You might also like
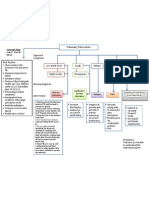
- Concept Map PTBDocument1 pageConcept Map PTBJoan Abardo100% (2)
- Basic Math Ability Exam A Relias Graded ADocument6 pagesBasic Math Ability Exam A Relias Graded ADebs MaxNo ratings yet
- Student Excursion Consent FormDocument4 pagesStudent Excursion Consent Formapi-276186998No ratings yet
- Non-Medical Endoscopists: British Society of GastroenterologyDocument11 pagesNon-Medical Endoscopists: British Society of GastroenterologyScott MackenzieNo ratings yet
- Pathophysiology of InflammationDocument50 pagesPathophysiology of InflammationElla Jones0% (1)
- Behavioral Health Care Plan: Assessment DataDocument9 pagesBehavioral Health Care Plan: Assessment Dataapi-521018364No ratings yet
- 2 Allergic DiseasesDocument27 pages2 Allergic DiseasesMuhammad AgussalimNo ratings yet
- Digestive System Diseases-Autonomo TaskDocument2 pagesDigestive System Diseases-Autonomo TaskMaily OrozcoNo ratings yet
- Pharmacology Test 2 Drug ListDocument33 pagesPharmacology Test 2 Drug ListSHRIKANTNo ratings yet
- Pharmacology Test 2 Drug List: CategorizedDocument33 pagesPharmacology Test 2 Drug List: CategorizedAniket SinghNo ratings yet
- 2 Anti Peptic Ulcer DiseasesDocument27 pages2 Anti Peptic Ulcer DiseasesAhmad YusrizalNo ratings yet
- Pharmacology Test 3 Drug ListDocument32 pagesPharmacology Test 3 Drug ListSHRIKANTNo ratings yet
- Anti BiotikDocument82 pagesAnti BiotikKaniaArfianiNo ratings yet
- Ocularpharmacologydr 160405034844Document73 pagesOcularpharmacologydr 160405034844vrajshekharNo ratings yet
- Mangifera Casturi in Thioglycollate-Induced LeukocyteDocument6 pagesMangifera Casturi in Thioglycollate-Induced LeukocyterabiatulNo ratings yet
- Fungal Treatment: Igri Septian Risky I11109018Document13 pagesFungal Treatment: Igri Septian Risky I11109018Igri Septian Risky DiaanNo ratings yet
- Drug StudyDocument13 pagesDrug StudyL Rean Carmelle MAGALLONESNo ratings yet
- Topik 11 - Fitoterapi Endokrin - GinekologiDocument48 pagesTopik 11 - Fitoterapi Endokrin - GinekologiIkaputri fNo ratings yet
- Occurrence of Tendon Pathologies in MetabolicDocument10 pagesOccurrence of Tendon Pathologies in MetabolicSebastián Jiménez GaticaNo ratings yet
- Li Windhu LBM 6 RespiDocument31 pagesLi Windhu LBM 6 RespiintaniafkuNo ratings yet
- Peptic Ulcer DiseaseDocument119 pagesPeptic Ulcer DiseaseJoy LacunaNo ratings yet
- Jurnal 2Document3 pagesJurnal 2MargaretaNo ratings yet
- AINESDocument86 pagesAINESFernandaNo ratings yet
- Drug Study - CaDocument3 pagesDrug Study - Casaint_ronald8No ratings yet
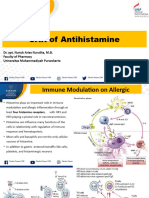
- 7 Sar AntihistaminDocument44 pages7 Sar AntihistaminGitasetya NingrumNo ratings yet
- Drug Action Indications and Contraindications Nursing ResponsibilitesDocument3 pagesDrug Action Indications and Contraindications Nursing ResponsibilitesGino B. BulanaNo ratings yet
- Fortune Vushe CH205 Assignment 1Document4 pagesFortune Vushe CH205 Assignment 1Fortune VusheNo ratings yet
- Drug Index: Generic/ Brand Name Dosage Mode of Action Indications Contraindications Adverse Effects Co AmoxiclavDocument3 pagesDrug Index: Generic/ Brand Name Dosage Mode of Action Indications Contraindications Adverse Effects Co AmoxiclavkNo ratings yet
- Treatment of Intestinal Permeability Defects Leaky Gut Corey Resnick Natural Medicine Journal 2010Document10 pagesTreatment of Intestinal Permeability Defects Leaky Gut Corey Resnick Natural Medicine Journal 2010Bariša KiršnerNo ratings yet
- Farmakologi Analgetik NSAID (Dr. Atina)Document56 pagesFarmakologi Analgetik NSAID (Dr. Atina)RidhaNo ratings yet
- Mycology AssignmentDocument9 pagesMycology AssignmenttenawNo ratings yet
- Gamutin Drug Study-PediatricsDocument6 pagesGamutin Drug Study-PediatricsJhulia GamutinNo ratings yet
- Gabungan TumcunDocument109 pagesGabungan Tumcuntarisa perolinNo ratings yet
- Kollazeb Presentation125Document11 pagesKollazeb Presentation125Ehsan AliNo ratings yet
- Article 1609836991Document9 pagesArticle 1609836991Read WhiteNo ratings yet
- Effects of Photodynamic Therapy in The Treatment of Mild To Moderate Acne VulgarisDocument5 pagesEffects of Photodynamic Therapy in The Treatment of Mild To Moderate Acne VulgarisCentral Asian StudiesNo ratings yet
- Drugs For GUTDocument11 pagesDrugs For GUTAyesha LiaqatNo ratings yet
- Introduction To Pharmacology: Prof. Johnny S. Bacud JR., RPH, Mspharm CandDocument81 pagesIntroduction To Pharmacology: Prof. Johnny S. Bacud JR., RPH, Mspharm Candlola&losa farhanNo ratings yet
- Pharmacology MidtermsDocument6 pagesPharmacology MidtermsConcepcion NazaredoNo ratings yet
- 14: Drugs Used in Malignant Diseases and For ImmunosuppressionDocument36 pages14: Drugs Used in Malignant Diseases and For ImmunosuppressionleonNo ratings yet
- In Vitro Antioxidant and Anti-Inflammatory Potential ofDocument13 pagesIn Vitro Antioxidant and Anti-Inflammatory Potential ofSabrina JonesNo ratings yet
- Pharmacotherapy of Acute Gout: Amit Gupta Roll No. 19Document15 pagesPharmacotherapy of Acute Gout: Amit Gupta Roll No. 19shashankNo ratings yet
- Inflamationppt 180928164511Document37 pagesInflamationppt 180928164511misdduaaNo ratings yet
- Uti ChemotherapyDocument13 pagesUti ChemotherapyKhadeer AGNo ratings yet
- Pharmacotherapy For Gastric Acidity, Peptic Ulcers, and Gastroesophageal Reflux DiseaseDocument10 pagesPharmacotherapy For Gastric Acidity, Peptic Ulcers, and Gastroesophageal Reflux DiseaseVera WatyNo ratings yet
- Amikacin 2Document2 pagesAmikacin 2Sian AsadaNo ratings yet
- Albumina en Cirrosis Descompensada 2020 BMJDocument12 pagesAlbumina en Cirrosis Descompensada 2020 BMJandreaNo ratings yet
- Medical ManagementDocument3 pagesMedical ManagementMark Jefferson LunaNo ratings yet
- Aminoglycosides AbsorptionDocument6 pagesAminoglycosides AbsorptionBella Fikka GamilaNo ratings yet
- PH Targeting in CancerDocument18 pagesPH Targeting in CancerSpore FluxNo ratings yet
- Day 12Document2 pagesDay 12Iiah Adda DiciniieNo ratings yet
- Cytoprotective Agents: Presented By: Guided byDocument53 pagesCytoprotective Agents: Presented By: Guided bydrfatimarizNo ratings yet
- Antibiotic IDocument11 pagesAntibiotic IMiloš KrstićNo ratings yet
- Pharma ExamDocument7 pagesPharma ExamGeno Adrian T PampangaNo ratings yet
- MID 2 PHARMA Anti-Infective DrugsDocument11 pagesMID 2 PHARMA Anti-Infective DrugsMariah Angela PinedaNo ratings yet
- Application of Colchicine, Side Effects, and Drug Interactions-2Document8 pagesApplication of Colchicine, Side Effects, and Drug Interactions-2Supun DhanushkaNo ratings yet
- Mycology AssignmentDocument7 pagesMycology AssignmenttenawNo ratings yet
- Screening The Anti Gout Traditional Herbs From TCM Using An in VitroDocument7 pagesScreening The Anti Gout Traditional Herbs From TCM Using An in VitroSanithaaaNo ratings yet
- Drug StudyDocument2 pagesDrug StudyChuchai AmbongNo ratings yet
- Clinical KHAIRANI's Antifungal AgentsDocument27 pagesClinical KHAIRANI's Antifungal AgentsRhomizal MazaliNo ratings yet
- 4 Sar AntibioticsDocument40 pages4 Sar AntibioticsGitasetya NingrumNo ratings yet
- Understanding Treatments For Gout: ReportsDocument8 pagesUnderstanding Treatments For Gout: ReportsTim LaneNo ratings yet
- Jurnal AjiDocument5 pagesJurnal Ajiajibagus prakosoNo ratings yet
- Hidroxicloroquina en El Tratamiento de Las Enfermedades Autoinmunes SistémicasDocument9 pagesHidroxicloroquina en El Tratamiento de Las Enfermedades Autoinmunes SistémicasGabriela Prado GumielNo ratings yet
- Pharamcology Unit 10 AnswersDocument13 pagesPharamcology Unit 10 AnswersLovren YoungNo ratings yet
- Science of Spices and Culinary Herbs - Latest Laboratory, Pre-clinical, and Clinical StudiesFrom EverandScience of Spices and Culinary Herbs - Latest Laboratory, Pre-clinical, and Clinical StudiesNo ratings yet
- Guidence Ipoi Operation SuccesDocument1 pageGuidence Ipoi Operation SuccesMuhammad AgussalimNo ratings yet
- Diabetes Prevention Knowledge and Perception of Risk AmongDocument7 pagesDiabetes Prevention Knowledge and Perception of Risk AmongMuhammad AgussalimNo ratings yet
- Risk of Etylen GlicolDocument1 pageRisk of Etylen GlicolMuhammad AgussalimNo ratings yet
- Ethylene Glycol Toxicosis in Animals - Toxicology - MSD Veterinary ManualDocument6 pagesEthylene Glycol Toxicosis in Animals - Toxicology - MSD Veterinary ManualMuhammad AgussalimNo ratings yet
- Intravenous Ketorolac Vs Diclofenac For AnalgesiaDocument6 pagesIntravenous Ketorolac Vs Diclofenac For AnalgesiaMuhammad AgussalimNo ratings yet
- Jurnal 1Document5 pagesJurnal 1Muhammad AgussalimNo ratings yet
- 1 s2.0 S2667147621000996 MainDocument5 pages1 s2.0 S2667147621000996 MainMuhammad AgussalimNo ratings yet
- Jurnal 2Document9 pagesJurnal 2Muhammad AgussalimNo ratings yet
- Jurnal 3Document21 pagesJurnal 3Muhammad AgussalimNo ratings yet
- Jurnal 6Document9 pagesJurnal 6Muhammad AgussalimNo ratings yet
- Jurnal 5Document13 pagesJurnal 5Muhammad AgussalimNo ratings yet
- Lipid Profile of Cholelithiasis Patients at Dr. Mohammad Hoesin Central General Hospital, PalembangDocument6 pagesLipid Profile of Cholelithiasis Patients at Dr. Mohammad Hoesin Central General Hospital, PalembangMuhammad AgussalimNo ratings yet
- Management Thoracic Pain 2019Document9 pagesManagement Thoracic Pain 2019Lotte WeggemanNo ratings yet
- Ncbi List of Books and Dental ArticlesDocument6 pagesNcbi List of Books and Dental ArticlesIulia Isacov0% (1)
- Understanding The RelapseDocument12 pagesUnderstanding The RelapseruziyanaNo ratings yet
- Urtricaria SDocument8 pagesUrtricaria SpalNo ratings yet
- Energy Drinks Are Bad RealDocument4 pagesEnergy Drinks Are Bad RealMadihi NorhadiNo ratings yet
- Wards and Departments in The Hospital NamingDocument4 pagesWards and Departments in The Hospital NamingSlebeww PetewNo ratings yet
- Feeling GreatDocument243 pagesFeeling GreatSunny LamNo ratings yet
- Treatment Modalities Applicable To The Psychiatric ClientDocument53 pagesTreatment Modalities Applicable To The Psychiatric Clientnickybore100% (1)
- McGrath Video Laryngoscope Rev 0.1Document6 pagesMcGrath Video Laryngoscope Rev 0.1adevasenNo ratings yet
- Mandibulasr Truma ManagementDocument18 pagesMandibulasr Truma Managementjoal510No ratings yet
- Classification of Tongue Cancer Resection and Treatment AlgorithmDocument8 pagesClassification of Tongue Cancer Resection and Treatment AlgorithmRahma WatiNo ratings yet
- E341 FullDocument7 pagesE341 FullwaribisalaNo ratings yet
- Castor OilDocument1 pageCastor OilRohan EarnestNo ratings yet
- Worksheet 4, Ubaidillah, 3BDocument6 pagesWorksheet 4, Ubaidillah, 3BUbay SegaNo ratings yet
- Etamsylate DS Meppo2010 PDFDocument3 pagesEtamsylate DS Meppo2010 PDFAqmarlia PutriNo ratings yet
- Pseudofollicular BabaeDocument13 pagesPseudofollicular BabaeOlamide EstherNo ratings yet
- AQ4PDocument3 pagesAQ4PAhmed GaberNo ratings yet
- Ultrasound Thesis TopicsDocument6 pagesUltrasound Thesis Topicsdw9x1bxb100% (2)
- Measuring Central Venous Pressure: Elaine ColeDocument8 pagesMeasuring Central Venous Pressure: Elaine ColednllkzaNo ratings yet
- Vertical Root Fracture !Document42 pagesVertical Root Fracture !Dr Dithy kkNo ratings yet
- CortisolDocument27 pagesCortisolCao YunNo ratings yet
- Full Body To Body Massage Centre in MG Road Gurgaon - Spa in Gurgaon MG RoadDocument11 pagesFull Body To Body Massage Centre in MG Road Gurgaon - Spa in Gurgaon MG RoadFlip Body SpaNo ratings yet
- Anesthesia-Assessing Depth PDFDocument1 pageAnesthesia-Assessing Depth PDFAvinash Technical ServiceNo ratings yet
- Tolak Angin TranslatedDocument3 pagesTolak Angin TranslatedWadz MuharNo ratings yet