You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- English Vocabulary For Medicine-2Document65 pagesEnglish Vocabulary For Medicine-2Denisse Segura100% (1)
- Renal TransplantDocument29 pagesRenal TransplantSujith Kuttan100% (1)
- ChecklistDocument2 pagesChecklisthappyNo ratings yet
- Hospital Design Data CollectionDocument59 pagesHospital Design Data CollectionSHERYL SHEKINAH E ARCH-2019 BATCH100% (1)
- Compile NeonateDocument32 pagesCompile NeonateWan Ahmad FaizFaizalNo ratings yet
- Erpm InfoDocument16 pagesErpm InfoPamudri Basnayake100% (1)
- JCRreputasisedangDocument10 pagesJCRreputasisedangMuhammad Ilham MaulanaNo ratings yet
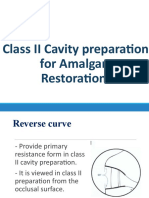
- Class II Cavity Preparation - 2Document28 pagesClass II Cavity Preparation - 2Tarteel MagdiNo ratings yet
- COPD TextbookDocument10 pagesCOPD Textbooknob2011nobNo ratings yet
- Tocilizumab and Remdesivir in HospitalizedDocument13 pagesTocilizumab and Remdesivir in HospitalizedYulian 53No ratings yet
- Bloom ChennaiDocument1 pageBloom ChennaiBloomChennai2012No ratings yet
- IBS Guidelines - Cervical Cancer Brachytherapy-3Document14 pagesIBS Guidelines - Cervical Cancer Brachytherapy-3Florina SimniceanuNo ratings yet
- PDFDocument2 pagesPDFSubhash BeraNo ratings yet
- Contact Derma TitusDocument5 pagesContact Derma TitusTiti PermatasariNo ratings yet
- Perawatan Luka Diabetes Mellitus Menggunakan Teknik Modern Dressing Alberikus Dimantika, Sugiyarto, Yuyun SetyoriniDocument13 pagesPerawatan Luka Diabetes Mellitus Menggunakan Teknik Modern Dressing Alberikus Dimantika, Sugiyarto, Yuyun SetyoriniNita ZahriNo ratings yet
- Preterm LaborDocument50 pagesPreterm LaborDr-Firas Nayf Al-ThawabiaNo ratings yet
- Referat OsteochondromaDocument3 pagesReferat Osteochondromaricha difayanaNo ratings yet
- Infectious Diseases EpidemiologyDocument28 pagesInfectious Diseases EpidemiologySarad Chand YadavNo ratings yet
- Fitt 1 - Activity 5Document1 pageFitt 1 - Activity 5zavriaNo ratings yet
- Vinu CV 2018Document10 pagesVinu CV 2018Vinu PoojapranavamNo ratings yet
- Department List - November 2018 SCHDocument12 pagesDepartment List - November 2018 SCHJustin SteeleNo ratings yet
- 2006 - Treatment of Extended1Document4 pages2006 - Treatment of Extended1Leidy NeiraNo ratings yet
- DR SathyaDocument34 pagesDR SathyaYoza FirdaozNo ratings yet
- Intraoperative CholangiogramDocument3 pagesIntraoperative CholangiogramPauline Jimenea100% (2)
- 17th Asian Games Incheon 2014Document44 pages17th Asian Games Incheon 2014dantevermillionNo ratings yet
- Meher Pharma International: Innovates FDCDocument4 pagesMeher Pharma International: Innovates FDCMohammad Shahbaz AlamNo ratings yet
- OFMR 31jul2009 PDFDocument147 pagesOFMR 31jul2009 PDFSanjib Kumar MandalNo ratings yet
- Philhealth TB PDFDocument35 pagesPhilhealth TB PDFO.r. CadzNo ratings yet
- General Science Solutions For Class 8 Science Chapter 2Document6 pagesGeneral Science Solutions For Class 8 Science Chapter 2Ashwini KhareNo ratings yet
- ReadinglistmbDocument1 pageReadinglistmbMahmOod GhNo ratings yet