You might also like
- POLYHYDRAMNIOSDocument4 pagesPOLYHYDRAMNIOSmohammed alkanani100% (1)
- Polyhydramnios 10Document4 pagesPolyhydramnios 10hussain AltaherNo ratings yet
- Definition of Premature Rapture of Membrane (Document3 pagesDefinition of Premature Rapture of Membrane (Merly Grael LigligenNo ratings yet
- Managing Pica, Polyhydramnios, Oligohydramnios, and Hyperemesis GravidarumDocument29 pagesManaging Pica, Polyhydramnios, Oligohydramnios, and Hyperemesis GravidarumKyle Ethan De la RiarteNo ratings yet
- Amniotic Fluid and Placenta AbnormalitiesDocument60 pagesAmniotic Fluid and Placenta AbnormalitiesMicah Lou CalambaNo ratings yet
- 109Document3 pages109Angel MoncadaNo ratings yet
- POLYHYDRAMNIOSDocument2 pagesPOLYHYDRAMNIOSyxly imperialNo ratings yet
- NCMB 312 Finals! (2.0)Document25 pagesNCMB 312 Finals! (2.0)Justine Dinice MunozNo ratings yet
- NCMB 312 Finals! (2.0)Document25 pagesNCMB 312 Finals! (2.0)Justine Dinice MunozNo ratings yet
- ANC Teaching On Danger Signs of PregnancyDocument5 pagesANC Teaching On Danger Signs of Pregnancyjenisha sapkotaNo ratings yet
- AMENORRHOEADocument35 pagesAMENORRHOEAnyangaraNo ratings yet
- Amniotic Fluid Disoder: Muhammad IzzatDocument26 pagesAmniotic Fluid Disoder: Muhammad IzzatcopperNo ratings yet
- Gestational Conditions: Hyperemesis Gravidarum Is Severe and Unremitting Nausea or Vomiting Associated WithDocument13 pagesGestational Conditions: Hyperemesis Gravidarum Is Severe and Unremitting Nausea or Vomiting Associated WithApRil Anne BalanonNo ratings yet
- Hyper Emesis Gravidrum Lesson PlanDocument14 pagesHyper Emesis Gravidrum Lesson PlanNaresh JarwalNo ratings yet
- Managment of Pulmonary HTN NeonateDocument30 pagesManagment of Pulmonary HTN Neonatejihad mansourNo ratings yet
- Review NTS..NCM 109Document11 pagesReview NTS..NCM 109Celline Isabelle ReyesNo ratings yet
- 1.Mds Test FinalDocument48 pages1.Mds Test FinalSubhashNo ratings yet
- Emotional Support in The Immediate Post Partum 1. Taking PhaseDocument3 pagesEmotional Support in The Immediate Post Partum 1. Taking PhaseApRil Anne BalanonNo ratings yet
- Department of Prasuti Tantra and Striroga Dayanand Ayurvedic College, Jalandhar SESSION 2016-17Document40 pagesDepartment of Prasuti Tantra and Striroga Dayanand Ayurvedic College, Jalandhar SESSION 2016-17jyothiNo ratings yet
- AbortionDocument32 pagesAbortionmani_mandeep262519100% (1)
- Gynecology: 3.09 - AmenorrheaDocument13 pagesGynecology: 3.09 - AmenorrheaAnna Mae MarantanNo ratings yet
- Giardiasis dan Leismania: Morfologi, Gejala, Diagnosis dan PengobatanDocument39 pagesGiardiasis dan Leismania: Morfologi, Gejala, Diagnosis dan PengobatanSurya PradnyaNo ratings yet
- M5F - Introduction To Dental Management of Pregnant PatientsDocument12 pagesM5F - Introduction To Dental Management of Pregnant PatientsBea YmsnNo ratings yet
- H.mole 2Document6 pagesH.mole 2cherry shane abanesNo ratings yet
- 4.1d - Pathology of The Pituitary - Nov.10 - Dr. GalangDocument4 pages4.1d - Pathology of The Pituitary - Nov.10 - Dr. GalangMiel Raphael AranillaNo ratings yet
- Prof. Ayman - GTDand GTN - NotesDocument34 pagesProf. Ayman - GTDand GTN - NotesThekra AlmosaedNo ratings yet
- Polyhydramnios & Oligohydramnios: Prepared By: Hamzah Qarawi To: Miss Mahdia KonyDocument37 pagesPolyhydramnios & Oligohydramnios: Prepared By: Hamzah Qarawi To: Miss Mahdia KonyNinaNo ratings yet
- Amniotic Fluid Abnorality PDF'Document31 pagesAmniotic Fluid Abnorality PDF'Aşna Rengîn0% (1)
- Teratology & Chronic PoisoningDocument54 pagesTeratology & Chronic PoisoningMadhu Sudhan PandeyaNo ratings yet
- OBII - 16 Postterm Pregnancy - PDF Version 1Document6 pagesOBII - 16 Postterm Pregnancy - PDF Version 1Felina CabadingNo ratings yet
- SRM COLLEGE PHYSIOTHERAPY TERATOGENESISDocument24 pagesSRM COLLEGE PHYSIOTHERAPY TERATOGENESISPONMATHI P FACULTY OF PHYSIOTHERAPYNo ratings yet
- Abnormalities of Amniotic FluidDocument27 pagesAbnormalities of Amniotic FluidRukmini kakatikar0% (1)
- 6 Endometrial Polyp - Libre PathologyDocument4 pages6 Endometrial Polyp - Libre PathologyfadoNo ratings yet
- LESSON PLAN ON Hyper Emesis GravidarumDocument12 pagesLESSON PLAN ON Hyper Emesis GravidarumMadhavi ModaNo ratings yet
- GYNE 4.06-Benign and Malignant Lesions of UterusDocument7 pagesGYNE 4.06-Benign and Malignant Lesions of UterusGray SnellNo ratings yet
- Amniotic FluidDocument7 pagesAmniotic FluidCherralaine CorderoNo ratings yet
- It Is Caused By:: Definition of TyphusDocument2 pagesIt Is Caused By:: Definition of TyphusAshima Viie BassamahNo ratings yet
- Post Partum Haemorrhage 1 - LoadDocument47 pagesPost Partum Haemorrhage 1 - Loadkalpananstl100% (1)
- Antepartum Hemorrhage CausesDocument9 pagesAntepartum Hemorrhage CausesadiNo ratings yet
- Micro TaechingDocument11 pagesMicro Taechingupma sharmaNo ratings yet
- Polyhydramnious and oligohydramnious: Causes, effects and managementDocument34 pagesPolyhydramnious and oligohydramnious: Causes, effects and managementEdward Munyaradzi KutsanziraNo ratings yet
- Early Pregnancy Loss CausesDocument23 pagesEarly Pregnancy Loss CausesDianne GalangNo ratings yet
- Poly and OligoDocument26 pagesPoly and OligoMAD Bl00DNo ratings yet
- Obstetrics - Abnormalities of The Amniotic FluidDocument6 pagesObstetrics - Abnormalities of The Amniotic FluidJonathanNo ratings yet
- Pregnancy Dermatosis GuideDocument87 pagesPregnancy Dermatosis Guidemohankumar sowmiyaNo ratings yet
- OBG Picture Based Discussion 01Document48 pagesOBG Picture Based Discussion 01Dheeraj Nandal0% (1)
- Prematurely Ruptured of Membranes (PROM)Document23 pagesPrematurely Ruptured of Membranes (PROM)NiNie Sie MbakayuNeNo ratings yet
- Upper Airway ObstructionDocument14 pagesUpper Airway ObstructionAnantaBenvenuto100% (1)
- MULTIPLE PREGNANCY: Types, Risks & CareDocument54 pagesMULTIPLE PREGNANCY: Types, Risks & CarerizmaNo ratings yet
- Common Complications of PregnancyDocument34 pagesCommon Complications of PregnancyiwennieNo ratings yet
- Dermatological Disorders Unique To Pregnancy: January 2009Document14 pagesDermatological Disorders Unique To Pregnancy: January 2009mutmainnahNo ratings yet
- Materi Dr. Muryanto - HemoroidsDocument20 pagesMateri Dr. Muryanto - HemoroidsAndria SaputraNo ratings yet
- Copy of pharma reviewerDocument9 pagesCopy of pharma reviewerLyra Penelope OliquinoNo ratings yet
- Disorders of Amniotic Fluid and Placental AbnormalitiesDocument60 pagesDisorders of Amniotic Fluid and Placental AbnormalitiesMonique BorresNo ratings yet
- Abnormalities of Amniotic Fluid: Presented by Ms. K.D. Sharon Final Year MSC (N) Obstetrics and Gynaecology NursingDocument32 pagesAbnormalities of Amniotic Fluid: Presented by Ms. K.D. Sharon Final Year MSC (N) Obstetrics and Gynaecology Nursingkalla sharonNo ratings yet
- Chapter%2B5%2BAmenorrhoeaDocument7 pagesChapter%2B5%2BAmenorrhoeapmj050gpNo ratings yet
- Handout 4Document13 pagesHandout 4ApRil Anne BalanonNo ratings yet
- 14 - AmenorrhoeaDocument26 pages14 - AmenorrhoeaHimanshu MehtaNo ratings yet
- Simulation San SeminarDocument6 pagesSimulation San SeminarDeepika PatidarNo ratings yet
- Teaching Methods and Evaluation in Family PlanningDocument9 pagesTeaching Methods and Evaluation in Family PlanningDeepika PatidarNo ratings yet
- FIRST STAGE of LABOUREVENTSDocument91 pagesFIRST STAGE of LABOUREVENTSDeepika PatidarNo ratings yet
- Urvi A.V. Aids FileDocument47 pagesUrvi A.V. Aids FileDeepika PatidarNo ratings yet
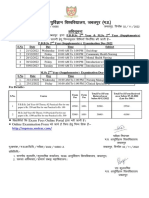
- PBBSC-MSC 2Y (Supply) Time Table (Dec 2022)Document4 pagesPBBSC-MSC 2Y (Supply) Time Table (Dec 2022)Deepika PatidarNo ratings yet
- Positioning and Its ImportanceDocument22 pagesPositioning and Its ImportanceDeepika PatidarNo ratings yet
- Physiological Jaundice Baby PoojaDocument17 pagesPhysiological Jaundice Baby PoojaDeepika PatidarNo ratings yet
- Health Talk Om Antenatal ExerciseDocument10 pagesHealth Talk Om Antenatal ExerciseDeepika PatidarNo ratings yet
- Seminar On Distance Education JKDocument6 pagesSeminar On Distance Education JKDeepika PatidarNo ratings yet
- Alternative and Complemntry TheoryDocument18 pagesAlternative and Complemntry TheoryDeepika PatidarNo ratings yet
- Demo AntenatalDocument26 pagesDemo AntenatalDeepika PatidarNo ratings yet
- Lesson Plan PositionDocument4 pagesLesson Plan PositionDeepika PatidarNo ratings yet
- Celecoxib Identification MethodsDocument5 pagesCelecoxib Identification Methodsabc1679No ratings yet
- Berca Engineering SUBMITTEDDocument20 pagesBerca Engineering SUBMITTEDJohandika FerbiantokoNo ratings yet
- A 1116Document15 pagesA 1116Rama S. SinghNo ratings yet
- Fermentation Technology for Food Preservation and ProcessingDocument47 pagesFermentation Technology for Food Preservation and ProcessingAhmad Syamil Muhamad ZinNo ratings yet
- Symbol High Low R5 R4 R3 R2: DailyDocument8 pagesSymbol High Low R5 R4 R3 R2: Daily257597 rmp.mech.16No ratings yet
- FarkolDocument7 pagesFarkolHasiadin LaodeNo ratings yet
- Smoke Stratification - Understanding the DynamicsDocument3 pagesSmoke Stratification - Understanding the DynamicsGagan UpadhyayNo ratings yet
- CH 2Document20 pagesCH 2Vivek SinghNo ratings yet
- GMP TD Ar FPL 11033Document1 pageGMP TD Ar FPL 11033Sammy NguyenNo ratings yet
- Appendix VIII - Civil and Structural Scope of WorkDocument140 pagesAppendix VIII - Civil and Structural Scope of WorkjaganrajNo ratings yet
- STM - Merck Case AnswersDocument2 pagesSTM - Merck Case AnswersreetayanNo ratings yet
- Development Team: Analytical Chemistry PolarographyDocument18 pagesDevelopment Team: Analytical Chemistry PolarographyKanchanNo ratings yet
- 85 HP John Deere 4045DFM50 Marine Diesel EngineDocument2 pages85 HP John Deere 4045DFM50 Marine Diesel EngineDAVIDNo ratings yet
- Hector: Genuine AccessoriesDocument18 pagesHector: Genuine AccessoriesssgfdfgNo ratings yet
- Accessibility POC: October 26, 2017Document7 pagesAccessibility POC: October 26, 2017Ramesh BodukaniNo ratings yet
- REBA Employee Assessment Worksheet: A. Neck, Trunk and Leg AnalysisDocument1 pageREBA Employee Assessment Worksheet: A. Neck, Trunk and Leg AnalysisAgni JayantiNo ratings yet
- Information Security Management System: Gheorghe MirelaDocument6 pagesInformation Security Management System: Gheorghe MirelaChristen CastilloNo ratings yet
- 1978 - 90 Day Study or Rhesus Monkey ToxicityDocument4 pages1978 - 90 Day Study or Rhesus Monkey Toxicitygrace poudrierNo ratings yet
- PCOS Diet Cookbook For Newly Diagnosed IndividualsDocument67 pagesPCOS Diet Cookbook For Newly Diagnosed Individualsmavendave4lifeNo ratings yet
- Deliver VALUE and RENEWABLE FUTUREDocument30 pagesDeliver VALUE and RENEWABLE FUTUREAlexandru SuciuNo ratings yet
- Better - Call - Saul - 4x10 WINNERDocument70 pagesBetter - Call - Saul - 4x10 WINNERMarcos Valdés GarridoNo ratings yet
- IED Recognition GuideDocument28 pagesIED Recognition GuideLeafs61100% (5)
- Cambridge BiologyDocument78 pagesCambridge BiologyBraweet SapkotaNo ratings yet
- Alpine Valley Liability ReleaseDocument1 pageAlpine Valley Liability ReleaseChristina Nakazaki0% (1)
- MFT28 - Greg Plitt's 4-Week Military Fitness Trainer by MET-RxDocument7 pagesMFT28 - Greg Plitt's 4-Week Military Fitness Trainer by MET-RxRayNo ratings yet
- Commercial Law Review Midterm - Without AnswersDocument1 pageCommercial Law Review Midterm - Without AnswersTorni JoNo ratings yet
- Compabloc Heat Exchangers Cut Downtime at Nynäs RefineryDocument2 pagesCompabloc Heat Exchangers Cut Downtime at Nynäs RefinerylaythNo ratings yet
- Sydney M PRPDocument23 pagesSydney M PRPapi-465406877No ratings yet
- Holy Names vs. Franklin SwimmingDocument3 pagesHoly Names vs. Franklin SwimmingstprepsNo ratings yet