You might also like
- Drug DiscoveryDocument397 pagesDrug DiscoveryJane Hanrahan100% (1)
- 100 Most Important DrugsDocument13 pages100 Most Important Drugsngopya djiki67% (3)
- Overview of Metabolism & The Provision of Metabolic Fuels (CHP 16 Harper) - TJLDocument6 pagesOverview of Metabolism & The Provision of Metabolic Fuels (CHP 16 Harper) - TJLMNo ratings yet
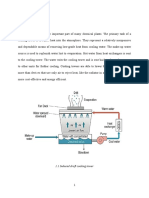
- Cooling Tower REPORTDocument25 pagesCooling Tower REPORTSaroj KumarNo ratings yet
- BT1000 - Cellular Metabolism PDFDocument35 pagesBT1000 - Cellular Metabolism PDFAnubhavAgarwal100% (1)
- Integration of Metabolism: Dr. Farzana Hakim Assistant Professor Biochemistry DepartmentDocument63 pagesIntegration of Metabolism: Dr. Farzana Hakim Assistant Professor Biochemistry DepartmentGriffinNo ratings yet
- CH 19 Integration of MetabolismDocument63 pagesCH 19 Integration of Metabolismshee140802100% (1)
- Intro To Metabo (IsmDocument8 pagesIntro To Metabo (IsmManila MedNo ratings yet
- Cell MetabolismDocument6 pagesCell MetabolismelsayidNo ratings yet
- Overview of Metabolism-1Document17 pagesOverview of Metabolism-1gospel munkondyaNo ratings yet
- 2011 03 15 Clariant - Corrosion Inhibitors and Corrosion Inhibitor SelectionDocument31 pages2011 03 15 Clariant - Corrosion Inhibitors and Corrosion Inhibitor SelectionVivek PatilNo ratings yet
- Introduction To MetabolismDocument33 pagesIntroduction To Metabolismlovelots123488% (16)
- Metabolic Concepts (Lecture 1-3)Document8 pagesMetabolic Concepts (Lecture 1-3)atifzea100% (1)
- Metabolism 1Document41 pagesMetabolism 1mukesh100% (1)
- Antimicrobial DrugsDocument64 pagesAntimicrobial Drugsdr. khushboo singh100% (1)
- Enzymes MCQ Topic Quiz Lesson ElementDocument19 pagesEnzymes MCQ Topic Quiz Lesson ElementArvin DiNozzoNo ratings yet
- The Fate of Metabolism Andmabolic PathwaysDocument25 pagesThe Fate of Metabolism Andmabolic PathwaysXuân Vi100% (1)
- IntgarationDocument94 pagesIntgarationfikaduNo ratings yet
- 16 HF 114 Introduction To MetabolismDocument26 pages16 HF 114 Introduction To Metabolismqueenmasa191No ratings yet
- SEM VI BOTANY C13T Plant MetabolismDocument10 pagesSEM VI BOTANY C13T Plant MetabolismAtashi MandalNo ratings yet
- K 19 20 Metabolism RegulationDocument29 pagesK 19 20 Metabolism RegulationIrfan MohammadNo ratings yet
- Metabolic Interrelationships Rev 2020-Lecture-StdsDocument79 pagesMetabolic Interrelationships Rev 2020-Lecture-StdsKavin AbdurrahiemNo ratings yet
- Mid Biochem: 7. Metabolism Is The Reactions Occurring in A Living Sysstem That Produce and Consume The EnergyDocument2 pagesMid Biochem: 7. Metabolism Is The Reactions Occurring in A Living Sysstem That Produce and Consume The EnergyNguyễn Bá Đạt100% (1)
- Carbohydrate Distribution, Metabolism, and ExcretionDocument93 pagesCarbohydrate Distribution, Metabolism, and ExcretionPSPD - Hana Athaya NNo ratings yet
- Gluconeogenesis, Glycogen Metabolism, and The Pentose Phosphate PathwayDocument24 pagesGluconeogenesis, Glycogen Metabolism, and The Pentose Phosphate PathwayMelisa Halilovic100% (1)
- Metabolic PathwaysDocument19 pagesMetabolic PathwaysAchmad IjaziNo ratings yet
- Biochemistry Final - Integrated - Metabolism-16Document113 pagesBiochemistry Final - Integrated - Metabolism-16keisha jonesNo ratings yet
- Integration of MetabolismDocument17 pagesIntegration of MetabolismSharif M Mizanur RahmanNo ratings yet
- Lecture 2.introduction To Metabolism. Specific and General Pathways of Carbohydrates, Lipids and Proteins Metabolism.Document16 pagesLecture 2.introduction To Metabolism. Specific and General Pathways of Carbohydrates, Lipids and Proteins Metabolism.shani9976614No ratings yet
- Lecture 02. Common Metabolic Pathways. Biological Oxidation. Tissue Respiration. Oxidative PhosphorylationDocument53 pagesLecture 02. Common Metabolic Pathways. Biological Oxidation. Tissue Respiration. Oxidative PhosphorylationВіталій Михайлович НечипорукNo ratings yet
- Week 2 Lesson 2Document18 pagesWeek 2 Lesson 2Yury DesuNo ratings yet
- Anabolism: The Use of Energy in Biosynthesis: Chapter OverviewDocument5 pagesAnabolism: The Use of Energy in Biosynthesis: Chapter OverviewElishae SamonteNo ratings yet
- Introduction To MetabolismDocument49 pagesIntroduction To Metabolismmaxwell amponsahNo ratings yet
- Technological Institute of The Philippines Quiapo, ManilaDocument10 pagesTechnological Institute of The Philippines Quiapo, ManilaKrystel LahomNo ratings yet
- LECTURE 2 - Carbohydrate MetabolismDocument60 pagesLECTURE 2 - Carbohydrate Metabolismmuhammedgmdidra95No ratings yet
- Biochem 2.1 Introduction To MetabolismDocument5 pagesBiochem 2.1 Introduction To Metabolismlovelots1234No ratings yet
- Drug MetabolismDocument25 pagesDrug MetabolismAbida AttaNo ratings yet
- 2022C Biochemistry Le 3 Objectives ListDocument1 page2022C Biochemistry Le 3 Objectives ListManila MedNo ratings yet
- Nutrient MetabolismDocument40 pagesNutrient MetabolismKaaviyaNo ratings yet
- Regulation of Metabolism-2Document14 pagesRegulation of Metabolism-2Marvin JeaNo ratings yet
- Biochemistry IIDocument56 pagesBiochemistry IITrescia Mae EstilloreNo ratings yet
- 8 Carbohydrate Metabolism PDFDocument36 pages8 Carbohydrate Metabolism PDFDayne Ocampo-SolimanNo ratings yet
- WUCHS Protein Lecture Note For Medical StudentsDocument361 pagesWUCHS Protein Lecture Note For Medical StudentsZelalem bekeleNo ratings yet
- Anabolism - Microbial MetabolismDocument28 pagesAnabolism - Microbial MetabolismDni AwatifNo ratings yet
- CARBOHYDRATE METABOLISM-DrSangitaDocument34 pagesCARBOHYDRATE METABOLISM-DrSangitaA MINOR100% (1)
- Integrated Metabolism Lec02Document35 pagesIntegrated Metabolism Lec02Fateha HussainNo ratings yet
- 4.2 - Metabolism and Metabolic PathwaysDocument3 pages4.2 - Metabolism and Metabolic PathwayscarlNo ratings yet
- 2.regulation of Metabolic PathwaysDocument14 pages2.regulation of Metabolic PathwaysProtusha RakshitNo ratings yet
- Intensive Course 2016 2017 Principles of Biochemistry: Prof Nik Norulaini Nik Ab RahmanDocument73 pagesIntensive Course 2016 2017 Principles of Biochemistry: Prof Nik Norulaini Nik Ab RahmanJayanthi LoganathanNo ratings yet
- Muscle Energy Metabolsm For MedicineDocument69 pagesMuscle Energy Metabolsm For MedicinefikaduNo ratings yet
- MODULE - FINALS - Biochem - 1Document5 pagesMODULE - FINALS - Biochem - 1Cyril CauilanNo ratings yet
- Metabolism OverviewDocument43 pagesMetabolism OverviewWinnet MaruzaNo ratings yet
- 1 Bioenegretics and MetabolismDocument60 pages1 Bioenegretics and MetabolismlikeleliletabaNo ratings yet
- Biochem NursingDocument144 pagesBiochem Nursingabukaritoyibu100No ratings yet
- Cellular Metabolism Overview of MetabolismDocument4 pagesCellular Metabolism Overview of MetabolismNathan Louis PalacioNo ratings yet
- BioenergeticsDocument4 pagesBioenergeticsMahnoor MansoorNo ratings yet
- Biochemistry: Introduction To MetabolismDocument7 pagesBiochemistry: Introduction To MetabolismAria ScribeNo ratings yet
- Biochemistry 2016 Spring Chapter17 19Document121 pagesBiochemistry 2016 Spring Chapter17 19krismarie94No ratings yet
- Carbohydrate MetabolismDocument139 pagesCarbohydrate MetabolismMarshall AzekeNo ratings yet
- Metabolisme Makronutrien FixDocument132 pagesMetabolisme Makronutrien FixbelaariyantiNo ratings yet
- Chapter 10-Integration of MetabolismDocument4 pagesChapter 10-Integration of MetabolismJenelyn Lanang DiariosNo ratings yet
- 2223 L1 Metabolism (STDS)Document21 pages2223 L1 Metabolism (STDS)Dhanen DranNo ratings yet
- Handout Biokimia LanjutDocument111 pagesHandout Biokimia Lanjuttheresia nababanNo ratings yet
- Metabolism Complete Notes #KigogoDocument145 pagesMetabolism Complete Notes #KigogoHesbone AneneNo ratings yet
- MetabolismDocument51 pagesMetabolismHanna YajNo ratings yet
- Mechanisms and Regulation of Carbohydrate Transport in BacteriaFrom EverandMechanisms and Regulation of Carbohydrate Transport in BacteriaNo ratings yet
- Muscle Energy Metabolsm For MedicineDocument69 pagesMuscle Energy Metabolsm For MedicinefikaduNo ratings yet
- ENZYMES For MedicineDocument127 pagesENZYMES For MedicinefikaduNo ratings yet
- Enzyme 1Document115 pagesEnzyme 1fikaduNo ratings yet
- Metabolism Interaction and Hormone Regulation.Document81 pagesMetabolism Interaction and Hormone Regulation.fikaduNo ratings yet
- Research ProposalDocument5 pagesResearch ProposalfikaduNo ratings yet
- @ CRHR Medicine Curriculum Final Ambo UniversityDocument42 pages@ CRHR Medicine Curriculum Final Ambo Universityfikadu100% (1)
- PHA-Learning Module - Work Place Safety IIDocument65 pagesPHA-Learning Module - Work Place Safety IIfikaduNo ratings yet
- Ambo University Legislation 2013Document241 pagesAmbo University Legislation 2013fikaduNo ratings yet
- Berberine - Scientific Review On Usage, Dosage, Side Effects - ExamineDocument51 pagesBerberine - Scientific Review On Usage, Dosage, Side Effects - Examineozman blooriNo ratings yet
- Figure 1.1: General Structure of Schiff BaseDocument15 pagesFigure 1.1: General Structure of Schiff Basedipto dasNo ratings yet
- HND Sector 2 Vol3-1Document530 pagesHND Sector 2 Vol3-1mbabit leslieNo ratings yet
- Oxidative Phosphorylation V Inhibitors and UncouplersDocument15 pagesOxidative Phosphorylation V Inhibitors and UncouplersIffatnazNo ratings yet
- 8.1 (2.5 HL)Document21 pages8.1 (2.5 HL)SudeNo ratings yet
- Antioxidant and Inhibition of Their Fractions of Ashitaba (Angelica Keiskei)Document4 pagesAntioxidant and Inhibition of Their Fractions of Ashitaba (Angelica Keiskei)yuli fitrianaNo ratings yet
- Discussion and ConclusionDocument4 pagesDiscussion and ConclusionRisma WerdaningsihNo ratings yet
- 1 s2.0 S1093326316300055 MainDocument11 pages1 s2.0 S1093326316300055 MainChinar PatelNo ratings yet
- BGR 34 BrochureDocument10 pagesBGR 34 Brochureydee28No ratings yet
- Frye and Edidin PaperDocument18 pagesFrye and Edidin PaperJonathan ShaoNo ratings yet
- Phle Module 4Document135 pagesPhle Module 4Margaret RNo ratings yet
- Solution Manual For Biochemistry A Short Course 3rd by TymoczkoDocument36 pagesSolution Manual For Biochemistry A Short Course 3rd by Tymoczkocabecadrawable.sxfi2c100% (44)
- Week 2 - Enzyme Kinetics All - v2 - 3slide HandoutsDocument14 pagesWeek 2 - Enzyme Kinetics All - v2 - 3slide HandoutsFizza HussainNo ratings yet
- Full Download Book Basic Clinical Pharmacology 15Th Edition PDFDocument41 pagesFull Download Book Basic Clinical Pharmacology 15Th Edition PDFalvin.vincent421100% (15)
- Lecture 5 - Enzymes Part 1Document15 pagesLecture 5 - Enzymes Part 1Fea Kristine PacquiaoNo ratings yet
- 1955 - Inhibition of HyaluronidaseDocument22 pages1955 - Inhibition of HyaluronidasekamilNo ratings yet
- Kami Export - Lab 8 Enzymes Answer SheetDocument3 pagesKami Export - Lab 8 Enzymes Answer SheetMonica OchoaNo ratings yet
- 3 Enzymes - MCQ QPDocument4 pages3 Enzymes - MCQ QPVivehaNo ratings yet
- 10A Review Questions 2015Document10 pages10A Review Questions 2015TheBoss 20No ratings yet
- Revision Notes For Class 12 CBSE Chemistry, Chemistry in Everyday Life - TopperlearningDocument8 pagesRevision Notes For Class 12 CBSE Chemistry, Chemistry in Everyday Life - TopperlearningRishabh Bhandari100% (1)
- Pharmacology - Mechanism of Action of All Drugs - +Document4 pagesPharmacology - Mechanism of Action of All Drugs - +Sahal ShaikhNo ratings yet
- Digestion Enzyme Practice TestDocument15 pagesDigestion Enzyme Practice TestJila HafiziNo ratings yet
- 1.production of Bioactive Peptides During Soybean Fermentation and Their Potential Health BenefitsDocument10 pages1.production of Bioactive Peptides During Soybean Fermentation and Their Potential Health BenefitsEva Mayte GuadarramaNo ratings yet
- 8.1 Metabolism Assessment StatementsDocument1 page8.1 Metabolism Assessment Statementspraata123No ratings yet