homeopathic AssociationStellaEstelNo ratings yet
- Anaes MCQ PDFDocument212 pagesAnaes MCQ PDFnot here 2make friends sorry100% (4)
- Tracheostomy Operating TechniqueDocument34 pagesTracheostomy Operating TechniqueIsa BasukiNo ratings yet
- Bowel Nosodes Notes: Henry C Allen - Timing of Bowel Nosode RXDocument21 pagesBowel Nosodes Notes: Henry C Allen - Timing of Bowel Nosode RXFuente DelavidaNo ratings yet
- TracheostomyDocument31 pagesTracheostomyTonyScaria100% (1)
- Hospital Oxygen Filling System For PatientsDocument95 pagesHospital Oxygen Filling System For PatientsShishir KumarNo ratings yet
- Tracheostomy DR KVLN Rao PDFDocument33 pagesTracheostomy DR KVLN Rao PDFVenkata Krishna Kanth ThippanaNo ratings yet
- Tracheostomy Care and ManagementDocument63 pagesTracheostomy Care and ManagementAyesha FayyazNo ratings yet
- Defining Physiology: Principles, Themes, Concepts.: Hwee Ming Cheng Kin Kheong Mah Kumar SeluakumaranDocument104 pagesDefining Physiology: Principles, Themes, Concepts.: Hwee Ming Cheng Kin Kheong Mah Kumar SeluakumaranGiovanni HenryNo ratings yet
- Defining Physiology: Principles, Themes, Concepts.: Hwee Ming Cheng Kin Kheong Mah Kumar SeluakumaranDocument104 pagesDefining Physiology: Principles, Themes, Concepts.: Hwee Ming Cheng Kin Kheong Mah Kumar SeluakumaranGiovanni HenryNo ratings yet
- TracheostomyDocument35 pagesTracheostomyAbdur Raqib100% (1)
- Gestational Diabetes Screening Case StudiesDocument50 pagesGestational Diabetes Screening Case Studiesdiabetes asia100% (1)
- Potassium ChlorideDocument2 pagesPotassium ChlorideRene John FranciscoNo ratings yet
- Assignment On TreacheostomyDocument7 pagesAssignment On Treacheostomysantosh kumarNo ratings yet
- Tracheostomy: by Veronica Robert, MD 4 Moderator DR - SamsonDocument41 pagesTracheostomy: by Veronica Robert, MD 4 Moderator DR - SamsonMacktevin FraterinNo ratings yet
- Bee Venom FAQsDocument6 pagesBee Venom FAQsRenaHeidNo ratings yet
- Tracheostomy Procedure ExplainedDocument6 pagesTracheostomy Procedure ExplainedMa. Ydela Meradores100% (1)
- 2018 Cardiovascular PhysiologyDocument197 pages2018 Cardiovascular PhysiologyGladys ParedesNo ratings yet
- Sept 2020 MRCS RecallsDocument46 pagesSept 2020 MRCS RecallsGiovanni Henry75% (4)
- TracheostomyDocument58 pagesTracheostomylissajanet1016100% (1)
- Medical EMQs and Clinical ScenariosDocument18 pagesMedical EMQs and Clinical ScenariosMehdi Hasan MazumderNo ratings yet
- ISUOG Basic Training: Gynecological Ultrasound: The BasicsDocument34 pagesISUOG Basic Training: Gynecological Ultrasound: The BasicsTheodoraAlinaNo ratings yet
- Recalls of Paper 2 - 11/9/2018: ConsentDocument6 pagesRecalls of Paper 2 - 11/9/2018: ConsentGiovanni Henry0% (1)
- TracheotomyDocument19 pagesTracheotomyKarina BundaNo ratings yet
- Surgery Questions EssayDocument11 pagesSurgery Questions Essaymimycutey100% (3)
- Music TherapyDocument2 pagesMusic TherapyGrace Ann Rodriguez SanDiegoNo ratings yet
- Uia28 TracheostomyDocument8 pagesUia28 TracheostomyAashik 249No ratings yet
- Laryngeal Split & Rib Cartilage Interpositional GraftingDocument9 pagesLaryngeal Split & Rib Cartilage Interpositional GraftingAlexi Chávez EchevarríaNo ratings yet
- Tracheostomy: As. Univ. Dr. Andrei Cristian Bobocea As. Univ. Dr. Serban Radu MatacheDocument21 pagesTracheostomy: As. Univ. Dr. Andrei Cristian Bobocea As. Univ. Dr. Serban Radu MatacheIoana VasileNo ratings yet
- 216851-Article Text-533920-1-10-20211102Document5 pages216851-Article Text-533920-1-10-20211102Vaino MungobaNo ratings yet
- JMedLife 07 343 PDFDocument6 pagesJMedLife 07 343 PDFAzmi FananyNo ratings yet
- Grenier 2009Document18 pagesGrenier 2009PabloNo ratings yet
- 241 TracheostomyDocument12 pages241 Tracheostomyalbert hutagalungNo ratings yet
- Chest Wall, Lung, Mediastinum, and Pleura: Trachea AnatomyDocument3 pagesChest Wall, Lung, Mediastinum, and Pleura: Trachea AnatomyNur SulistiyaningsihNo ratings yet
- E T IntubationDocument15 pagesE T Intubationjtalan9No ratings yet
- Tracheostomy 191224152833Document106 pagesTracheostomy 191224152833Dimas SevantoNo ratings yet
- Failed Fiberoptic Intubation and Surgical Tracheostomy in A Case of Down's Syndrome With GoiterDocument3 pagesFailed Fiberoptic Intubation and Surgical Tracheostomy in A Case of Down's Syndrome With GoiterxkrautNo ratings yet
- Tracheostomy EmergenciesLaura J. BontempoDocument11 pagesTracheostomy EmergenciesLaura J. BontempoIsmael Erazo AstudilloNo ratings yet
- Tracheostomy Procedure GuideDocument18 pagesTracheostomy Procedure GuideSudhanshu ShekharNo ratings yet
- 6 Original Articles - Review Article - Tracheotomy in The Icu - Current Opinions, C R Van Schalkwyk WDocument4 pages6 Original Articles - Review Article - Tracheotomy in The Icu - Current Opinions, C R Van Schalkwyk WAbhilash AntonyNo ratings yet
- TracheostomyDocument28 pagesTracheostomyprivatejarjarbinksNo ratings yet
- CM 05015Document4 pagesCM 05015Yacine Tarik AizelNo ratings yet
- The Changing Role For Tracheostomy in Patients Requiring Mechanical VentilationDocument11 pagesThe Changing Role For Tracheostomy in Patients Requiring Mechanical VentilationGhost11mNo ratings yet
- Tracheostomy 141214210035 Conversion Gate01Document69 pagesTracheostomy 141214210035 Conversion Gate01denaNo ratings yet
- Novel Scoring System for Tracheal Stenosis ProceduresDocument7 pagesNovel Scoring System for Tracheal Stenosis ProceduresAraceli BarreraNo ratings yet
- Preserving Oral Communication in Individuals With Tracheostomy and Ventilator DenpendencyDocument7 pagesPreserving Oral Communication in Individuals With Tracheostomy and Ventilator Denpendencypico 24No ratings yet
- Handout TracheostomyDocument1 pageHandout TracheostomyDhAiRyA ArOrANo ratings yet
- A Case of Anterior Tracheal Rupture Following Trivial TraumaDocument5 pagesA Case of Anterior Tracheal Rupture Following Trivial TraumaBhavesh PatadiyaNo ratings yet
- CekDocument3 pagesCekNasrudin EfendiNo ratings yet
- Anaesthesia For Tracheal and Airway Surgery: Aetiology of Adult Laryngotracheal StenosisDocument4 pagesAnaesthesia For Tracheal and Airway Surgery: Aetiology of Adult Laryngotracheal StenosisRicardoNo ratings yet
- 53 47 PBDocument7 pages53 47 PBpinaNo ratings yet
- Case Onko 2 Febby ShabrinaDocument16 pagesCase Onko 2 Febby ShabrinaVandy IkraNo ratings yet
- Annrcse01509 0sutureDocument3 pagesAnnrcse01509 0sutureNichole Audrey SaavedraNo ratings yet
- Tracheal TraumaDocument3 pagesTracheal TraumaWalid DarwicheNo ratings yet
- Tracheostomy and Airway Emergencies22Document26 pagesTracheostomy and Airway Emergencies22devilheadhuntersNo ratings yet
- Amit Tracheostomy Presentation 12 Aug 2010Document59 pagesAmit Tracheostomy Presentation 12 Aug 2010Amit KochetaNo ratings yet
- Thoracocentesis: Nadja E. SigristDocument4 pagesThoracocentesis: Nadja E. SigristDwi AnaNo ratings yet
- Ventilatory Management of Severe Tracheal Stenosis: Rakesh Lodha, Lokesh Guglani, S.C. Sharma and S.K. KabraDocument4 pagesVentilatory Management of Severe Tracheal Stenosis: Rakesh Lodha, Lokesh Guglani, S.C. Sharma and S.K. KabraPcrNo ratings yet
- Anatomia y Fisiologia TQTDocument7 pagesAnatomia y Fisiologia TQThuevazooo04No ratings yet
- Estenosis Tracheal No QX RevisafoDocument13 pagesEstenosis Tracheal No QX RevisafoFabiolaNo ratings yet
- An Unusual Complication of Chest Tube ThoracostomyDocument4 pagesAn Unusual Complication of Chest Tube Thoracostomyleonerbinondo22No ratings yet
- Chest Trauma SeminarDocument45 pagesChest Trauma Seminarha9719199No ratings yet
- Ent Throat 1Document58 pagesEnt Throat 1ميمونه عبدالرحيم مصطفىNo ratings yet
- Tracheal Perforation Managed by Temporary Tracheostomy in A HorseDocument3 pagesTracheal Perforation Managed by Temporary Tracheostomy in A HorseR. DaharyNo ratings yet
- Pisa Nu 2009Document6 pagesPisa Nu 2009vinicius.alvarez3No ratings yet
- PIIS152229420800007XDocument13 pagesPIIS152229420800007XOskar MartinezNo ratings yet
- Case Report: A Rare Cause of Upper Airway Obstruction in A ChildDocument4 pagesCase Report: A Rare Cause of Upper Airway Obstruction in A Childpagar bersihNo ratings yet
- PPK Bedah Luka BakarDocument7 pagesPPK Bedah Luka BakarBellaNo ratings yet
- TracheostomyDocument4 pagesTracheostomymindreader19No ratings yet
- ManagingAirwayObstruction PDFDocument5 pagesManagingAirwayObstruction PDFMeyNo ratings yet
- Hobai 2012Document22 pagesHobai 2012CristianpalmarNo ratings yet
- Tracheal StenosisDocument4 pagesTracheal StenosisJessica MarianoNo ratings yet
- Tracheostomy in Icu: Who Should Do It ? The Surgeon or The Anesthesiologist ?Document45 pagesTracheostomy in Icu: Who Should Do It ? The Surgeon or The Anesthesiologist ?Cristina PironNo ratings yet
- Advanced Upper Airway Obstruction in ENT Surgery: Leanne Rees FRCA Rosemary A. Mason FRCADocument5 pagesAdvanced Upper Airway Obstruction in ENT Surgery: Leanne Rees FRCA Rosemary A. Mason FRCARatna WindyaningrumNo ratings yet
- Tracheostomy in IcuDocument45 pagesTracheostomy in IcuCarmen IulianaNo ratings yet
- Reirradiation Meta Analysis and Systematic ReviewDocument13 pagesReirradiation Meta Analysis and Systematic ReviewGiovanni HenryNo ratings yet
- Paediatric Neck MassesDocument7 pagesPaediatric Neck MassesGiovanni HenryNo ratings yet
- Endoscopic Sinus SurgeryDocument91 pagesEndoscopic Sinus SurgeryGiovanni HenryNo ratings yet
- Anterior Pharyngeal PouchDocument4 pagesAnterior Pharyngeal PouchGiovanni HenryNo ratings yet
- Evaluation of The Dizzy PatientDocument61 pagesEvaluation of The Dizzy PatientGiovanni HenryNo ratings yet
- Clinical Features of Ramsay Hunt Syndrome.: C J Sweeney, and D H Gilden J Neurol Neurosurg Psychiatry 2001 71:149-154Document1 pageClinical Features of Ramsay Hunt Syndrome.: C J Sweeney, and D H Gilden J Neurol Neurosurg Psychiatry 2001 71:149-154Giovanni HenryNo ratings yet
- April 2018 Recalls - Reda: Embolectomy??)Document5 pagesApril 2018 Recalls - Reda: Embolectomy??)Giovanni HenryNo ratings yet
- DNB Gen Surgery Old Question Papers 1Document28 pagesDNB Gen Surgery Old Question Papers 1sidorai100% (1)
- September 2020 Recalls Scorpio and Al Beruni 243 QuestionsDocument9 pagesSeptember 2020 Recalls Scorpio and Al Beruni 243 QuestionsGiovanni HenryNo ratings yet
- April 2018 IMRCS A Exam ReviewDocument12 pagesApril 2018 IMRCS A Exam Reviewmobz00No ratings yet
- DNB Gen Surgery Old Question Papers 1Document28 pagesDNB Gen Surgery Old Question Papers 1sidorai100% (1)
- Surgical AnatomyDocument4 pagesSurgical AnatomyGiovanni HenryNo ratings yet
- General Surgery June 2010: Paper IDocument2 pagesGeneral Surgery June 2010: Paper IGiovanni HenryNo ratings yet
- Transplantation: Leo-Paul Powell DM Tutorial Series March 30, 2021Document45 pagesTransplantation: Leo-Paul Powell DM Tutorial Series March 30, 2021Giovanni HenryNo ratings yet
- The Physiology of Human DefecationDocument21 pagesThe Physiology of Human Defecationyohanna yohannaNo ratings yet
- Endothelium I: Atherogenesis: Maintenance of Vascular HomeostasisDocument5 pagesEndothelium I: Atherogenesis: Maintenance of Vascular HomeostasisGiovanni HenryNo ratings yet
- Frcs Viva TOPICSDocument4 pagesFrcs Viva TOPICSGiovanni HenryNo ratings yet
- Gen Surg 1996 2009Document26 pagesGen Surg 1996 2009LijoeliyasNo ratings yet
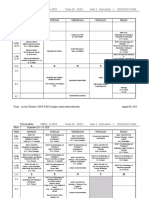
- Class of 2023 Year 1 Sem 1 Final Aug 30Document16 pagesClass of 2023 Year 1 Sem 1 Final Aug 30Giovanni HenryNo ratings yet
- EVAR vs. Open Repair - EvidenceDocument5 pagesEVAR vs. Open Repair - EvidenceGiovanni HenryNo ratings yet
- Colon & Rectum Questions Aug 2008Document61 pagesColon & Rectum Questions Aug 2008Dr.mesho Bin MansourNo ratings yet
- NS Camp 2012 - Health History Form For HTsDocument1 pageNS Camp 2012 - Health History Form For HTsThanhThao NguyenNo ratings yet
- Tracheostomies: The Complete Guide - Dr. Linda Morris, PHD, APN, CCNS, Dr. M. Sherif Afifi, MD, FCCMDocument1 pageTracheostomies: The Complete Guide - Dr. Linda Morris, PHD, APN, CCNS, Dr. M. Sherif Afifi, MD, FCCMpratiwiNo ratings yet
- Glandular Cystitis - A Rare Benign Condition Presenting As A Pseudo-Tumor of The BladderDocument3 pagesGlandular Cystitis - A Rare Benign Condition Presenting As A Pseudo-Tumor of The BladderRahmamagerNo ratings yet
- Radiology 2Document15 pagesRadiology 2Alonso GuardadoNo ratings yet
- Newborn Care Charts Guide Routine Care and ManagementDocument102 pagesNewborn Care Charts Guide Routine Care and ManagementM. KurnNo ratings yet
- Time Pressure Management As A Compensatory Strategy Training After Closed Head InjuryDocument20 pagesTime Pressure Management As A Compensatory Strategy Training After Closed Head InjuryMarta SanchezNo ratings yet
- Case Study FormatDocument3 pagesCase Study FormatPeter John CaballejosNo ratings yet
- Tranquilizers IN Wild AnimalsDocument23 pagesTranquilizers IN Wild AnimalsAsif AliNo ratings yet
- DR Ahmed Abar CVDocument7 pagesDR Ahmed Abar CVAnonymous H1EZvy1yQNo ratings yet
- Rguhs Thesis Topics in PeriodonticsDocument5 pagesRguhs Thesis Topics in PeriodonticsSara Perez100% (2)
- Effects of Thamboolam (Betel Leaf) ChewingDocument12 pagesEffects of Thamboolam (Betel Leaf) ChewingkpugazhNo ratings yet
- Final Solicitation LetterDocument2 pagesFinal Solicitation LetterBrian Jobim TanNo ratings yet
- Methods in Human Growth ResearchDocument414 pagesMethods in Human Growth ResearchSvarta BergetNo ratings yet
- GCSE Biology RevisionDocument2 pagesGCSE Biology RevisionsannnnnNo ratings yet
- Formulation and Evaluation of Solid Self Micro Emulsifying Drug Delivery System Using Aerosil 200 As Solid CarrierDocument6 pagesFormulation and Evaluation of Solid Self Micro Emulsifying Drug Delivery System Using Aerosil 200 As Solid CarriermorganvilleNo ratings yet
- Sle Report NotesDocument3 pagesSle Report NotesVane UcatNo ratings yet
- Blood Groups, Abo and RHDocument6 pagesBlood Groups, Abo and RHromeoenny4154No ratings yet
- Phenomenal Bombardment of Antibiotic in Poultry: Contemplating The Environmental RepercussionsDocument15 pagesPhenomenal Bombardment of Antibiotic in Poultry: Contemplating The Environmental RepercussionsCrislyn Akilit BayawaNo ratings yet
- VALDEZ, Gail-Marie R. Eaec-3 Yr. Psychiatric Assessment and Mental Status Exam General DataDocument8 pagesVALDEZ, Gail-Marie R. Eaec-3 Yr. Psychiatric Assessment and Mental Status Exam General DatabochoiNo ratings yet