0% found this document useful (0 votes)
831 views1 pageResponder Form
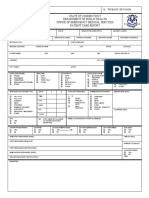
This document appears to be a form for first responders to document information about a medical emergency call. It includes fields to document details such as the nature of the call, patient information like name and vital signs, assessment findings including pupillary response and communication barriers, treatments provided such as oxygen administration and splinting, and a narrative section. The purpose is to collect essential information about the patient, incident, and emergency response.
Uploaded by
Jonard DuranCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
831 views1 pageResponder Form
This document appears to be a form for first responders to document information about a medical emergency call. It includes fields to document details such as the nature of the call, patient information like name and vital signs, assessment findings including pupillary response and communication barriers, treatments provided such as oxygen administration and splinting, and a narrative section. The purpose is to collect essential information about the patient, incident, and emergency response.
Uploaded by
Jonard DuranCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd