You might also like
- Gynecology PDFDocument18 pagesGynecology PDFKatheryn100% (2)
- Psychotherapist and Wiccan Clergy: The Ethics of A Dual Relationship by Ellen C. FriedmanDocument22 pagesPsychotherapist and Wiccan Clergy: The Ethics of A Dual Relationship by Ellen C. FriedmanNUR ZULYDIA BINTI ABU KARIMNo ratings yet
- AmenorrheaDocument23 pagesAmenorrheaKarmmanya Razahani PurnamaNo ratings yet
- Reproductive HormonesDocument43 pagesReproductive HormonesMunchkin CelinaNo ratings yet
- Physical Education 10 Las No.1 Week1 2 Fourth QuarterDocument2 pagesPhysical Education 10 Las No.1 Week1 2 Fourth QuarterTheresa Vasquez Vicente100% (1)
- AmenorrheaDocument41 pagesAmenorrheaBonitavanyNo ratings yet
- Dr. Shehla Jamal Assistant Professor: OBG S M S & RDocument69 pagesDr. Shehla Jamal Assistant Professor: OBG S M S & RAppy LoveNo ratings yet
- Infertility 001Document257 pagesInfertility 001Habtamu Nigussie100% (1)
- Unit 8. Cholinergic and AnticholinergicsDocument50 pagesUnit 8. Cholinergic and AnticholinergicsApril Mergelle LapuzNo ratings yet
- Menstrual CycleDocument45 pagesMenstrual CycleChari RivoNo ratings yet
- SBM Reproduction NotesDocument73 pagesSBM Reproduction NotesAhra100% (2)
- CHN ReportDocument16 pagesCHN Reportash aliNo ratings yet
- Clinical Guidelines ForDocument54 pagesClinical Guidelines ForHenry SudharsonoNo ratings yet
- 4.primary - Secondary AmenorrheaDocument5 pages4.primary - Secondary AmenorrheaAhmed Al GhaithiNo ratings yet
- 3 AmenorrrheaDocument29 pages3 AmenorrrheaKilp MosesNo ratings yet
- Chapter 27. Amenorrhea: Berek & Novak's Gynecology 14 Edition (P 1035 1068) R3 Jung Mi ByunDocument95 pagesChapter 27. Amenorrhea: Berek & Novak's Gynecology 14 Edition (P 1035 1068) R3 Jung Mi Byunhossam626No ratings yet
- Absence of A Menstrual PeriodDocument2 pagesAbsence of A Menstrual PeriodDragan PetrovicNo ratings yet
- AmenorrheaDocument26 pagesAmenorrheaThatStudentNo ratings yet
- 4.4 (Amenorrhea) University of AlexanderDocument28 pages4.4 (Amenorrhea) University of AlexanderAnonymous XSXlZJvyWNo ratings yet
- Amenorrhea PDFDocument5 pagesAmenorrhea PDFKenneth Robin CarbonellNo ratings yet
- Amenorrhea: Stelian Hodorogea, Associate ProfessorDocument73 pagesAmenorrhea: Stelian Hodorogea, Associate ProfessorgvfhgNo ratings yet
- 2 AmenorrheaDocument41 pages2 AmenorrheaKilp MosesNo ratings yet
- MEETING 6 AmenorrheaDocument41 pagesMEETING 6 AmenorrheaNader KhouryNo ratings yet
- Primary Amenorrhea: Rabika Almina RabiaDocument30 pagesPrimary Amenorrhea: Rabika Almina RabiaAlmina RehmanNo ratings yet
- Amen or RheaDocument41 pagesAmen or Rheakhadzx100% (2)
- AmenorrheaDocument41 pagesAmenorrheadoraNo ratings yet
- Primary Amenorrhoea 2Document42 pagesPrimary Amenorrhoea 2sivaNo ratings yet
- First Aid For The OBS&GYN Clerkship CH 17 (Amenorrhea)Document9 pagesFirst Aid For The OBS&GYN Clerkship CH 17 (Amenorrhea)黃芳昌No ratings yet
- Aditiawati - No Signs of Puberty PDFDocument43 pagesAditiawati - No Signs of Puberty PDFJayantiNo ratings yet
- AmenorrheaDocument51 pagesAmenorrheabisharatNo ratings yet
- AmenorrheaDocument55 pagesAmenorrheaAla AbushehabNo ratings yet
- AmenorrheaDocument41 pagesAmenorrheaarfahregarNo ratings yet
- GynecologyDocument27 pagesGynecologyDaniel Dwi NugrohoNo ratings yet
- Sindrom Turner Stein Leventhal TB Pelvis: Chest) and WidelyDocument2 pagesSindrom Turner Stein Leventhal TB Pelvis: Chest) and WidelyAris BudiNo ratings yet
- Sexuality and IntersexualityDocument23 pagesSexuality and IntersexualityManu BharadwazNo ratings yet
- Laporan Tutorial V: Tutor: Dr. Amir Fauzi, SP - OgDocument29 pagesLaporan Tutorial V: Tutor: Dr. Amir Fauzi, SP - OgmpurboNo ratings yet
- Amenorrhoea 5thyr DR KKDocument56 pagesAmenorrhoea 5thyr DR KKpmj050gpNo ratings yet
- Hypothalamus-Pituitary-Gonad. Female Sex Hormones: Rishabh Kumar LD-212Document18 pagesHypothalamus-Pituitary-Gonad. Female Sex Hormones: Rishabh Kumar LD-212Ankit KumarNo ratings yet
- Haid Patologis: Ramadina, SpogDocument21 pagesHaid Patologis: Ramadina, SpogOoy RokayahNo ratings yet
- AmenorrhoeaDocument38 pagesAmenorrhoeaheydydNo ratings yet
- Laboratory Investigation of Amenorrhea:: DefinitionsDocument8 pagesLaboratory Investigation of Amenorrhea:: DefinitionsAmelia SetiawatiNo ratings yet
- Amenorrhea - DrPrekshyaDocument44 pagesAmenorrhea - DrPrekshyaasdfNo ratings yet
- من دون عنوانDocument50 pagesمن دون عنوانjjeddawNo ratings yet
- OB - GYN (5) - Alaa SalmanppDocument6 pagesOB - GYN (5) - Alaa Salmanppmotasem.med120No ratings yet
- Rimary Menorrhea: By: Zaineb Talib Nimaa Zahra Ali Hasoon Zina Safaa AldienDocument28 pagesRimary Menorrhea: By: Zaineb Talib Nimaa Zahra Ali Hasoon Zina Safaa AldienZaineb TalibNo ratings yet
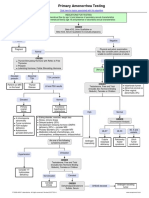
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmGabriella AguirreNo ratings yet
- IVF Infertility Treatment IndiaDocument26 pagesIVF Infertility Treatment India24x7emarketing100% (1)
- AmenorrheaDocument41 pagesAmenorrheaDewi Felayati Gusni100% (2)
- Sexual Differentiation Anomalies+Puberty - PPT Fara PozeDocument49 pagesSexual Differentiation Anomalies+Puberty - PPT Fara PozeAmira AsaadNo ratings yet
- Amenorrhea, Hirsutism, VirilismDocument12 pagesAmenorrhea, Hirsutism, VirilismAly MorganNo ratings yet
- First Aid For The OBS&GYN Clerkship CH 14 (Menstruation)Document4 pagesFirst Aid For The OBS&GYN Clerkship CH 14 (Menstruation)黃芳昌No ratings yet
- Primary AmenorrheaDocument33 pagesPrimary AmenorrheaZaraNo ratings yet
- Physio Bull BORRABLEDocument11 pagesPhysio Bull BORRABLEfrhasseyNo ratings yet
- AmennorheaDocument14 pagesAmennorheakutra3000No ratings yet
- Menstruation and Bleeding Conditions in Women and AdolescentsDocument123 pagesMenstruation and Bleeding Conditions in Women and AdolescentsBritanny NelsonNo ratings yet
- Endocrine and Reproductive Pharmacology-By:Dr. DHIREN BHOIDocument77 pagesEndocrine and Reproductive Pharmacology-By:Dr. DHIREN BHOIdrdhirenvet100% (9)
- Female PubertyDocument24 pagesFemale PubertyHeba Khalid Al-HashmeyNo ratings yet
- Secondary AmenorrheaDocument3 pagesSecondary AmenorrheageldeveraNo ratings yet
- Stress Hormone, Any Form of Stress It Is Elevated Pituitary Lactogenic HormoneDocument3 pagesStress Hormone, Any Form of Stress It Is Elevated Pituitary Lactogenic HormoneAthalia amaris SanchezNo ratings yet
- Physical Growth and Development During AdolescenceDocument54 pagesPhysical Growth and Development During AdolescencereemmajzoubNo ratings yet
- Balancing Hormones Naturally: A Woman's Guide to Hormonal Harmony: HealthFrom EverandBalancing Hormones Naturally: A Woman's Guide to Hormonal Harmony: HealthNo ratings yet
- Safety Data Sheet: Page 1 of 6 Msds For #01037 - Testor Enamel PaintDocument6 pagesSafety Data Sheet: Page 1 of 6 Msds For #01037 - Testor Enamel PaintJake VergaraNo ratings yet
- 03 - A Hipertrofia Muscular É Afetada Por Modelos de Progressão de Carga de VolumeDocument6 pages03 - A Hipertrofia Muscular É Afetada Por Modelos de Progressão de Carga de Volumealan.consultoriafitnessNo ratings yet
- Environmental Engineering - Gupta & GuptaDocument760 pagesEnvironmental Engineering - Gupta & GuptaRajat RathoreNo ratings yet
- HEROIC RPG v2.1Document23 pagesHEROIC RPG v2.1Layon RodriguesNo ratings yet
- Quiz On ReadingDocument4 pagesQuiz On ReadingMilagros Rodriguez (Mili)No ratings yet
- YsealDocument4 pagesYsealMuhammad Reza Agung SadewaNo ratings yet
- Kuesioner Kualitas HidupDocument9 pagesKuesioner Kualitas HidupRetno ManggalihNo ratings yet
- Chapter 4 Business Ethics and Social Responsibility Student NotesDocument2 pagesChapter 4 Business Ethics and Social Responsibility Student NotesSpandanXalxo100% (3)
- Exercise Rehabilitation For Smartphone Addiction: Review ArticleDocument6 pagesExercise Rehabilitation For Smartphone Addiction: Review ArticlePlitaniumNo ratings yet
- High KVP Technique Portable Chest X RayDocument31 pagesHigh KVP Technique Portable Chest X Rayjturos2003No ratings yet
- Mom ShamingDocument3 pagesMom ShamingIva DivacNo ratings yet
- NCM 102 Demo BrochureDocument2 pagesNCM 102 Demo BrochureTrisha Mikaela CaguladaNo ratings yet
- Asmita Saini CVDocument3 pagesAsmita Saini CVasmi94No ratings yet
- AI Impact On Employee Work Performance and Employee Morale in The Philippines A Literature Review - Docx13Document15 pagesAI Impact On Employee Work Performance and Employee Morale in The Philippines A Literature Review - Docx13pecataasenov100% (1)
- PE-10-Quarter2-Week3-4-Module2 (Health&Wellness) - Baltazar - Ramil.et AlDocument16 pagesPE-10-Quarter2-Week3-4-Module2 (Health&Wellness) - Baltazar - Ramil.et AlShekinah Joy Arellano ViloriaNo ratings yet
- Pathology of The Integumentary System: References: Http://people - Upei.ca/hannaDocument22 pagesPathology of The Integumentary System: References: Http://people - Upei.ca/hannaLakshita PrajapatiNo ratings yet
- The Impact of Telehealth Consultations On Adolescent Type II Diabetes 1Document5 pagesThe Impact of Telehealth Consultations On Adolescent Type II Diabetes 1Shilah chepkemboiNo ratings yet
- Research ClassifiedDocument6 pagesResearch ClassifiedPatricia OrtegaNo ratings yet
- Admission Test For PHD in Molecular BiologyDocument1 pageAdmission Test For PHD in Molecular BiologysbspuNo ratings yet
- Health Benefits of Prebiotics and Probiotics: Specialty "Food "Document18 pagesHealth Benefits of Prebiotics and Probiotics: Specialty "Food "Alexandra Ioan100% (1)
- The Life and Culture of The Indigenous PeopleDocument2 pagesThe Life and Culture of The Indigenous PeopleJustine Airra OndoyNo ratings yet
- Pharmacy Thesis TitlesDocument8 pagesPharmacy Thesis TitlesEssayHelperAlbuquerque100% (4)
- Analisis Iklan Layanan Masyarakat COVID-19 - Versi Kementerian Kesehatan RIDocument7 pagesAnalisis Iklan Layanan Masyarakat COVID-19 - Versi Kementerian Kesehatan RIAmira TifaliaNo ratings yet
- Internship Project Report On Mobile-Health Applications For The Efficient Delivery of Health Care Facility To People: - A Survey On Woodland RPGDocument42 pagesInternship Project Report On Mobile-Health Applications For The Efficient Delivery of Health Care Facility To People: - A Survey On Woodland RPGBishal RoyNo ratings yet
- Health Care Career TreeDocument1 pageHealth Care Career TreefruitcNo ratings yet
- Before Hon'Ble Judicial Magistrate First Class. at BhokarDocument3 pagesBefore Hon'Ble Judicial Magistrate First Class. at BhokarBhupendra ChavanNo ratings yet