You might also like
- Pre Medical Examination Format (MER Form)Document5 pagesPre Medical Examination Format (MER Form)soham67% (3)
- HonorDishonorProcess - Victoria Joy-1 PDFDocument126 pagesHonorDishonorProcess - Victoria Joy-1 PDFarjay1266100% (3)
- Migrant Health FormDocument5 pagesMigrant Health FormImelda Junaedi100% (3)
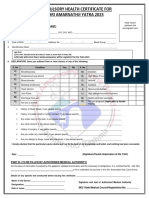
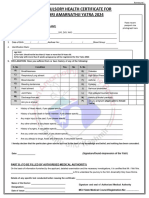
- Compulsory Health Certificate for Amarnath YatraDocument1 pageCompulsory Health Certificate for Amarnath YatraEknath KoliNo ratings yet
- HEALTHY PILGRIMAGEDocument1 pageHEALTHY PILGRIMAGEEknath KoliNo ratings yet
- CHC Updated 2023Document1 pageCHC Updated 2023maheshmonu9449No ratings yet
- CHC Updated 2023Document1 pageCHC Updated 2023Vishal Singh ShekhawatNo ratings yet
- English CHCDocument1 pageEnglish CHCBhupi AgrawalNo ratings yet
- Amarnath Yatra Compulsory Health Certificate 2017Document1 pageAmarnath Yatra Compulsory Health Certificate 2017Sneha KerkarNo ratings yet
- Medical Fitness Certificate For TrekkersDocument1 pageMedical Fitness Certificate For TrekkersRajatChadhaNo ratings yet
- Application Form and CHC Form For Yatra 2021Document2 pagesApplication Form and CHC Form For Yatra 2021nitishNo ratings yet
- CHCAndApplicationForm2022 1 2Document2 pagesCHCAndApplicationForm2022 1 2sawant.httpNo ratings yet
- Annexure II Compulsory Health Certificate For Kumbh Mela Haridwar - 2021Document1 pageAnnexure II Compulsory Health Certificate For Kumbh Mela Haridwar - 2021Shrasti SoniNo ratings yet
- Medical Fitness FormDocument1 pageMedical Fitness FormvickyreddyNo ratings yet
- ICICI Prudential Life Insurance Co LTD - Attachment - 6Document2 pagesICICI Prudential Life Insurance Co LTD - Attachment - 6vermalabNo ratings yet
- Compulsory Health Certificate For Shri Amarnathji Yatra 2014Document1 pageCompulsory Health Certificate For Shri Amarnathji Yatra 2014gsekar74No ratings yet
- Form G Health Examination Report International StudentDocument6 pagesForm G Health Examination Report International StudentVictor OjukwuNo ratings yet
- Kolej Teknologi Darulnaim: Darulnaim College of TechnologyDocument5 pagesKolej Teknologi Darulnaim: Darulnaim College of TechnologyDaryanto SutejiNo ratings yet
- FormatDocument3 pagesFormatchiragNo ratings yet
- D ReportDocument2 pagesD ReportHihiNo ratings yet
- Medical Certificate of Fitness: To Be Filled by CandidateDocument2 pagesMedical Certificate of Fitness: To Be Filled by CandidatevenkatNo ratings yet
- General Questions NO YESDocument5 pagesGeneral Questions NO YESChristian James PACILANNo ratings yet
- Medical Certificate of FitnessDocument2 pagesMedical Certificate of FitnessDINESH CHANDRA GANNAVARAPUNo ratings yet
- DR Langford1Document8 pagesDR Langford1Spencer JacksonNo ratings yet
- Guidelines To Fill in Health Examination ReportDocument6 pagesGuidelines To Fill in Health Examination ReportNurman HidayatNo ratings yet
- Libro ComplementarioDocument155 pagesLibro ComplementarioKowe xDNo ratings yet
- Apgenco 2012 Certificate of Fitness 22032012Document2 pagesApgenco 2012 Certificate of Fitness 22032012Veera ChaitanyaNo ratings yet
- Latihan MTK Un SMP BahasDocument2 pagesLatihan MTK Un SMP Bahasdinas pertanianNo ratings yet
- GPL Pre Employment Medical Examination Form - Draft - 08.09.2018Document1 pageGPL Pre Employment Medical Examination Form - Draft - 08.09.2018almamunmolla96No ratings yet
- Medical ReportDocument1 pageMedical Reportwhit.ehouseboyquantiumNo ratings yet
- Pre-Anaesthetic Self Assessment FormDocument2 pagesPre-Anaesthetic Self Assessment FormmmmmNo ratings yet
- Forrm 4aDocument4 pagesForrm 4aJ.L. Jumbo XeroxNo ratings yet
- Pediatrician Report: Questions Relating To Proposed InsuredDocument2 pagesPediatrician Report: Questions Relating To Proposed InsuredSincerely ReynNo ratings yet
- Adobe Scan 03 Jun 2023Document1 pageAdobe Scan 03 Jun 2023Gaurav SinghNo ratings yet
- Ramachandran Medical Application FormDocument3 pagesRamachandran Medical Application FormRuban JebaduraiNo ratings yet
- GPMRDocument5 pagesGPMRwisdom hameloNo ratings yet
- Medical Examination: Subang Polyclinic SDN BHDDocument5 pagesMedical Examination: Subang Polyclinic SDN BHDSubang polylinicNo ratings yet
- Request for Cashless HospitalisationDocument1 pageRequest for Cashless Hospitalisationjigerpanchal0% (1)
- Medical DecDocument4 pagesMedical DecSoumya ranjan HatiNo ratings yet
- WWW - Csc.gov - PH: Additional RequirementsDocument4 pagesWWW - Csc.gov - PH: Additional RequirementsMaria JessaNo ratings yet
- Pre Employment Medical Declaration Form - 2022Document2 pagesPre Employment Medical Declaration Form - 2022Neel GhoshNo ratings yet
- Physical FitnessDocument2 pagesPhysical FitnessRaj UshamollaNo ratings yet
- Fitness Form & Hospital ListDocument24 pagesFitness Form & Hospital ListAbhijeetMhatreNo ratings yet
- Pre-Employment Medical ExamDocument4 pagesPre-Employment Medical ExamdrirajaNo ratings yet
- Health Certificate Provides Thorough Medical DetailsDocument2 pagesHealth Certificate Provides Thorough Medical DetailsAndré DomanskiNo ratings yet
- Certificate of Physical FitnessDocument2 pagesCertificate of Physical FitnessVijay KumarNo ratings yet
- Medical Fitness PDFDocument5 pagesMedical Fitness PDFVenkateshwara ReddyNo ratings yet
- Elem Sec Health CardsDocument17 pagesElem Sec Health CardsMary Grace CalipesNo ratings yet
- Great Eastern Life - Confidential Medical Certificate (Other Illnesses) - CLMLAMCODocument2 pagesGreat Eastern Life - Confidential Medical Certificate (Other Illnesses) - CLMLAMCOsimpoonNo ratings yet
- Borang Silat DoktorDocument2 pagesBorang Silat DoktorhafizNo ratings yet
- Oil and Natural Gas Corporation LTD Self Declaration On Medical StatusDocument4 pagesOil and Natural Gas Corporation LTD Self Declaration On Medical StatusDodiya NikunjNo ratings yet
- History Taking ENTDocument6 pagesHistory Taking ENTzaid.qadir.6No ratings yet
- Critical Illness ClaimDocument7 pagesCritical Illness ClaimIzzatt TazaliNo ratings yet
- Examination Form MedicalsDocument3 pagesExamination Form MedicalsPushpa SinghNo ratings yet
- Welcome To Orthopedics Care Center !Document2 pagesWelcome To Orthopedics Care Center !Ahmed M. RafatNo ratings yet
- Form PD1 Medical Examination ReportDocument9 pagesForm PD1 Medical Examination ReportSyazwi BaharuddinNo ratings yet
- Death Claim Form B EnglishDocument2 pagesDeath Claim Form B EnglishDeath Claim PHS HYDNo ratings yet
- Liver Disease Questionnaire For Proposed Insured/OwnerDocument2 pagesLiver Disease Questionnaire For Proposed Insured/OwnerSincerely ReynNo ratings yet
- One Step Med: General Medical Information Record Keeping ManualFrom EverandOne Step Med: General Medical Information Record Keeping ManualNo ratings yet
- Inflamed Aorta, (Aortitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandInflamed Aorta, (Aortitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Risk Factors For Developing Aortic Disease (Second Edition)From EverandRisk Factors For Developing Aortic Disease (Second Edition)No ratings yet
- RTR Piping Inspection GuideDocument17 pagesRTR Piping Inspection GuideFlorante NoblezaNo ratings yet
- Syllabus PTSV3Document21 pagesSyllabus PTSV3Pablito Quispe RuizNo ratings yet
- Trial BalanceDocument2 pagesTrial BalanceJoseph Bayo BasanNo ratings yet
- 2020.07.31 Marchese Declaration With ExhibitsDocument103 pages2020.07.31 Marchese Declaration With Exhibitsheather valenzuelaNo ratings yet
- Engagement LetterDocument1 pageEngagement LetterCrystal Jenn Balaba100% (1)
- Determination of Atenolol in Pharmaceutical Dosages by Fourier Transform Infrared Spectrometry (FTIR)Document11 pagesDetermination of Atenolol in Pharmaceutical Dosages by Fourier Transform Infrared Spectrometry (FTIR)Geovas GomezNo ratings yet
- B.Ed Syllabus NEW 2015-16 PDFDocument170 pagesB.Ed Syllabus NEW 2015-16 PDFVikas KuthadiNo ratings yet
- Multibody Simulation of A Freight Bogie With Friction DampersDocument10 pagesMultibody Simulation of A Freight Bogie With Friction DampersGermán GoñiNo ratings yet
- COR2-03 Admist The Mists and Coldest Frost PDFDocument16 pagesCOR2-03 Admist The Mists and Coldest Frost PDFLouis BachNo ratings yet
- Cheat Codes SkyrimDocument13 pagesCheat Codes SkyrimDerry RahmaNo ratings yet
- MIZAT PWHT Procedure Ensures Welded Joints Meet StandardsDocument9 pagesMIZAT PWHT Procedure Ensures Welded Joints Meet StandardsM. R. Shahnawaz KhanNo ratings yet
- Training Report On Machine LearningDocument27 pagesTraining Report On Machine LearningBhavesh yadavNo ratings yet
- Ap4955 PDFDocument4 pagesAp4955 PDFGilvan HenriqueNo ratings yet
- St. Francis de Sales Sr. Sec. School, Gangapur CityDocument12 pagesSt. Francis de Sales Sr. Sec. School, Gangapur CityArtificial GammerNo ratings yet
- 9284 - Technical Instruction Addenum 3 Corrigendum 2Document5 pages9284 - Technical Instruction Addenum 3 Corrigendum 2Bambang HerimantoNo ratings yet
- Consumer Behavior PP Chapter 4Document36 pagesConsumer Behavior PP Chapter 4tuongvyvyNo ratings yet
- DWDM Route Planning A4 WPDocument3 pagesDWDM Route Planning A4 WPChavara MatekweNo ratings yet
- V14 EngDocument8 pagesV14 EngJamil PavonNo ratings yet
- Coffee TestDocument6 pagesCoffee TestAmit Satyen RaviNo ratings yet
- Cubic Spline Tutorial v3Document6 pagesCubic Spline Tutorial v3Praveen SrivastavaNo ratings yet
- A Rail-To-Rail Constant Gain Buffered Op-Amp For Real Time Video ApplicationsDocument8 pagesA Rail-To-Rail Constant Gain Buffered Op-Amp For Real Time Video Applicationskvpk_vlsiNo ratings yet
- LTG 04 DD Unit 4 WorksheetsDocument2 pagesLTG 04 DD Unit 4 WorksheetsNguyễn Kim Ngọc Lớp 4DNo ratings yet
- Dedicated Teacher ResumeDocument2 pagesDedicated Teacher ResumeLei Pitallano ComboyNo ratings yet
- Tutorial Task 3 - A C P I WK 2Document8 pagesTutorial Task 3 - A C P I WK 2BM70621 Alya Zahirah Binti AziziNo ratings yet
- Year 12 Holiday Homework Term 3Document4 pagesYear 12 Holiday Homework Term 3Lucas GauciNo ratings yet
- Danbury BrochureDocument24 pagesDanbury BrochureQuique MartinNo ratings yet
- Mondstadt City of Freedom Travel GuideDocument10 pagesMondstadt City of Freedom Travel GuideShypackofcheetos100% (3)
- Safety Data Sheet: 1. Identification of The Substance/preparation and of The Company/undertakingDocument4 pagesSafety Data Sheet: 1. Identification of The Substance/preparation and of The Company/undertakingBalasubramanian AnanthNo ratings yet
- Effect of Upstream Dam Geometry On Peak Discharge During Overtopping Breach in Noncohesive Homogeneous Embankment Dams Implications For Tailings DamsDocument22 pagesEffect of Upstream Dam Geometry On Peak Discharge During Overtopping Breach in Noncohesive Homogeneous Embankment Dams Implications For Tailings DamsHelvecioNo ratings yet