You might also like
- Abnormal PuerperiumDocument21 pagesAbnormal PuerperiumNatukunda DianahNo ratings yet
- V Upashama PrakaranamDocument488 pagesV Upashama PrakaranamantiX LinuxNo ratings yet
- Islamic ArchitectureDocument84 pagesIslamic ArchitecturesidNo ratings yet
- Postpartum ComplicationsDocument16 pagesPostpartum Complicationshoohoo100% (1)
- Virgin Galactic Profile & Performance Business ReportDocument10 pagesVirgin Galactic Profile & Performance Business ReportLoic PitoisNo ratings yet
- Postpartum ComplicationsDocument7 pagesPostpartum ComplicationsCarlo BerzNo ratings yet
- PTV Vissim - First Steps ENG PDFDocument34 pagesPTV Vissim - First Steps ENG PDFBeby RizcovaNo ratings yet
- Postpartum Period (Complications)Document3 pagesPostpartum Period (Complications)Isabel BangalaoNo ratings yet
- Midterm Nucama 460Document7 pagesMidterm Nucama 460Reysel MonteroNo ratings yet
- Clinical TeachingDocument21 pagesClinical Teachingtanmai nooluNo ratings yet
- NCM 109 (OB) - 4.1 Nursing Care of The Postpartum ClientDocument9 pagesNCM 109 (OB) - 4.1 Nursing Care of The Postpartum ClientKristine Joyce Bongao BediaNo ratings yet
- High Risk Postpartum Client ReviewerDocument6 pagesHigh Risk Postpartum Client ReviewerArianJubaneNo ratings yet
- Abnormalities of The Puerperium: Puerperal PyrexiaDocument28 pagesAbnormalities of The Puerperium: Puerperal Pyrexiadrravindermehetrey100% (2)
- Module 5 - MCN TransesDocument6 pagesModule 5 - MCN TransesCarl UyNo ratings yet
- Placenta Previa (OB)Document4 pagesPlacenta Previa (OB)Winj BudayNo ratings yet
- Upper Genital Tract InfectionDocument2 pagesUpper Genital Tract InfectiondanielNo ratings yet
- MCN 80 114Document35 pagesMCN 80 114Jianne CaloNo ratings yet
- Reviewer in NCMDocument12 pagesReviewer in NCMtamsmadjad18No ratings yet
- Module 5 - MCN TransesDocument6 pagesModule 5 - MCN TransesCarl UyNo ratings yet
- MCN II Puerperal Infection 1Document23 pagesMCN II Puerperal Infection 1Rafik LakhdarNo ratings yet
- Metritis With Pelvic CellulitisDocument2 pagesMetritis With Pelvic CellulitisCleoGomezNo ratings yet
- Ob2 Sas 13Document8 pagesOb2 Sas 13Ralph Louie ManagoNo ratings yet
- Presentation 1Document6 pagesPresentation 1Sherylou Kumo SurioNo ratings yet
- Chapter 23 ContinuationDocument7 pagesChapter 23 ContinuationArabelle GO100% (1)
- Antepartal ComplicationsDocument13 pagesAntepartal ComplicationsJennie KimNo ratings yet
- Obstetrics Cards 19 30 PDFDocument81 pagesObstetrics Cards 19 30 PDFNavid BabluNo ratings yet
- Puerperal SepsisDocument4 pagesPuerperal SepsisSonali NayakNo ratings yet
- Perineal SputumDocument8 pagesPerineal SputumYellowNo ratings yet
- Obstetrics - Puerperal InfectionDocument4 pagesObstetrics - Puerperal InfectionJonathanNo ratings yet
- OB - Puerperal ComplicationsDocument5 pagesOB - Puerperal ComplicationsDarren Mae MosadaNo ratings yet
- STI&STDDocument5 pagesSTI&STDRica Joy Sulicipan FiestaNo ratings yet
- Subinvolution of The UterusDocument5 pagesSubinvolution of The UterusJanica Rose Maloloy-onNo ratings yet
- Precipitate Labor and DeliveryDocument2 pagesPrecipitate Labor and Deliverymyer pasandalanNo ratings yet
- Sumu PDFDocument30 pagesSumu PDFalokpalreshaNo ratings yet
- Placental AbnormalitiesDocument5 pagesPlacental AbnormalitiesNica Lopez FernandezNo ratings yet
- MCN NotesDocument20 pagesMCN NotesLiamLexus JavierNo ratings yet
- Postpartal ComplicationDocument4 pagesPostpartal ComplicationHanna AligatoNo ratings yet
- Abortion ReportDocument3 pagesAbortion ReportnengskNo ratings yet
- IMMUNOLOGY Student Ver 2024Document17 pagesIMMUNOLOGY Student Ver 2024Sogan, MaureenNo ratings yet
- Ob2 Sas 14Document5 pagesOb2 Sas 14Ralph Louie ManagoNo ratings yet
- Module 14 Care of A Family Experiencing A Postpartum Complication Puerperal 1Document14 pagesModule 14 Care of A Family Experiencing A Postpartum Complication Puerperal 1Blair AnnNo ratings yet
- Circulatory System Infectious Diseases: Dengue Hemorrhagic Shock SyndromeDocument3 pagesCirculatory System Infectious Diseases: Dengue Hemorrhagic Shock Syndromegrazelantonette.calubNo ratings yet
- Vrebsc 180521172503Document16 pagesVrebsc 180521172503D. Melba S.S ChinnaNo ratings yet
- Abruptio Placentae: Moses Quinanola Oral Revalida 2 SemesterDocument6 pagesAbruptio Placentae: Moses Quinanola Oral Revalida 2 SemesterBrian OrejudosNo ratings yet
- AbortionDocument1 pageAbortionMohiuddin AhmedNo ratings yet
- Patologi Sistem Reproduksi WanitaDocument5 pagesPatologi Sistem Reproduksi WanitaAnjayNo ratings yet
- Puerperal InfectionsDocument18 pagesPuerperal InfectionsJkimNo ratings yet
- PMC503 Parasitology Nematoda 1 2022Document33 pagesPMC503 Parasitology Nematoda 1 2022Adam DiabNo ratings yet
- PMC503 Parasitology Nematoda 1 2022Document33 pagesPMC503 Parasitology Nematoda 1 2022Adam DiabNo ratings yet
- TRANS NOTES For CH16Document5 pagesTRANS NOTES For CH16Patricia CabisonNo ratings yet
- Uncommon Presentation of Necrotizing Fasciitis Affe - 2024 - International JournDocument7 pagesUncommon Presentation of Necrotizing Fasciitis Affe - 2024 - International JournRonald QuezadaNo ratings yet
- Subacute Uterine Inversion With Shock - A Distinct Surgical ManagementDocument3 pagesSubacute Uterine Inversion With Shock - A Distinct Surgical ManagementBima GhovaroliyNo ratings yet
- Fibroids: 1. Red DegenerationDocument2 pagesFibroids: 1. Red Degenerationcgao30No ratings yet
- HIGH RISK AND SICK MOTHER 5PsDocument16 pagesHIGH RISK AND SICK MOTHER 5Psbaracream.exeNo ratings yet
- Module 2 - MCN TransesDocument6 pagesModule 2 - MCN TransesCarl UyNo ratings yet
- MCN MIDTERM Post BreastDocument15 pagesMCN MIDTERM Post BreastkaiaslayNo ratings yet
- NCM 109 Midterms M1 M4 1 2Document47 pagesNCM 109 Midterms M1 M4 1 2bsn1kgangNo ratings yet
- Fetal DevelopmentDocument5 pagesFetal DevelopmentHazelGraceNo ratings yet
- SGD 2Document1 pageSGD 2Thea PepitoNo ratings yet
- Gynae Study MaterialDocument3 pagesGynae Study MaterialAyeshik ChakrabortyNo ratings yet
- Endometritis BrochureDocument2 pagesEndometritis BrochureNovelyn PuaNo ratings yet
- Abnormalities of PuerperiumDocument70 pagesAbnormalities of PuerperiumYasmin SharmaNo ratings yet
- Typhoid FeverDocument3 pagesTyphoid FeverKrista CabelloNo ratings yet
- Bourbon Explorer 500 Series Commercial LeafletDocument6 pagesBourbon Explorer 500 Series Commercial LeafletDaniel ZhangNo ratings yet
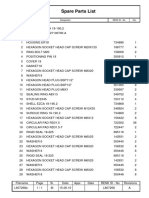
- Pms 500 - International Mechanics KitDocument0 pagesPms 500 - International Mechanics KitArsul RNo ratings yet
- Momentum - Action High Intensity 2022Document24 pagesMomentum - Action High Intensity 2022GabrielNo ratings yet
- THE 3RD INDONESIA EBTKE CONEX 2014 (4-6 June'14) PDFDocument10 pagesTHE 3RD INDONESIA EBTKE CONEX 2014 (4-6 June'14) PDFArik AprilliyantoNo ratings yet
- 01 IKSP and Environmental MovementsDocument12 pages01 IKSP and Environmental MovementsGlister Diadem DolleraNo ratings yet
- CV TemplateDocument1 pageCV TemplateHimanshu RaghuwanshiNo ratings yet
- Biodiversity ReportDocument52 pagesBiodiversity ReportAdrian HudsonNo ratings yet
- Excel Subhadip NandyDocument9 pagesExcel Subhadip NandyNihilisticDelusionNo ratings yet
- Joint Inspection Report FormatDocument2 pagesJoint Inspection Report FormatRAMAKRISHNAN RNo ratings yet
- Aciclovir 400mg and 800mg TabletsDocument2 pagesAciclovir 400mg and 800mg TabletsKalyan NandanNo ratings yet
- Newyearbook PDFDocument165 pagesNewyearbook PDFAlberto CenniniNo ratings yet
- Merciales v. CA (2002)Document5 pagesMerciales v. CA (2002)Jude FanilaNo ratings yet
- Smart Test Series: Q.1 Circle The Correct Answers. (6x1 6)Document1 pageSmart Test Series: Q.1 Circle The Correct Answers. (6x1 6)Eeman AkbarNo ratings yet
- The Enemy Within - v18Document8 pagesThe Enemy Within - v18Matt WillisNo ratings yet
- Government SyllabusDocument3 pagesGovernment Syllabusapi-100383549No ratings yet
- Industrial Development Economic Growth in Andhra PradeshDocument9 pagesIndustrial Development Economic Growth in Andhra PradeshMurali Krishna ReddyNo ratings yet
- Ernst Bloch Principle of Hope PDFDocument2 pagesErnst Bloch Principle of Hope PDFAdamNo ratings yet
- Antenna Mini ProjectDocument65 pagesAntenna Mini ProjectHassan MehsenNo ratings yet
- Review of The Householder's Guide To Community Defence Against Bureaucratic Aggression (1973)Document2 pagesReview of The Householder's Guide To Community Defence Against Bureaucratic Aggression (1973)Regular BookshelfNo ratings yet
- CAT LOGO ALPINESTARS OFF-ROAD 2021Document73 pagesCAT LOGO ALPINESTARS OFF-ROAD 2021Carla ArcosNo ratings yet
- Councillor Danny Thorpe: Leader, Royal Borough of GreenwichDocument2 pagesCouncillor Danny Thorpe: Leader, Royal Borough of GreenwichDr-Syed Ali TarekNo ratings yet
- ALVAREZ, John Edriane A - Experiment No. 1Document7 pagesALVAREZ, John Edriane A - Experiment No. 1John Edriane AlvarezNo ratings yet
- Imran Index 1Document11 pagesImran Index 1api-387022302No ratings yet
- L807268EDocument1 pageL807268EsjsshipNo ratings yet
- Percakapan BHS Inggris Penerimaan PasienDocument5 pagesPercakapan BHS Inggris Penerimaan PasienYulia WyazztNo ratings yet