You might also like
- Psychological Testing-II Report Submitted by Fatima Syed Fa17-Bpy-016Document53 pagesPsychological Testing-II Report Submitted by Fatima Syed Fa17-Bpy-016Fatima SyedNo ratings yet
- Critical Thinking: A Literature Review: Research ReportDocument50 pagesCritical Thinking: A Literature Review: Research ReportLenna NicaNo ratings yet
- Usefullness of TestingDocument64 pagesUsefullness of TestingThảo TrầnNo ratings yet
- Psychological Assessment Test BankDocument25 pagesPsychological Assessment Test BankCharmaine CuarteNo ratings yet
- Industrial Psych RGO Enhanced For 2017Document178 pagesIndustrial Psych RGO Enhanced For 2017Anonymous okusLz100% (1)
- Choosing a Research Method, Scientific Inquiry:: Complete Process with Qualitative & Quantitative Design ExamplesFrom EverandChoosing a Research Method, Scientific Inquiry:: Complete Process with Qualitative & Quantitative Design ExamplesNo ratings yet
- Critical ThinkingDocument6 pagesCritical ThinkingMohammad Ashraful AminNo ratings yet
- Brainard Occupational Preference Inventory (BOPI)Document15 pagesBrainard Occupational Preference Inventory (BOPI)Zeke CoronacionNo ratings yet
- Concept Analysis in Nursing MORSEDocument27 pagesConcept Analysis in Nursing MORSEMARILYN PINEDANo ratings yet
- Critical ThinkingDocument6 pagesCritical ThinkingAzizul Hakim HashimNo ratings yet
- Critical Thinking, The Nursing Process, and Clinical Judgment PDFDocument22 pagesCritical Thinking, The Nursing Process, and Clinical Judgment PDFChristian Jake Paomey100% (5)
- Evidence-Based Nursing (Qualitative Research)Document6 pagesEvidence-Based Nursing (Qualitative Research)focus16hoursgmailcom100% (1)
- Critical Thinking and CreativityDocument25 pagesCritical Thinking and CreativityLilianaNo ratings yet
- A Layperson’S Guide to Understanding Research and Data AnalysisFrom EverandA Layperson’S Guide to Understanding Research and Data AnalysisNo ratings yet
- Methods in Behavioural Research Canadian 2nd Edition Cozby Test Bank 1Document11 pagesMethods in Behavioural Research Canadian 2nd Edition Cozby Test Bank 1claire100% (46)
- Clinical ReasoningDocument23 pagesClinical Reasoningathe_triiaNo ratings yet
- An Assessment of Psychosocial Challenges of The Elderly in Ibagwa-Aka Community, Igbo-Eze South Local Government Area of Enugu State, NigeriaDocument71 pagesAn Assessment of Psychosocial Challenges of The Elderly in Ibagwa-Aka Community, Igbo-Eze South Local Government Area of Enugu State, NigeriaSarah AdogaNo ratings yet
- Psychology Research Methods: A Writing Intensive ApproachFrom EverandPsychology Research Methods: A Writing Intensive ApproachNo ratings yet
- CompetentClinicalJdgmjnt CCTDI 94 JNEdDocument14 pagesCompetentClinicalJdgmjnt CCTDI 94 JNEd9 PsychologyNo ratings yet
- Disposition To CT 1995 JGEDocument18 pagesDisposition To CT 1995 JGEJee SyahfitriNo ratings yet
- Review of Related Literature and Studies: Student's Name: Juan Dela Cruz Section & Group: BSN4A - Group 1Document17 pagesReview of Related Literature and Studies: Student's Name: Juan Dela Cruz Section & Group: BSN4A - Group 1sshhaplNo ratings yet
- Disposition Toward Critical ThinkingDocument17 pagesDisposition Toward Critical ThinkingVicente De la OssaNo ratings yet
- Critical Thinking Versus Clinical Reasoning Versus Clinical JudgmentDocument3 pagesCritical Thinking Versus Clinical Reasoning Versus Clinical JudgmentWinda ArfinaNo ratings yet
- Critical Thinking Definitions PDFDocument2 pagesCritical Thinking Definitions PDFAlpha Niño S SanguenzaNo ratings yet
- F300 Extended Project Summative TaskDocument9 pagesF300 Extended Project Summative TaskRennyNo ratings yet
- CRITical Thinking 1Document5 pagesCRITical Thinking 1Emeraldha TheodorusNo ratings yet
- Dimensions of Critical ThinkingDocument6 pagesDimensions of Critical ThinkingMiguel SeminarioNo ratings yet
- The Scientifically Minded Psychologist Science As A Core CompetencyDocument11 pagesThe Scientifically Minded Psychologist Science As A Core CompetencyPaula Manalo-SuliguinNo ratings yet
- The Purpose of Literature Review in Qualitative ResearchDocument5 pagesThe Purpose of Literature Review in Qualitative ResearchafmzveaqnkpypmNo ratings yet
- Critical Thinking: A Literature Review: Research ReportDocument50 pagesCritical Thinking: A Literature Review: Research ReportJay AbainzaNo ratings yet
- Critical Thinking Review FinalDocument50 pagesCritical Thinking Review FinalJay AbainzaNo ratings yet
- Sesión 3. Jankowski2000 Article FusingHorizonsExploringQualitaDocument10 pagesSesión 3. Jankowski2000 Article FusingHorizonsExploringQualitaMariana Andrea Pinillos GuzmanNo ratings yet
- Relationships Between Critical and Creative ThinkiDocument17 pagesRelationships Between Critical and Creative ThinkiDian LaraNo ratings yet
- The Development of A Test On Critical Thinking: August 2008Document9 pagesThe Development of A Test On Critical Thinking: August 2008mvnivanNo ratings yet
- Relationships Between Critical and Creative ThinkiDocument17 pagesRelationships Between Critical and Creative ThinkiAchmad Zultan MansurNo ratings yet
- How Should Critical Thinking Be Conceptualized?Document10 pagesHow Should Critical Thinking Be Conceptualized?Azher BeboNo ratings yet
- Fountain 2016Document23 pagesFountain 2016Alfred RodNo ratings yet
- Final Project Topic Selection Workand Literature ReviewDocument5 pagesFinal Project Topic Selection Workand Literature ReviewMichael Guido PierangelinoNo ratings yet
- Students Knowledge SlidesDocument20 pagesStudents Knowledge SlidesDilshad ShahNo ratings yet
- Critical Thinking Extended DefinitionDocument9 pagesCritical Thinking Extended DefinitionGhina SaleemNo ratings yet
- King Kitchener 2004Document15 pagesKing Kitchener 2004Endris AbbayNo ratings yet
- Thinking Skills and CreativityDocument9 pagesThinking Skills and CreativityArifNo ratings yet
- Notes in Research CompleteDocument19 pagesNotes in Research CompletejennmeriscoNo ratings yet
- The Internal Audit As Tool To Enhance The Quality of Qualitative ResearchDocument15 pagesThe Internal Audit As Tool To Enhance The Quality of Qualitative ResearchEvantheNo ratings yet
- Devon 2007 A Psychometric Toolbox For Testing ValidityDocument10 pagesDevon 2007 A Psychometric Toolbox For Testing ValidityNatalia Esquivel GarzonNo ratings yet
- Understanding The Assessment of Clinical Reasoning: Omar S. LaynesaDocument20 pagesUnderstanding The Assessment of Clinical Reasoning: Omar S. Laynesaomar laynesaNo ratings yet
- Resarch IdeaDocument23 pagesResarch IdeaNashwa KamalNo ratings yet
- Ryan Coughlan Qualitative Research CritiqueDocument7 pagesRyan Coughlan Qualitative Research CritiqueAndreea IonitaNo ratings yet
- Gandire Critică Pentru Cadrele DidactieDocument9 pagesGandire Critică Pentru Cadrele DidactieAlina SitarNo ratings yet
- Developing Students' Critical Thinking Skills by Task-Based Learning in Chemistry Experiment TeachingDocument6 pagesDeveloping Students' Critical Thinking Skills by Task-Based Learning in Chemistry Experiment TeachingIffatul MunaNo ratings yet
- 201 FullDocument5 pages201 FullAmongusNo ratings yet
- Kielhofners Research in Occupational Therapy Methods of Inquiry For Enhancing Practice 2Nd Edition Full ChapterDocument42 pagesKielhofners Research in Occupational Therapy Methods of Inquiry For Enhancing Practice 2Nd Edition Full Chapterwallace.poulsen272100% (25)
- Berfikir KritisDocument28 pagesBerfikir KritistyasNo ratings yet
- Chapter1 Introd QRDocument22 pagesChapter1 Introd QRrajanityagi23No ratings yet
- BPC The Centrality of ResearchDocument8 pagesBPC The Centrality of ResearchApóstolo Jurandir Ribeiro ArautoNo ratings yet
- Pensamiento CriticoDocument111 pagesPensamiento CriticoEdwin VasquezNo ratings yet
- Kielhofners Research in Occupational Therapy Methods of Inquiry For Enhancing Practice 2nd Edition Ebook PDF VersionDocument62 pagesKielhofners Research in Occupational Therapy Methods of Inquiry For Enhancing Practice 2nd Edition Ebook PDF Versionbruce.glinski869100% (42)
- Malterud-2001-Qualitative Research - Standards, Challenges, and Guidelines PDFDocument6 pagesMalterud-2001-Qualitative Research - Standards, Challenges, and Guidelines PDFJeronimo SantosNo ratings yet
- Quantitative Research 2 ModuleDocument106 pagesQuantitative Research 2 Modulecathy domingoNo ratings yet
- Why Is Literature Review Important in ScienceDocument5 pagesWhy Is Literature Review Important in Sciencetkpmzasif100% (1)
- Dev 334Document4 pagesDev 334Gkri Proskyneoo-bsdNo ratings yet
- Rothstien, A. - A Perspective On Doing A ConsultationDocument11 pagesRothstien, A. - A Perspective On Doing A ConsultationFelipe LeguerNo ratings yet
- Understanding and Evaluating QualitativeDocument16 pagesUnderstanding and Evaluating QualitativeSubashni VeeramuthuNo ratings yet
- Literature Review Evidence LevelDocument4 pagesLiterature Review Evidence Levelcdkxbcrif100% (1)
- Module 2 Research LanguageDocument10 pagesModule 2 Research Languageruby gullemNo ratings yet
- 1 s2.0 S1871187123001359 MainDocument13 pages1 s2.0 S1871187123001359 MaindinaNo ratings yet
- Fairness in Educational and Psychological Testing: Examining Theoretical, Research, Practice, and Policy Implications of the 2014 StandardsFrom EverandFairness in Educational and Psychological Testing: Examining Theoretical, Research, Practice, and Policy Implications of the 2014 StandardsNo ratings yet
- 213 680 1 PBDocument5 pages213 680 1 PBiman si tampan kerenNo ratings yet
- Redhana 2021 J. Phys. Conf. Ser. 1806 012187Document6 pagesRedhana 2021 J. Phys. Conf. Ser. 1806 012187iman si tampan kerenNo ratings yet
- Fostering Critical Thinking Through Socrates' Questioning in Iranian Language InstitutesDocument6 pagesFostering Critical Thinking Through Socrates' Questioning in Iranian Language Institutesiman si tampan kerenNo ratings yet
- Mohsen Zare & Reza Biria: Original ArticleDocument8 pagesMohsen Zare & Reza Biria: Original Articleiman si tampan kerenNo ratings yet
- Download pdf Research In Education 10Th Edition John W Best ebook full chapterDocument53 pagesDownload pdf Research In Education 10Th Edition John W Best ebook full chapterryan.klein198No ratings yet
- Diff. Types of Research InstrumentDocument3 pagesDiff. Types of Research Instrumentanon_814871911No ratings yet
- RiyadiDocument15 pagesRiyadiPadlah Riyadi. SE., Ak., CA., MM.No ratings yet
- 217163-Article Text-534568-1-10-20211109Document18 pages217163-Article Text-534568-1-10-20211109Krishna KumarNo ratings yet
- Research On The Customer Involvement in E-Commerce 2.0Document7 pagesResearch On The Customer Involvement in E-Commerce 2.0ivan platiniNo ratings yet
- RPR Mba 2nd YearDocument32 pagesRPR Mba 2nd YearSimar KaurNo ratings yet
- Work Environ, MotivasiDocument12 pagesWork Environ, MotivasiW Deamaga AlberoraNo ratings yet
- Shensa 2018Document13 pagesShensa 2018Dini Pratiwi NasruddinNo ratings yet
- CH 1Document18 pagesCH 1bharat sachdevaNo ratings yet
- Research in Daily Life 2Document175 pagesResearch in Daily Life 2Bryan SambranoNo ratings yet
- Data ValidationDocument5 pagesData ValidationAli KhanNo ratings yet
- Validation of The General Health Questionnaire GHQDocument6 pagesValidation of The General Health Questionnaire GHQAbby p.No ratings yet
- Measurement of AttitudeDocument23 pagesMeasurement of AttitudeA K SubramaniNo ratings yet
- Competitive Intelligence and Marketing Effectiveness in Corporate Organizations in NigeriaDocument13 pagesCompetitive Intelligence and Marketing Effectiveness in Corporate Organizations in Nigeriazemen tadesseNo ratings yet
- 4 Main Characteristics of A Good TestDocument8 pages4 Main Characteristics of A Good TestSaNnilyn MiNonNo ratings yet
- Using Mind Maps and Diagrams To Teach Vocabulary For First Year Mainstream Students at Division IDocument114 pagesUsing Mind Maps and Diagrams To Teach Vocabulary For First Year Mainstream Students at Division INương Đoàn100% (18)
- Esp Students'Responses To Task-Based Language Teaching (TBLT) ImplementationDocument417 pagesEsp Students'Responses To Task-Based Language Teaching (TBLT) ImplementationBadPlayNo ratings yet
- Industrial Management & Data Systems: Article InformationDocument42 pagesIndustrial Management & Data Systems: Article Informationhassan_zazaus3965No ratings yet
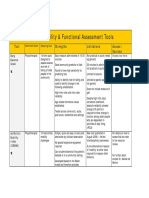
- 2013 Table 1 Mobility and Functional Assessment Tools PDFDocument4 pages2013 Table 1 Mobility and Functional Assessment Tools PDFesbat07No ratings yet
- Business Strategy - MSMEs' Performance Relationship: Innovation and Accounting Information System As MediatorsDocument21 pagesBusiness Strategy - MSMEs' Performance Relationship: Innovation and Accounting Information System As MediatorsLejandra MNo ratings yet
- Factors That Influence The Decision When BuyingDocument39 pagesFactors That Influence The Decision When Buyingprince様.No ratings yet
- 283 752 1 PB1 PDFDocument39 pages283 752 1 PB1 PDFIvan MiStNo ratings yet
- Political Impact of Media ExposureDocument21 pagesPolitical Impact of Media Exposureelena24ungureanuNo ratings yet