You might also like
- List of Psychological TestsDocument11 pagesList of Psychological Testsmenar86% (7)
- TodosDocument97 pagesTodosRenata Flor0% (1)
- Member 1 (Saher) Life Position:: The Life Positions Can Be Categorized As FollowsDocument8 pagesMember 1 (Saher) Life Position:: The Life Positions Can Be Categorized As FollowsUmar GhaniNo ratings yet
- Supported Living Strategy For Mental HealthDocument63 pagesSupported Living Strategy For Mental HealthAnonymous 9iK0i8h0dPNo ratings yet
- Emergency Care Algorithms 2018 PDFDocument77 pagesEmergency Care Algorithms 2018 PDFFranklin Correa100% (2)
- Guide Clinical Interview and Psychological Report of Clinical CasesDocument9 pagesGuide Clinical Interview and Psychological Report of Clinical CasesMaría González MartínNo ratings yet
- UK AND US HEALTHCARE COMPARISON - EditedDocument19 pagesUK AND US HEALTHCARE COMPARISON - EditedAbiola Abraham100% (1)
- Shop Resource PackDocument130 pagesShop Resource PackAndreea BirceaNo ratings yet
- Towards A Spirit at Peace: Understanding The Treatment of Shen Disorders With Chinese MedicineDocument6 pagesTowards A Spirit at Peace: Understanding The Treatment of Shen Disorders With Chinese MedicineMarcin SowNo ratings yet
- Hospice and End of Life Care PaperDocument6 pagesHospice and End of Life Care Paperapi-570837257No ratings yet
- Prenatal ExperiencingLudwigJanusDocument297 pagesPrenatal ExperiencingLudwigJanusSimon FalconiNo ratings yet
- Population Health Systems Kingsfund Feb15Document40 pagesPopulation Health Systems Kingsfund Feb15Anonymous IUFzAW9wHGNo ratings yet
- Diabetes InsipidusDocument8 pagesDiabetes InsipidusNader Smadi100% (5)
- Seminar On AsthmaDocument27 pagesSeminar On Asthmalumina.s100% (1)
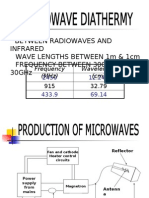
- Microwave DiathermyDocument14 pagesMicrowave Diathermybpt2No ratings yet
- MenopauseDocument49 pagesMenopauseKaruna Kumari100% (3)
- Unit 3 Health and Social CareDocument22 pagesUnit 3 Health and Social Carearies usamaNo ratings yet
- Unit 3 Health and Social CareDocument22 pagesUnit 3 Health and Social Carearies usamaNo ratings yet
- A Case Study On Chronic Renal DiseaseDocument17 pagesA Case Study On Chronic Renal Diseasematucojulio100% (1)
- Understanding The Human Services: AssignmentDocument8 pagesUnderstanding The Human Services: AssignmentHasan MahmoodNo ratings yet
- Care of The Older People WorkDocument11 pagesCare of The Older People Workbright osakweNo ratings yet
- A Summary of The Final ReportDocument115 pagesA Summary of The Final ReportcozzaflorenceNo ratings yet
- Unit 3 - Final - EditedDocument16 pagesUnit 3 - Final - EditedBeenishFatimaNo ratings yet
- Paula Anglia Ruskin-ARU-HEDocument19 pagesPaula Anglia Ruskin-ARU-HERoki Hassan0% (1)
- Sunita Saturday SAP - EditedDocument7 pagesSunita Saturday SAP - EditedMonisha ChaturvediNo ratings yet
- Impact of Ageing Population On Models of Health Care DeliveryDocument10 pagesImpact of Ageing Population On Models of Health Care DeliveryWaruingi WamungaiNo ratings yet
- Running Head: POLICYDocument11 pagesRunning Head: POLICYHamza HaiderNo ratings yet
- The Impact of Community Care Policy On Older People in Britain. 1970s-1990s by Flourish Itulua-AbumereDocument5 pagesThe Impact of Community Care Policy On Older People in Britain. 1970s-1990s by Flourish Itulua-AbumereFlourish Itulua-Abumere100% (3)
- Literature Review: Quality Management and Improvement Practices For Home and Community-Based CareDocument76 pagesLiterature Review: Quality Management and Improvement Practices For Home and Community-Based CareJame StuartNo ratings yet
- Briefing20 Scie Personal Budgets Young PeopleDocument28 pagesBriefing20 Scie Personal Budgets Young PeopleONLINEACCOUNT7715No ratings yet
- Unit 3 - FinalDocument16 pagesUnit 3 - FinalBeenishFatimaNo ratings yet
- Securing Good Care Chapter 1Document21 pagesSecuring Good Care Chapter 1Adelina-sonilaTroianoNo ratings yet
- The Contextual Development of Healthy Living Centres Services: An Examination of Food-Related InitiativesDocument12 pagesThe Contextual Development of Healthy Living Centres Services: An Examination of Food-Related InitiativesDina OliveiraNo ratings yet
- Carers' Quality of Life and Experiences of Adult Social Care Support in EnglandDocument11 pagesCarers' Quality of Life and Experiences of Adult Social Care Support in EnglandNurul ShahirahNo ratings yet
- Achieving the Human Right to a Caring Society in an Aging AmericaFrom EverandAchieving the Human Right to a Caring Society in an Aging AmericaNo ratings yet
- Health Care Scotland - FinalDocument10 pagesHealth Care Scotland - FinalMonu BhagatNo ratings yet
- Jurnal R 9Document13 pagesJurnal R 9DhienWhieNo ratings yet
- A Critical Insight, Analysis and Comparative of Health Care Provision in The United Kingdom and United States of America.Document19 pagesA Critical Insight, Analysis and Comparative of Health Care Provision in The United Kingdom and United States of America.Abiola AbrahamNo ratings yet
- Awaiting Long-Term Care Services in A Rapidly Changing Environment: Voices From Older Chinese AdultsDocument17 pagesAwaiting Long-Term Care Services in A Rapidly Changing Environment: Voices From Older Chinese AdultsForce MapuNo ratings yet
- Unit 3 - Final - Edited.editedDocument16 pagesUnit 3 - Final - Edited.editedBeenishFatimaNo ratings yet
- Taskforce On Care CostsDocument72 pagesTaskforce On Care CostslibrarycvNo ratings yet
- 6988 EditedDocument11 pages6988 EditedHamza HaiderNo ratings yet
- Good Housing Leads To Good Health: A Toolkit For Environmental Health PractitionersDocument44 pagesGood Housing Leads To Good Health: A Toolkit For Environmental Health PractitionersJaymark BanaagNo ratings yet
- The Financial Impact of Social Care On UK EconomyDocument22 pagesThe Financial Impact of Social Care On UK EconomyDeva LinaNo ratings yet
- Personalisation ReportDocument75 pagesPersonalisation ReportChristina MironovNo ratings yet
- 2020 - Ikegami - Choices in PublicpoliticymakersDocument16 pages2020 - Ikegami - Choices in Publicpoliticymakersplft.alma.romoNo ratings yet
- Discussion Paper 1: Enshrining The Ability To Work in The New NHS, Steve BoormanDocument9 pagesDiscussion Paper 1: Enshrining The Ability To Work in The New NHS, Steve BoormanFitForWorkUKNo ratings yet
- No 362524 3Document5 pagesNo 362524 3My EscrowNo ratings yet
- Tucker Et AlDocument16 pagesTucker Et AlEno RLNo ratings yet
- 16 Ok Ok Kumar & Bauer - Lean Thinking and Six Sigma in Public Housing Autorities - 2010Document18 pages16 Ok Ok Kumar & Bauer - Lean Thinking and Six Sigma in Public Housing Autorities - 2010Oscar Ivan Londoño GalvizNo ratings yet
- ILMs 5 Asks For A Better Health and Social Care Integration August 2013Document5 pagesILMs 5 Asks For A Better Health and Social Care Integration August 2013Priyadershi RakeshNo ratings yet
- Department of Health and Human Services MemoDocument10 pagesDepartment of Health and Human Services MemoGazetteonlineNo ratings yet
- Determining The Implementation Status of Benefits Under Magna Carta of Public Health Workers (RA 7305) in The PhilippinesDocument7 pagesDetermining The Implementation Status of Benefits Under Magna Carta of Public Health Workers (RA 7305) in The Philippineslea mae andoloyNo ratings yet
- Question 2: Write Notes On Any Two: B) Types of Ngos: Stake Holders in Health Care SectorDocument5 pagesQuestion 2: Write Notes On Any Two: B) Types of Ngos: Stake Holders in Health Care SectordrkamaniNo ratings yet
- CSJJ8435 Universal Credit Universal Support 201007Document56 pagesCSJJ8435 Universal Credit Universal Support 201007Gail WardNo ratings yet
- Developing A New Next National Disability Strategy Implementation Plan - Consultation DocumentDocument6 pagesDeveloping A New Next National Disability Strategy Implementation Plan - Consultation DocumentGateway ProjectNo ratings yet
- An Overview of The White Paper " Caring For Our Future - Reforming Care and Support"Document4 pagesAn Overview of The White Paper " Caring For Our Future - Reforming Care and Support"My Care My HomeNo ratings yet
- Care in Old Age in Southeast Asia and ChinaDocument54 pagesCare in Old Age in Southeast Asia and ChinatassiahNo ratings yet
- The Private Sector,: Universal Health Coverage and Primary Health CareDocument12 pagesThe Private Sector,: Universal Health Coverage and Primary Health CareJohn Aries CabilingNo ratings yet
- Assertive Community Treatment For People With Severe Mental IllnessDocument19 pagesAssertive Community Treatment For People With Severe Mental IllnessMarco Herrera FloresNo ratings yet
- Stakeholder & Peak BodiesDocument3 pagesStakeholder & Peak Bodies244 Sohan MiaNo ratings yet
- Discussion Paper 2 Approaches For Reform FINALDocument69 pagesDiscussion Paper 2 Approaches For Reform FINALAllison Buchan-TerrellNo ratings yet
- Global Budgeting Promoting Flexible Funding To Support Long Term Care ChoicesDocument25 pagesGlobal Budgeting Promoting Flexible Funding To Support Long Term Care ChoicesLeslie HendricksonNo ratings yet
- Critical Social Work As Human Rights Practice in Hospital Discharge SettingsDocument4 pagesCritical Social Work As Human Rights Practice in Hospital Discharge SettingsAngela BortaNo ratings yet
- Client Services IRC Industry Summary (Draft)Document7 pagesClient Services IRC Industry Summary (Draft)Thomas JurkiewiczNo ratings yet
- Community Mental Health Framework For Adults and Older AdultsDocument22 pagesCommunity Mental Health Framework For Adults and Older AdultsLuigi LuiNo ratings yet
- Task 1Document12 pagesTask 1aries usamaNo ratings yet
- Community Nursing and Care Continuity LEARNING OUTCOMES After CompletingDocument23 pagesCommunity Nursing and Care Continuity LEARNING OUTCOMES After Completingtwy113100% (1)
- OVSJG 2022 Performance Oversight Hearing TestimonyDocument9 pagesOVSJG 2022 Performance Oversight Hearing TestimonyCami MondeauxNo ratings yet
- Project Information Document (Pid) Appraisal Stage Project Name Region Sector Project ID Borrower(s) Implementing AgencyDocument10 pagesProject Information Document (Pid) Appraisal Stage Project Name Region Sector Project ID Borrower(s) Implementing AgencyMasab AliNo ratings yet
- 2001 - America's Forgotten Families: Voices of Welfare ReformDocument55 pages2001 - America's Forgotten Families: Voices of Welfare ReformUnitarian Universalist Service CommitteeNo ratings yet
- The Declining Work and Welfare of People with Disabilities: What Went Wrong and a Strategy for ChangeFrom EverandThe Declining Work and Welfare of People with Disabilities: What Went Wrong and a Strategy for ChangeNo ratings yet
- Revised Pn-Law Society and Controversy (K9nke4six5) 1Document12 pagesRevised Pn-Law Society and Controversy (K9nke4six5) 1aries usamaNo ratings yet
- Self-Development PortfolioDocument19 pagesSelf-Development Portfolioaries usamaNo ratings yet
- ZJ052303Document7 pagesZJ052303aries usamaNo ratings yet
- Case Study RAH-EDU-2517Document10 pagesCase Study RAH-EDU-2517aries usamaNo ratings yet
- Rah Edu 2517Document9 pagesRah Edu 2517aries usamaNo ratings yet
- Is Healthcare A Right or A PrivilegeDocument6 pagesIs Healthcare A Right or A Privilegearies usamaNo ratings yet
- Research Notes - JassDocument3 pagesResearch Notes - Jassaries usamaNo ratings yet
- Task 1Document12 pagesTask 1aries usamaNo ratings yet
- Paternalism in HealthcareDocument9 pagesPaternalism in Healthcarearies usamaNo ratings yet
- Role of HR in Employee Motivation AssignmentDocument10 pagesRole of HR in Employee Motivation Assignmentaries usamaNo ratings yet
- Quality Management in A Care Setting Assignment Q1.Document13 pagesQuality Management in A Care Setting Assignment Q1.aries usamaNo ratings yet
- Health and Social Care Education in Action Unit 5Document26 pagesHealth and Social Care Education in Action Unit 5aries usamaNo ratings yet
- Positive Impact of Covid On TESCO EssayDocument4 pagesPositive Impact of Covid On TESCO Essayaries usamaNo ratings yet
- Paternalism in HealthcareDocument9 pagesPaternalism in Healthcarearies usamaNo ratings yet
- Innovation and Commercialization Report AssignmentDocument15 pagesInnovation and Commercialization Report Assignmentaries usamaNo ratings yet
- Doping AssignmentDocument5 pagesDoping Assignmentaries usamaNo ratings yet
- Stemcelltransplantation PDFDocument33 pagesStemcelltransplantation PDFharshit chaudharyNo ratings yet
- Complications of Upper GI SDocument30 pagesComplications of Upper GI SNavin ChandarNo ratings yet
- MinefieldDocument4 pagesMinefieldnitin21822No ratings yet
- DRUG STUDY Cefu and Keto and SummaryDocument8 pagesDRUG STUDY Cefu and Keto and SummaryAmanie Usman AmanoddinNo ratings yet
- Basic Information On Pharmaceutical Dosage Forms and Drug Delivery SystemsDocument30 pagesBasic Information On Pharmaceutical Dosage Forms and Drug Delivery SystemsSyed Hussain AsafNo ratings yet
- Hypo Kale MiaDocument13 pagesHypo Kale MiaMuhammad IqbalNo ratings yet
- Activity N0. 2 Daily Lesson PlanDocument3 pagesActivity N0. 2 Daily Lesson PlanRobert Andrew BaldadoNo ratings yet
- Esthetic and Endodontic Management of A Deep Crown-Root Fracture of A Maxillary Central IncisorDocument4 pagesEsthetic and Endodontic Management of A Deep Crown-Root Fracture of A Maxillary Central IncisordrgozanNo ratings yet
- Progressive Strengthening and Stretching Exercises and Ultrasound For Chronic Lateral EpicondylitisDocument9 pagesProgressive Strengthening and Stretching Exercises and Ultrasound For Chronic Lateral EpicondylitisTomBrambo100% (1)
- Atherosclerosis-Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis-Dyslipidaemia and Diabetes SlidesECG17No ratings yet
- TCHP Shock Series Part 2Document2 pagesTCHP Shock Series Part 2ikeernawatiNo ratings yet
- Hakomi - Working With The Response BarrierDocument2 pagesHakomi - Working With The Response BarrierPaul HubbardNo ratings yet
- Group DynamicsDocument20 pagesGroup Dynamicspriyadarade97No ratings yet
- Principles of Toxicology: The Study of PoisonsDocument42 pagesPrinciples of Toxicology: The Study of PoisonsAgnivesh MangalNo ratings yet
- Pathology 2 TND LiveDocument38 pagesPathology 2 TND Livepavan kumarNo ratings yet
- Curriculm VitaeDocument10 pagesCurriculm Vitaeapi-603235692No ratings yet
- B PharmacyDocument26 pagesB PharmacyAkankshaNo ratings yet
- Peters AptDocument49 pagesPeters AptAlejandra VitiNo ratings yet