You might also like
- Reflexology EssentialDocument79 pagesReflexology EssentialMM Nabeel100% (2)
- Post Traumatic Stress Disorder (PTSD)Document114 pagesPost Traumatic Stress Disorder (PTSD)Gugus EkaNo ratings yet
- O Level Biology Practice Questions And Answers Transport In HumanFrom EverandO Level Biology Practice Questions And Answers Transport In HumanNo ratings yet
- Medical Information FormDocument2 pagesMedical Information FormNot yet SenseNo ratings yet
- CD-42 - Medical QuestionnaireDocument6 pagesCD-42 - Medical QuestionnaireRasLDKNo ratings yet
- Physical Fitness CertificateDocument1 pagePhysical Fitness CertificateDilip SenthNo ratings yet
- Malaria Treatment TableDocument9 pagesMalaria Treatment Tableاحمد عرفاتNo ratings yet
- Medical FormDocument4 pagesMedical FormSujata DeviNo ratings yet
- Peripheral Intravenous Cannulation PolicyDocument14 pagesPeripheral Intravenous Cannulation PolicyRoksana AkhterNo ratings yet
- Dental Orthodontics MCQsDocument23 pagesDental Orthodontics MCQsSuraj RaiNo ratings yet
- Food Safety CultureDocument9 pagesFood Safety CultureSimone BalianNo ratings yet
- Product Name: Heartbeat - Product UIN: MAXHLIP20065V051920Document61 pagesProduct Name: Heartbeat - Product UIN: MAXHLIP20065V051920RekhaNo ratings yet
- Penology Reviewer QuestionnaireDocument35 pagesPenology Reviewer QuestionnaireLowell De Los Reyes100% (1)
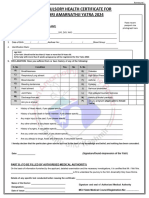
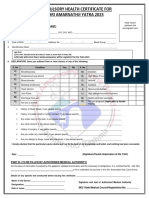
- Compulsory Heal TH Certificate For Shri Amarna Thji Ya Tra 2023Document1 pageCompulsory Heal TH Certificate For Shri Amarna Thji Ya Tra 2023Eknath KoliNo ratings yet
- Critical Illness (Heart) - Statement of Medical ExaminerDocument2 pagesCritical Illness (Heart) - Statement of Medical ExaminerUstazFaizalAriffinOriginalNo ratings yet
- Pre-Exercise Screening Form: 1.personal DetailsDocument4 pagesPre-Exercise Screening Form: 1.personal DetailsLee TarrozaNo ratings yet
- HD FormatDocument4 pagesHD FormatSaravana KumarNo ratings yet
- Medical Fitness Certificate For TrekkersDocument1 pageMedical Fitness Certificate For TrekkersRajatChadhaNo ratings yet
- English CHCDocument1 pageEnglish CHCBhupi AgrawalNo ratings yet
- AutoRecovery Save of Revised MEDICAL EXAMINATION REPORTDocument3 pagesAutoRecovery Save of Revised MEDICAL EXAMINATION REPORTFred mungaNo ratings yet
- CHCAndApplicationForm2022 1 2Document2 pagesCHCAndApplicationForm2022 1 2sawant.httpNo ratings yet
- Amarnath Yatra Compulsory Health Certificate 2017Document1 pageAmarnath Yatra Compulsory Health Certificate 2017Sneha KerkarNo ratings yet
- Medical Tasac New - Iso - 1Document11 pagesMedical Tasac New - Iso - 1Mustafa JumaNo ratings yet
- MedicalDocument2 pagesMedicalOseghale MichaelNo ratings yet
- Application Form and CHC Form For Yatra 2021Document2 pagesApplication Form and CHC Form For Yatra 2021nitishNo ratings yet
- Borang Pemeriksaan KesihatanDocument4 pagesBorang Pemeriksaan KesihatanMan DenzoNo ratings yet
- Annexure II Compulsory Health Certificate For Kumbh Mela Haridwar - 2021Document1 pageAnnexure II Compulsory Health Certificate For Kumbh Mela Haridwar - 2021Shrasti SoniNo ratings yet
- Medical Clearance FormDocument2 pagesMedical Clearance FormPhake CodedNo ratings yet
- Form4 COPDocument3 pagesForm4 COPAdarsh RaghuwanshiNo ratings yet
- Circular 07Document2 pagesCircular 07Eliyas AlamNo ratings yet
- Medical ReportDocument2 pagesMedical ReportwildanmuhammadnajmiNo ratings yet
- Protocol BluebookDocument16 pagesProtocol BluebookItz D LifeNo ratings yet
- Compulsory Health Certificate For Shri Amarnathji Yatra 2023Document1 pageCompulsory Health Certificate For Shri Amarnathji Yatra 2023Eknath KoliNo ratings yet
- Medical Board Format 2015Document6 pagesMedical Board Format 2015hemantaduttaghy1No ratings yet
- Medical Examination - FormDocument3 pagesMedical Examination - FormVivek KumarNo ratings yet
- Health Questionnaire - Occupational HealthDocument3 pagesHealth Questionnaire - Occupational HealthRJay JacabanNo ratings yet
- Proforma For Medical CertificateDocument2 pagesProforma For Medical CertificateGagan PrasadNo ratings yet
- Pre-Anaesthetic Self Assessment FormDocument2 pagesPre-Anaesthetic Self Assessment FormmmmmNo ratings yet
- TN TRA Blood Donor QuestionnaireDocument2 pagesTN TRA Blood Donor QuestionnaireEman KarisNo ratings yet
- 14.05 Eurojam-Health Sheet GB FRDocument3 pages14.05 Eurojam-Health Sheet GB FRZanfir MihailNo ratings yet
- To Be Completed by The Applicant: Coronavirus (Sars-Cov-2) Infection QuestionnaireDocument2 pagesTo Be Completed by The Applicant: Coronavirus (Sars-Cov-2) Infection Questionnairecky7vyfv48No ratings yet
- Medical Form DeborahDocument3 pagesMedical Form Deborahwakermarine16No ratings yet
- Physical Examination CertificateDocument3 pagesPhysical Examination CertificateHira DamayantiNo ratings yet
- TYPED-medical SoftDocument5 pagesTYPED-medical SoftynrajambaNo ratings yet
- Blood Donation Application FormDocument2 pagesBlood Donation Application FormFadjar MulyaNo ratings yet
- Death Form - 0001Document1 pageDeath Form - 0001mordhwajsingh.jat76No ratings yet
- Non Medical QuestionaireDocument2 pagesNon Medical QuestionaireLoveth EkwegbaraNo ratings yet
- CHC Updated 2023Document1 pageCHC Updated 2023maheshmonu9449No ratings yet
- CHC Updated 2023Document1 pageCHC Updated 2023Vishal Singh ShekhawatNo ratings yet
- Health Fitness Certificate For The Purposes of Permission To Work in Confined SpaceDocument6 pagesHealth Fitness Certificate For The Purposes of Permission To Work in Confined SpaceNur ShaNo ratings yet
- Medical CertificateDocument4 pagesMedical CertificateRishi ScifreakNo ratings yet
- Physical Fitness CertificateDocument1 pagePhysical Fitness CertificateVijendra RNo ratings yet
- Historia Salud INGLESDocument2 pagesHistoria Salud INGLESjaferloNo ratings yet
- Travel Questionnaire For PatientsDocument2 pagesTravel Questionnaire For PatientsVineet ShettyNo ratings yet
- FICHES METHODE ANGLAIS FR VocabulaireDocument63 pagesFICHES METHODE ANGLAIS FR Vocabulairehajar razikNo ratings yet
- Targeted Patient Safety QuestionnairesDocument27 pagesTargeted Patient Safety QuestionnairesAafreen KhairNo ratings yet
- Health FormDocument3 pagesHealth FormkrissramNo ratings yet
- HKCAD Medical Report FormDocument4 pagesHKCAD Medical Report FormHelloWorldNo ratings yet
- College of Applied Medical Sciences Nursing Department Nursing Care Plan 5%Document4 pagesCollege of Applied Medical Sciences Nursing Department Nursing Care Plan 5%Ghadah AlfahadNo ratings yet
- Model of Maritime Declaration of Health: Annex 8Document1 pageModel of Maritime Declaration of Health: Annex 8Dian Pratiwi AkbarNo ratings yet
- Patient Packet OnlineDocument11 pagesPatient Packet OnlineSt Terri WulfeNo ratings yet
- 3.medical FormDocument5 pages3.medical Formamistudio30No ratings yet
- M.ramadhani - Askep Batu EmpeduDocument12 pagesM.ramadhani - Askep Batu EmpeduPingky BoyNo ratings yet
- Proforma Age Estimation PDFDocument3 pagesProforma Age Estimation PDFYogitaNo ratings yet
- Short Cases Phase 1Document56 pagesShort Cases Phase 1Sanjaya WijesekaraNo ratings yet
- Wellness Check Questionnaire Updated 2023Document5 pagesWellness Check Questionnaire Updated 2023Matthew TivNo ratings yet
- D. Offering To Do Something.: A. Have Just LostDocument9 pagesD. Offering To Do Something.: A. Have Just LostRauf PriantamaNo ratings yet
- Study Guide Lecture Exam 1 Use This Handout With Your Video Review Possible Essay QuestionsDocument4 pagesStudy Guide Lecture Exam 1 Use This Handout With Your Video Review Possible Essay QuestionsBrandice BradleyNo ratings yet
- Impaired Tissue PerfusionDocument2 pagesImpaired Tissue PerfusionLeo Mar MakilanNo ratings yet
- Asbestos Contamination in Talc-Based Cosmetics: An Invisible Cancer RiskDocument3 pagesAsbestos Contamination in Talc-Based Cosmetics: An Invisible Cancer RiskAlexia GonzalezNo ratings yet
- Dam-It, It's Easy: Handbook of Basic Dental Dam ProceduresDocument32 pagesDam-It, It's Easy: Handbook of Basic Dental Dam ProceduresNonoNo ratings yet
- TETRINDocument2 pagesTETRINDr.2020No ratings yet
- 1 - Kanno - J Oral Rehab - 2006 CópiaDocument13 pages1 - Kanno - J Oral Rehab - 2006 CópiaYvelisse LoraNo ratings yet
- The Endocrine SystemDocument7 pagesThe Endocrine SystemRODGIELYN MAE GEJONNo ratings yet
- Brochure 6th World Congress On Polycystic Ovarian SyndromeDocument11 pagesBrochure 6th World Congress On Polycystic Ovarian Syndromemegan scottNo ratings yet
- Gum PaintDocument3 pagesGum PaintAni GuptaNo ratings yet
- TPN For EE Short Time ReviewDocument1,376 pagesTPN For EE Short Time ReviewDivine Borja100% (1)
- Advanced Writing Note For StudentsDocument27 pagesAdvanced Writing Note For StudentsRADEAT GETIYENo ratings yet
- Ventricular Tachycardia Storm Management in ADocument6 pagesVentricular Tachycardia Storm Management in Aselandia nisrinaNo ratings yet
- Plantar Fasciitis: What Is The Plantar Fasciae?Document6 pagesPlantar Fasciitis: What Is The Plantar Fasciae?mattamooreNo ratings yet
- Dental HygieneDocument3 pagesDental Hygieneapi-507354264No ratings yet
- General Topic: Fun Facts About HorsesDocument5 pagesGeneral Topic: Fun Facts About HorsesLittle SleepybirdNo ratings yet
- First AidDocument10 pagesFirst AidSanthiya venkadesanNo ratings yet
- The Relationship Between Social Support and Psychological Problems AmongDocument8 pagesThe Relationship Between Social Support and Psychological Problems Amongltomic_1No ratings yet
- Jurnal Infeksi Saluran PencernaanDocument22 pagesJurnal Infeksi Saluran PencernaanDini Okta PutriNo ratings yet
- Slipped Capital Femoral Epiphysis (Scfe)Document27 pagesSlipped Capital Femoral Epiphysis (Scfe)Mariam AntonyNo ratings yet
- Ventricular Tachycardia Bsn3b-Grp1Document35 pagesVentricular Tachycardia Bsn3b-Grp1Jessica RamosNo ratings yet
- What Is Hypovolemic ShockDocument4 pagesWhat Is Hypovolemic ShockDukittyNo ratings yet