You might also like
- Autism Test-1Document4 pagesAutism Test-1Salbia RiasatNo ratings yet
- Cluster BDocument62 pagesCluster BAshish DootNo ratings yet
- Medical Certificate For Service at Sea: ConfidentialDocument4 pagesMedical Certificate For Service at Sea: ConfidentialADMIN MCU RSU SAHID SAHIRMAN100% (1)
- Ischemic Heart DiseaseDocument67 pagesIschemic Heart Diseasealfaz lakhani80% (5)
- Medical Evaluation Form 2022Document2 pagesMedical Evaluation Form 2022jimmy p. lamhi50% (2)
- Geri - Nutrition Study GuideDocument5 pagesGeri - Nutrition Study GuideMonica Castillo MearesNo ratings yet
- Older Adult - Soap 2 PDFDocument4 pagesOlder Adult - Soap 2 PDFSavanna EarleNo ratings yet
- Microbiologist: 3.1.5 Isolation & Gram StainingDocument5 pagesMicrobiologist: 3.1.5 Isolation & Gram Stainingapi-534896073No ratings yet
- UHS Pre-Enrolment Physical (Medical) Examination Form PDFDocument2 pagesUHS Pre-Enrolment Physical (Medical) Examination Form PDFReaStephanieCidNo ratings yet
- 1 Glomerular DiseasesDocument127 pages1 Glomerular DiseasesCoy NuñezNo ratings yet
- HISTORY TAKING: Acute GastroenteritisDocument4 pagesHISTORY TAKING: Acute GastroenteritisSham100% (1)
- Biennial National Medical ReportDocument5 pagesBiennial National Medical ReportXimena FariasNo ratings yet
- Health Assessment Form For Student 022Document1 pageHealth Assessment Form For Student 022Ko AlphaNo ratings yet
- Student Haf RevDocument1 pageStudent Haf Revalexamyles sepicoNo ratings yet
- Dile Jamiel Lyca A. New HafDocument1 pageDile Jamiel Lyca A. New HafPaul SahagunNo ratings yet
- F2F HAF For StudentDocument1 pageF2F HAF For StudentG4 AMOYO ANGELICA NICOLENo ratings yet
- Nicanor Reyes Medical Foundation: Far Eastern UniversityDocument2 pagesNicanor Reyes Medical Foundation: Far Eastern UniversityAudreyNo ratings yet
- Nicanor Reyes Medical Foundation: Far Eastern UniversityDocument2 pagesNicanor Reyes Medical Foundation: Far Eastern UniversityGeorgeMarcusNo ratings yet
- Hope Week 4Document11 pagesHope Week 4Joseph Patrick OcapanNo ratings yet
- New Normal Health Assessment Form For Learners 2020 RegionDocument4 pagesNew Normal Health Assessment Form For Learners 2020 RegionCleofe Mae Piñero AseñasNo ratings yet
- 02.borang Diabetes Outcome UpdateDocument1 page02.borang Diabetes Outcome Updatesuhairizwan ab wahabNo ratings yet
- Health Declaration: Teresita L. Jalandoni Provincial HospitalDocument2 pagesHealth Declaration: Teresita L. Jalandoni Provincial HospitalPrincess Faniega SugatonNo ratings yet
- IMNCI - A3 - EnglishDocument4 pagesIMNCI - A3 - EnglishRedietNo ratings yet
- Pediatrics HX ImportantDocument7 pagesPediatrics HX ImportantYaseen AhmadNo ratings yet
- Special Triage Screening Form For COVID 19 1Document1 pageSpecial Triage Screening Form For COVID 19 1Kathleen Joy PingenNo ratings yet
- Applicant Set Up Questionnaire: Section 1Document5 pagesApplicant Set Up Questionnaire: Section 1Jason BarnardNo ratings yet
- Health Assessment Form FinalDocument1 pageHealth Assessment Form FinalJohn Mark SalazarNo ratings yet
- Diabetes+mellitus+questionnaire ApplicantDocument2 pagesDiabetes+mellitus+questionnaire ApplicantClaudine Limasa TabudlongNo ratings yet
- Medical HistoryDocument3 pagesMedical HistoryHassan HekmatNo ratings yet
- New Patient Forms Package1Document2 pagesNew Patient Forms Package1Ache HNo ratings yet
- COVID19 Monitoring Form July2020Document1 pageCOVID19 Monitoring Form July2020TDRSNo ratings yet
- Pat ms1 3 08Document14 pagesPat ms1 3 08api-371817203No ratings yet
- Msii Pat 1-1Document22 pagesMsii Pat 1-1api-404285262No ratings yet
- WhatsInMarsR22021 - Hilary JansenDocument33 pagesWhatsInMarsR22021 - Hilary JansenerikaNo ratings yet
- English Course: Pharmacy StudentsDocument36 pagesEnglish Course: Pharmacy StudentsAmida UrfaNo ratings yet
- OGUK Medical FormDocument7 pagesOGUK Medical Formum erNo ratings yet
- Field Work Report R-CongoDocument9 pagesField Work Report R-Congoritwik microlabsNo ratings yet
- REPORTDocument24 pagesREPORTPABLO, JACKSON P.No ratings yet
- Infection Screening Form Word TemplateDocument1 pageInfection Screening Form Word TemplateTan Chris PaoloNo ratings yet
- ms1 PatDocument14 pagesms1 Patapi-364212510No ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormMark Israel DirectoNo ratings yet
- GeorgeDocument2 pagesGeorgeSteve MaguireNo ratings yet
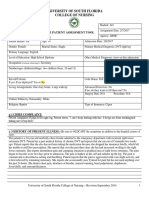
- University of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient InformationDocument16 pagesUniversity of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient Informationapi-402496681No ratings yet
- Physical Form 2018Document2 pagesPhysical Form 2018api-247134277No ratings yet
- GratataDocument1 pageGratataJeremy VelasquezNo ratings yet
- Pat Med Surg IDocument21 pagesPat Med Surg Iapi-399464028No ratings yet
- Uncpn Form New Patient Medical HistoryDocument5 pagesUncpn Form New Patient Medical HistorySonuraj rana RanaNo ratings yet
- Management of COVID-19 - KURNIA 2021Document108 pagesManagement of COVID-19 - KURNIA 2021Ricky Cornelius TariganNo ratings yet
- Medical Examination Form 2022-2023Document5 pagesMedical Examination Form 2022-2023Linh ĐặngNo ratings yet
- Texas Department of State Health Services Tuberculosis Health Assessment/HistoryDocument2 pagesTexas Department of State Health Services Tuberculosis Health Assessment/HistoryMohd Faiz Mohd ZinNo ratings yet
- Ms 1 Pat Marline FaustinDocument18 pagesMs 1 Pat Marline Faustinapi-365764138No ratings yet
- Clerk Sheet Imed and ObsDocument4 pagesClerk Sheet Imed and ObsGrace PhiriNo ratings yet
- Pharmaceutical Care&Pembahasan CKD, CHF, HT, CAPDocument13 pagesPharmaceutical Care&Pembahasan CKD, CHF, HT, CAPSelpiani AstutyNo ratings yet
- Consent For Minor Dental PDFDocument2 pagesConsent For Minor Dental PDFJanNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormUzair KhalidNo ratings yet
- Health CertificateDocument2 pagesHealth CertificateChristos YiangouNo ratings yet
- NCMH NotesDocument7 pagesNCMH NotesAlex Araya PabellanNo ratings yet
- Full Medical Records A PerkoulidisDocument146 pagesFull Medical Records A PerkoulidisDr Paul PerkoulidisNo ratings yet
- Health Declaration FormDocument3 pagesHealth Declaration FormBerlyn ColegadoNo ratings yet
- Vendivel IE SampleDocument12 pagesVendivel IE SampleMargareth Christine CusoNo ratings yet
- University of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient InformationDocument17 pagesUniversity of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient Informationapi-355083078No ratings yet
- Congvax Booster HDF Consent FormDocument2 pagesCongvax Booster HDF Consent FormMichael Mangay-atNo ratings yet
- ms1 Pat 2-2Document21 pagesms1 Pat 2-2api-404285262No ratings yet
- Pat1 2Document16 pagesPat1 2api-385494784No ratings yet
- Registration FormDocument3 pagesRegistration Formsimon farrellNo ratings yet
- GROUP 5 1.02.0 The Effects of Hobbies in Mental Health of Student in Our Lady of Fatima UniversityDocument6 pagesGROUP 5 1.02.0 The Effects of Hobbies in Mental Health of Student in Our Lady of Fatima UniversityDEALAGDON, RhyzaNo ratings yet
- Week 7 Activity - COMPREHENSION CHECKDocument3 pagesWeek 7 Activity - COMPREHENSION CHECKDEALAGDON, RhyzaNo ratings yet
- A Lesson For The SulutanDocument3 pagesA Lesson For The SulutanDEALAGDON, RhyzaNo ratings yet
- Week 5 ActivityDocument3 pagesWeek 5 ActivityDEALAGDON, RhyzaNo ratings yet
- Final Research Group 4 Abm 12 BDocument88 pagesFinal Research Group 4 Abm 12 BDEALAGDON, RhyzaNo ratings yet
- Chapter 3 Financial Planning Tools and ConceptsDocument28 pagesChapter 3 Financial Planning Tools and ConceptsDEALAGDON, RhyzaNo ratings yet
- Day 1: FDAR/ NCP (Pain) : Form No.: Revision No.: Effectivity DateDocument3 pagesDay 1: FDAR/ NCP (Pain) : Form No.: Revision No.: Effectivity DateLiza M. PurocNo ratings yet
- Hope 4 (2ND Sem) - Module 5Document2 pagesHope 4 (2ND Sem) - Module 5Gleany lisle SarifaNo ratings yet
- Treatment of Sepsis by Extracorporeal Blood Purification SystemsDocument23 pagesTreatment of Sepsis by Extracorporeal Blood Purification SystemsyamtotlNo ratings yet
- Resumen Mental HealthDocument7 pagesResumen Mental Healthfelix1perez-5No ratings yet
- Quiz Critical CareDocument15 pagesQuiz Critical CareSuma AhmadNo ratings yet
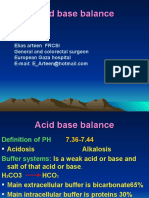
- Acid Base BalanceDocument69 pagesAcid Base BalanceAli AttarNo ratings yet
- CARDIODocument34 pagesCARDIOKevin Patrick PadolinaNo ratings yet
- Tube Insertion - NGT, Ogt (RM2021)Document2 pagesTube Insertion - NGT, Ogt (RM2021)Ray Emmanuel Enriquez DomingoNo ratings yet
- ALS Fact SheetDocument4 pagesALS Fact SheetGovar Miqdad GardiNo ratings yet
- DRUG STUDY (Ceftriaxone)Document2 pagesDRUG STUDY (Ceftriaxone)Avianna CalliopeNo ratings yet
- Homeopathy As Immunisation: Fiction SheetDocument2 pagesHomeopathy As Immunisation: Fiction SheetPaul GallagherNo ratings yet
- Mulat B.: Gastro Esophageal Reflux Disease (Gerd)Document44 pagesMulat B.: Gastro Esophageal Reflux Disease (Gerd)NehimyaNo ratings yet
- A Case Study of Urinary Tract Infection 2Document23 pagesA Case Study of Urinary Tract Infection 2Jenyl BajadoNo ratings yet
- Dementia SynopsisDocument9 pagesDementia SynopsisSuni Mary VargheseNo ratings yet
- 6 S's of Common Summer Diseases (Article and Infographics)Document4 pages6 S's of Common Summer Diseases (Article and Infographics)Dimitri MangubatNo ratings yet
- Skin DisordersDocument202 pagesSkin DisordersMj Briones100% (1)
- Breast CancerDocument19 pagesBreast CancerSuresh ThanneruNo ratings yet
- Irritablebowelsyndrome: What Treatments Really WorkDocument16 pagesIrritablebowelsyndrome: What Treatments Really WorkJavier Camino QuispeNo ratings yet
- Lilelihood RatioDocument10 pagesLilelihood Ratiorajesh ramukaNo ratings yet
- Foundations in Microbiology: TalaroDocument71 pagesFoundations in Microbiology: Talaromertx013No ratings yet
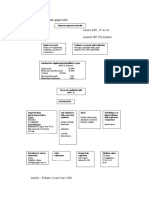
- Algoritma Penatalaksanaan Gagal NafasDocument2 pagesAlgoritma Penatalaksanaan Gagal NafasLion Sangkut Neng EndiNo ratings yet
- Generic Name: Mebeverine Hydrochloride Mechanism of Action Side Effects/ Adverse Reaction Nursing Responsibility Assessment & Drug EffectsDocument4 pagesGeneric Name: Mebeverine Hydrochloride Mechanism of Action Side Effects/ Adverse Reaction Nursing Responsibility Assessment & Drug EffectsNiziu BearsNo ratings yet
- Chapter 4Document103 pagesChapter 4tenaw100% (1)
- A Retrospective Analysis of Fourniers Gangrene at A TertiaryGovernment Hospital in The PhilippinesDocument3 pagesA Retrospective Analysis of Fourniers Gangrene at A TertiaryGovernment Hospital in The PhilippinesGian PagadduNo ratings yet