You might also like
- Culture and Depression: Studies in the Anthropology and Cross-Cultural Psychiatry of Affect and DisorderFrom EverandCulture and Depression: Studies in the Anthropology and Cross-Cultural Psychiatry of Affect and DisorderRating: 3 out of 5 stars3/5 (1)
- My Imaginary Illness: A Journey into Uncertainty and Prejudice in Medical DiagnosisFrom EverandMy Imaginary Illness: A Journey into Uncertainty and Prejudice in Medical DiagnosisNo ratings yet
- Caseness and Narrative: Contrasting Approaches to People Psychiatrically Labelled: Transformational Stories, #1From EverandCaseness and Narrative: Contrasting Approaches to People Psychiatrically Labelled: Transformational Stories, #1No ratings yet
- From Paralysis to Fatigue: A History of Psychosomatic Illness in the Modern EraFrom EverandFrom Paralysis to Fatigue: A History of Psychosomatic Illness in the Modern EraRating: 5 out of 5 stars5/5 (1)
- Mind and Body in Eighteenth Century Medicine: A Study Based on Jerome Gaub's De Regimine MentisFrom EverandMind and Body in Eighteenth Century Medicine: A Study Based on Jerome Gaub's De Regimine MentisNo ratings yet
- Under the Medical Gaze: Facts and Fictions of Chronic PainFrom EverandUnder the Medical Gaze: Facts and Fictions of Chronic PainNo ratings yet
- Search For The Real Self: Unmasking The Personality Disorders Of Our AgeFrom EverandSearch For The Real Self: Unmasking The Personality Disorders Of Our AgeRating: 3.5 out of 5 stars3.5/5 (18)
- Depression NarrativesDocument32 pagesDepression Narrativesstaygoldsam100% (1)
- Psychic Wholeness and Healing, Second Edition: Using All the Powers of the Human PsycheFrom EverandPsychic Wholeness and Healing, Second Edition: Using All the Powers of the Human PsycheNo ratings yet
- COVID-19/Mental Health Crises: Holistic Understanding and SolutionsFrom EverandCOVID-19/Mental Health Crises: Holistic Understanding and SolutionsNo ratings yet
- Talking Therapy: Knowledge and Power in American Psychiatric NursingFrom EverandTalking Therapy: Knowledge and Power in American Psychiatric NursingNo ratings yet
- Origins of Mental Illness: Temperament, Deviance and DisorderFrom EverandOrigins of Mental Illness: Temperament, Deviance and DisorderNo ratings yet
- Chronic Fatigue Syndrome, Fibromyalgia, and Other Invisible Illnesses: The Comprehensive GuideFrom EverandChronic Fatigue Syndrome, Fibromyalgia, and Other Invisible Illnesses: The Comprehensive GuideRating: 4.5 out of 5 stars4.5/5 (4)
- Destigmatising mental illness?: Professional politics and public education in Britain, 1870–1970From EverandDestigmatising mental illness?: Professional politics and public education in Britain, 1870–1970No ratings yet
- Suburban Shaman: tales from medicine's frontlineFrom EverandSuburban Shaman: tales from medicine's frontlineRating: 5 out of 5 stars5/5 (1)
- Invalid Women: Figuring Feminine Illness in American Fiction and Culture, 1840-1940From EverandInvalid Women: Figuring Feminine Illness in American Fiction and Culture, 1840-1940No ratings yet
- When A Doctor Hates A Patient: And Other Chapters in a Young Physician's LifeFrom EverandWhen A Doctor Hates A Patient: And Other Chapters in a Young Physician's LifeRating: 5 out of 5 stars5/5 (1)
- A Profession Without Reason: The Crisis of Contemporary Psychiatry—Untangled and Solved by Spinoza, Freethinking, and Radical EnlightenmentFrom EverandA Profession Without Reason: The Crisis of Contemporary Psychiatry—Untangled and Solved by Spinoza, Freethinking, and Radical EnlightenmentNo ratings yet
- Psychotherapy: the practical applications of modern psychologyFrom EverandPsychotherapy: the practical applications of modern psychologyNo ratings yet
- Doctoring the South: Southern Physicians and Everyday Medicine in the Mid-Nineteenth CenturyFrom EverandDoctoring the South: Southern Physicians and Everyday Medicine in the Mid-Nineteenth CenturyNo ratings yet
- Culture and PTSD: Trauma in Global and Historical PerspectiveFrom EverandCulture and PTSD: Trauma in Global and Historical PerspectiveNo ratings yet
- Transforming Trauma: A drugless and creative path to healing PTS and ACEFrom EverandTransforming Trauma: A drugless and creative path to healing PTS and ACENo ratings yet
- Dismissed: Tackling the Biases That Undermine our Health CareFrom EverandDismissed: Tackling the Biases That Undermine our Health CareNo ratings yet
- Counseling From Within: The Microbiome Mental Health ConnectionFrom EverandCounseling From Within: The Microbiome Mental Health ConnectionNo ratings yet
- The Lumber Room: Mental Illness in the House of Medicine (2016 second edition)From EverandThe Lumber Room: Mental Illness in the House of Medicine (2016 second edition)No ratings yet
- The Myth of Psychotherapy: Mental Healing as Religion, Rhetoric, and RepressionFrom EverandThe Myth of Psychotherapy: Mental Healing as Religion, Rhetoric, and RepressionRating: 4 out of 5 stars4/5 (7)
- Depression, Emotion and the Self: Philosophical and Interdisciplinary PerspectivesFrom EverandDepression, Emotion and the Self: Philosophical and Interdisciplinary PerspectivesNo ratings yet
- Understanding Troubled Minds Updated Edition: A guide to mental illness and its treatmentFrom EverandUnderstanding Troubled Minds Updated Edition: A guide to mental illness and its treatmentNo ratings yet
- Dealing with Depression: A commonsense guide to mood disordersFrom EverandDealing with Depression: A commonsense guide to mood disordersRating: 2 out of 5 stars2/5 (1)
- Download From Melancholia To Depression Disordered Mood In Nineteenth Century Psychiatry 1St Edition Edition Asa Jansson full chapterDocument68 pagesDownload From Melancholia To Depression Disordered Mood In Nineteenth Century Psychiatry 1St Edition Edition Asa Jansson full chaptermiguel.mckinney517100% (7)
- Metaphor and MedicineDocument9 pagesMetaphor and MedicineCrystal DuarteNo ratings yet
- Kleinman 1986Document12 pagesKleinman 1986Valentina QuinteroNo ratings yet
- The Americanization of Mental IllnessDocument4 pagesThe Americanization of Mental Illnessfiona.tangNo ratings yet
- 2010JAN08 The Americanization of Mental Illness - NYTimesDocument8 pages2010JAN08 The Americanization of Mental Illness - NYTimescrljones100% (1)
- DSM and PhenomDocument5 pagesDSM and PhenomgauravtandonNo ratings yet
- Medicine and Literature Intersect to Improve Patient CareDocument7 pagesMedicine and Literature Intersect to Improve Patient CareRafael AnselméNo ratings yet
- DETEKSI TBDocument7 pagesDETEKSI TBSetiaty PandiaNo ratings yet
- Marginal Ridge Is Severely WeakenedDocument9 pagesMarginal Ridge Is Severely WeakenedChin GeslaniNo ratings yet
- Ronald R. Martel Celebrated As A Professional of The Year For 2022 by Strathmore's Who's Who Worldwide PublicationDocument4 pagesRonald R. Martel Celebrated As A Professional of The Year For 2022 by Strathmore's Who's Who Worldwide PublicationPR.comNo ratings yet
- WAB-R Calculator: Quickly Calculate AQ, LQ & CQ ScoresDocument7 pagesWAB-R Calculator: Quickly Calculate AQ, LQ & CQ ScoresKirsten King100% (2)
- Tooth Eruption & Shedding MechanismsDocument18 pagesTooth Eruption & Shedding MechanismsAnamika PandeyNo ratings yet
- CPS 2 ToxicologyDocument31 pagesCPS 2 ToxicologyNgọc Hà NguyễnNo ratings yet
- Post Mortem Report FinalDocument3 pagesPost Mortem Report Finalnupur jhodNo ratings yet
- B.inggris (Applying IV Infusion)Document2 pagesB.inggris (Applying IV Infusion)Renika Dwi WahyuniNo ratings yet
- NCM 120 LecDocument4 pagesNCM 120 LecJamaica Leslie NovenoNo ratings yet
- Practices of Exclusive Breastfeeding Among Lactating Mothers Attending Care at HoimaDocument7 pagesPractices of Exclusive Breastfeeding Among Lactating Mothers Attending Care at HoimaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Economy of Scale and Scope in Healthcare OperationsDocument22 pagesEconomy of Scale and Scope in Healthcare OperationsRavia SharmaNo ratings yet
- Love - Bondage or Liberation - A Psychological Exploration of The Meaning, Values and Dangers of Falling in Love PDFDocument209 pagesLove - Bondage or Liberation - A Psychological Exploration of The Meaning, Values and Dangers of Falling in Love PDFPurnendra SinghNo ratings yet
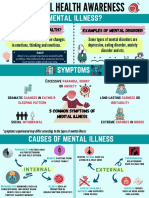
- Mental Health AwarenessDocument2 pagesMental Health Awarenessfarhatulhanimzulkifl100% (2)
- Partograph: Source: Basic Emergency Obstetric Care Dr. Jose Fabella Memorial Hospital, & Who By: Araceli F. SuratDocument33 pagesPartograph: Source: Basic Emergency Obstetric Care Dr. Jose Fabella Memorial Hospital, & Who By: Araceli F. SuratRaquel MonsalveNo ratings yet
- Case StudyDocument3 pagesCase StudyNovelyn B. PlaniaNo ratings yet
- Haeberle, Erwin - An Interview With Harry Benjamin (1985)Document4 pagesHaeberle, Erwin - An Interview With Harry Benjamin (1985)ArthurLeonardoDaCostaNo ratings yet
- OmniTurn Manual g3Document210 pagesOmniTurn Manual g3CESAR MTZNo ratings yet
- BULLDOZER - C52JSA-037 - Dozer Clearing of Existing Tracks in Jebel - 18-Mar-14Document6 pagesBULLDOZER - C52JSA-037 - Dozer Clearing of Existing Tracks in Jebel - 18-Mar-14hechame TamerhouletNo ratings yet
- Download Yatra App for Flight DetailsDocument3 pagesDownload Yatra App for Flight DetailsShafi Moznur AhmedNo ratings yet
- Strategy Implementation in Organizations A ConceptDocument14 pagesStrategy Implementation in Organizations A ConceptGemechis LemaNo ratings yet
- Edgar Allan Poe - The Facts in The Case of M. ValdemarDocument13 pagesEdgar Allan Poe - The Facts in The Case of M. ValdemarCem AvciNo ratings yet
- Ournal of Utrition Ollege: Journal of Nutrition CollegeDocument7 pagesOurnal of Utrition Ollege: Journal of Nutrition CollegeFathan Jundi RobbaniNo ratings yet
- Shine-On 22Document3 pagesShine-On 22I Gusti PradanaNo ratings yet
- Orthotic Intervention For The Hand and Upper Extremity Splinting PrinciplesDocument61 pagesOrthotic Intervention For The Hand and Upper Extremity Splinting Principleskevin.smart540No ratings yet
- Logic Models To Enhance Program PerformanceDocument32 pagesLogic Models To Enhance Program PerformanceCitra ManikNo ratings yet
- Gender EuphoriaDocument25 pagesGender EuphoriaillaritzaNo ratings yet
- Pre-Employment Requirements - KFC S-FZDocument1 pagePre-Employment Requirements - KFC S-FZJenalyn AmarNo ratings yet
- Summative Test (Health)Document3 pagesSummative Test (Health)Diego ConopioNo ratings yet
- Alphaplus® C24-28: Safety Data SheetDocument12 pagesAlphaplus® C24-28: Safety Data SheetlyesNo ratings yet
- Sicat Surgical Guide Manual PDFDocument56 pagesSicat Surgical Guide Manual PDFvashishtanatomyNo ratings yet