You might also like
- Cimetidine Anti Cancer Drug Reverses Tumor Immunity - Jeffrey Dach MDDocument26 pagesCimetidine Anti Cancer Drug Reverses Tumor Immunity - Jeffrey Dach MDnepretipNo ratings yet
- Tumours of Skin: DR F Bhatti Pennine VTS Sept 08Document39 pagesTumours of Skin: DR F Bhatti Pennine VTS Sept 08pfxbkNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument22 pagesSee Full Prescribing Information For Complete Boxed WarningTracy PopeNo ratings yet
- Skintox Practiceguidelines EGFR SCCDocument17 pagesSkintox Practiceguidelines EGFR SCCFelpnilNo ratings yet
- Cervicogenic Headache1Document41 pagesCervicogenic Headache1Jeetendra Soni100% (1)
- ACNE SCAR Goodarzi2021Document7 pagesACNE SCAR Goodarzi2021Dr Dhanraj ChavanNo ratings yet
- Dermatology PDFDocument23 pagesDermatology PDFjonyNo ratings yet
- Ghid Anestezie Locala PDFDocument19 pagesGhid Anestezie Locala PDFanaNo ratings yet
- 7 Bleeding Disorders DR - AlaaDocument35 pages7 Bleeding Disorders DR - Alaaaj1998ajNo ratings yet
- Melanocytic TumorsDocument254 pagesMelanocytic TumorsmixandgoNo ratings yet
- Induction Ceremony Emcee ScriptDocument5 pagesInduction Ceremony Emcee Scriptyg love91% (11)
- Yeung H Et Al 2012. Patient Reported Reasons For The Discontinuation of Commonly Used Treatments For Moderate To Severe PsoriasisDocument9 pagesYeung H Et Al 2012. Patient Reported Reasons For The Discontinuation of Commonly Used Treatments For Moderate To Severe PsoriasisAndi MarsaliNo ratings yet
- Phototherapy For Dermatologic ConditionsDocument18 pagesPhototherapy For Dermatologic ConditionsSeth MosebyNo ratings yet
- Fast Facts: Dermatological Nursing: A practical guide on career pathwaysFrom EverandFast Facts: Dermatological Nursing: A practical guide on career pathwaysNo ratings yet
- Facial Fillers ComplicationsDocument12 pagesFacial Fillers ComplicationsLewis PiersNo ratings yet
- Aplied Anatomy BotoxDocument8 pagesAplied Anatomy BotoxYesuratnam DudduNo ratings yet
- Derm StuffDocument7 pagesDerm StuffSudesna Roy ChowdhuryNo ratings yet
- Case Series AminaphtoneDocument3 pagesCase Series AminaphtoneevalubisNo ratings yet
- Principles of Topical Treatments in DermatologyDocument18 pagesPrinciples of Topical Treatments in DermatologyAnonymous OlS0WZwNo ratings yet
- AAD Atopic Dermatitis - Phototherapy and Systemic Agents 2014Document42 pagesAAD Atopic Dermatitis - Phototherapy and Systemic Agents 2014Yan Zhen YuanNo ratings yet
- Derma MegatableDocument21 pagesDerma MegatableNicole ChanNo ratings yet
- An Approach To The Patient With ErythrodermaDocument42 pagesAn Approach To The Patient With ErythrodermaShakilNo ratings yet
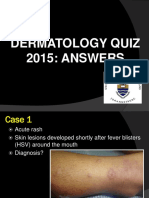
- Dermatology Quiz 2015 AnswersDocument40 pagesDermatology Quiz 2015 Answerspoorva shahNo ratings yet
- Omalizumab in DermatologyDocument35 pagesOmalizumab in DermatologyDeval MistryNo ratings yet
- Dermatology Lectures JRRMMCDocument10 pagesDermatology Lectures JRRMMCGi Em100% (1)
- Dermatoven MCQDocument30 pagesDermatoven MCQS2 GIZI FKUI 2020No ratings yet
- Oral Dermatology: Important Oral Questions & AnswersDocument29 pagesOral Dermatology: Important Oral Questions & AnswersMedo JTNo ratings yet
- Dermatology Skin in Systemic DiseaseDocument47 pagesDermatology Skin in Systemic DiseaseNariska CooperNo ratings yet
- Sqweqwesf Erwrewfsdfs Adasd Dhe: Dermnet NZDocument19 pagesSqweqwesf Erwrewfsdfs Adasd Dhe: Dermnet NZkdwazirNo ratings yet
- Viral-Exanthems Read Only RVDocument66 pagesViral-Exanthems Read Only RVAde JuandaNo ratings yet
- Skin Diseases Affecting The VulvaDocument7 pagesSkin Diseases Affecting The VulvaNoraNo ratings yet
- General Considerations For Topical PreparationsDocument6 pagesGeneral Considerations For Topical PreparationsOccamsRazorNo ratings yet
- Hair Growth Disorders N Pigmentary DisordersDocument7 pagesHair Growth Disorders N Pigmentary Disordersmrosaregina michelleNo ratings yet
- Chapter-03 Acneiform EruptionDocument6 pagesChapter-03 Acneiform EruptionSylvia DiamondNo ratings yet
- Botox in Facial AestheticsDocument27 pagesBotox in Facial AestheticsTip Piraya100% (6)
- DA Sistemik TerapiDocument11 pagesDA Sistemik TerapiariyatiNo ratings yet
- Derma MCQ Ch01 PDFDocument20 pagesDerma MCQ Ch01 PDFShah NawazNo ratings yet
- Pigmentary Disorders in Asian Skin Treatment With Laser and Intense Pulsed Light SourcesDocument8 pagesPigmentary Disorders in Asian Skin Treatment With Laser and Intense Pulsed Light SourcesLutfi MKNo ratings yet
- Superficial Fungal Infections of The Skin VoiceoverDocument67 pagesSuperficial Fungal Infections of The Skin VoiceoverMedo JT100% (1)
- Medical Surgical Nursing AssignmentDocument166 pagesMedical Surgical Nursing AssignmentSonali Sengar0% (1)
- KEY: Certain, Pretty Sure, Possible: 18 Years Old/female CameDocument8 pagesKEY: Certain, Pretty Sure, Possible: 18 Years Old/female Camefairodz salapudinNo ratings yet
- Language of DermatologyDocument45 pagesLanguage of DermatologykurutalaNo ratings yet
- Photodermatologic Disorders (Photodermatoses) : Mikias Woldetensay Dermatology & Venereology Oct 2021Document59 pagesPhotodermatologic Disorders (Photodermatoses) : Mikias Woldetensay Dermatology & Venereology Oct 2021CHALIE MEQUNo ratings yet
- Cards+Against+Paediatric+Dermatology+-+Vickie+Wells+&+Emma+Buxton+ (v1 0)Document146 pagesCards+Against+Paediatric+Dermatology+-+Vickie+Wells+&+Emma+Buxton+ (v1 0)Donna Ricotta100% (1)
- Palmoplantar KeratodermaDocument4 pagesPalmoplantar KeratodermakurutalaNo ratings yet
- Dermatology Questions and AnsDocument147 pagesDermatology Questions and AnsEl FaroukNo ratings yet
- Advantage Basic Nursing Thinking Doing and Caring 2nd by Treas DavisDocument21 pagesAdvantage Basic Nursing Thinking Doing and Caring 2nd by Treas DavisjennieNo ratings yet
- Clinical Cases in Dermatology Modern Management of Acne Actinic Keratosis and Atopic DermatitisDocument7 pagesClinical Cases in Dermatology Modern Management of Acne Actinic Keratosis and Atopic DermatitisJpratoNo ratings yet
- Dermatology CasesDocument4 pagesDermatology Casesejikieru03No ratings yet
- Panniculitis 2021Document45 pagesPanniculitis 2021karimahihdaNo ratings yet
- Acne Vulgaris (Or Acne) Is A CommonDocument21 pagesAcne Vulgaris (Or Acne) Is A CommonNia YuniarNo ratings yet
- Carti DermatoDocument29 pagesCarti Dermatosepis10No ratings yet
- Andrews - Chapter 4 - Pruritus and Neurocutaneous DermatosesDocument40 pagesAndrews - Chapter 4 - Pruritus and Neurocutaneous DermatosesAngeli Ramos-EstrellaNo ratings yet
- Stasis Dermatitis and Leg UlcersDocument76 pagesStasis Dermatitis and Leg Ulcersozhan_holmesNo ratings yet
- Steroid Pulse Therapies in DermatologyDocument4 pagesSteroid Pulse Therapies in DermatologyWelly WijayantiNo ratings yet
- Topical Antibiotics in DermatologyDocument19 pagesTopical Antibiotics in DermatologyJejem Marandra EmkamasNo ratings yet
- Dermatology FinalDocument16 pagesDermatology FinalMelinda100% (2)
- Introduction To Dermatology Assessment of A Dermatologic PatientDocument86 pagesIntroduction To Dermatology Assessment of A Dermatologic PatientAtifNo ratings yet
- Paraneoplastic DermatosesDocument57 pagesParaneoplastic DermatosesMohamed Riyaz100% (1)
- Derm - Monitoring Systemic MedicationsDocument3 pagesDerm - Monitoring Systemic MedicationsriskhakovNo ratings yet
- Skin Disease WartsDocument4 pagesSkin Disease WartsFatima Al MarzouqiNo ratings yet
- June 2022 - Dermatology - 10 McqsDocument8 pagesJune 2022 - Dermatology - 10 McqsAhmed ShihataNo ratings yet
- Dermatology - LoveDocument433 pagesDermatology - LoveAntonio EscobarNo ratings yet
- UrticariaDocument12 pagesUrticarialilyrbrtNo ratings yet
- Molluscum Contagiosum Module - PPSXDocument38 pagesMolluscum Contagiosum Module - PPSXDevy Anggi SitompulNo ratings yet
- Anti Fungal DrugsDocument6 pagesAnti Fungal Drugsbilal ahmadNo ratings yet
- Dermnet NZ: Special Stains and TestsDocument4 pagesDermnet NZ: Special Stains and TestsRaja Sekaran DuraiNo ratings yet
- Vaccine MalariaDocument15 pagesVaccine MalariaRaissa ANo ratings yet
- Case Studies: Chapter 20: VancomycinDocument5 pagesCase Studies: Chapter 20: VancomycinSaul RuizNo ratings yet
- Expert Report On Innovations in Health Care in The Slovak RepublicDocument62 pagesExpert Report On Innovations in Health Care in The Slovak RepublicPeter ŠtetkaNo ratings yet
- Pericardial DX Endocarditis MyocarditisDocument63 pagesPericardial DX Endocarditis MyocarditisIrfan Ners MaulanaNo ratings yet
- Transplantation Tolerance Through Mixed Chimerism. From Allo To XenoDocument11 pagesTransplantation Tolerance Through Mixed Chimerism. From Allo To XenoJose Adriel Chinchay FrancoNo ratings yet
- Affidavit of Darrell Griffith in Kearney Vs University of KentuckyDocument3 pagesAffidavit of Darrell Griffith in Kearney Vs University of KentuckyPaulKearneyCase1No ratings yet
- Nursing Care PlanDocument18 pagesNursing Care PlanElla Grace PradoNo ratings yet
- Concept MapDocument10 pagesConcept Mapapi-608044542No ratings yet
- Health Insurance in IndiaDocument7 pagesHealth Insurance in Indianetsavy71No ratings yet
- Complete Catalogue AUGUST 2017Document32 pagesComplete Catalogue AUGUST 2017RajeevSangamNo ratings yet
- Playing Video Games Liked To AsthmaDocument2 pagesPlaying Video Games Liked To AsthmaSandroLaoNo ratings yet
- Pengetahuan Ergonomi Dan Postur Kerja Perawat Pada Perawatan Luka Dengan Gangguan Muskuloskeletal Di Dr. H. Koesnadi BondowosoDocument5 pagesPengetahuan Ergonomi Dan Postur Kerja Perawat Pada Perawatan Luka Dengan Gangguan Muskuloskeletal Di Dr. H. Koesnadi BondowosoImanuel SihotangNo ratings yet
- Reviewer CDI 7Document6 pagesReviewer CDI 720-0383.dizorNo ratings yet
- LUNG CaDocument59 pagesLUNG CaokaciaNo ratings yet
- What Is Mcardle'S Disease?Document2 pagesWhat Is Mcardle'S Disease?automatissunNo ratings yet
- LaboratoryDocument2 pagesLaboratoryEdsel OtaoNo ratings yet
- Acute Mastoiditis in Adults and ChildrenDocument5 pagesAcute Mastoiditis in Adults and ChildrenAnonymous tG35SYROzENo ratings yet
- DipiroDocument38 pagesDipiroPetrick Ariska Pratama50% (2)
- McNeill Dysphagia Therapy ProgramDocument5 pagesMcNeill Dysphagia Therapy ProgramBeca ArmyNo ratings yet
- English Research PaperDocument6 pagesEnglish Research Paperapi-390838152No ratings yet
- Medicine PDFDocument24 pagesMedicine PDFBharat JamodNo ratings yet
- NCP Diabetes MellitusDocument5 pagesNCP Diabetes MellitusDenise Loren O. PamaongNo ratings yet
- Wound Dressing ThesisDocument5 pagesWound Dressing Thesisfd0kyjpa100% (1)