You might also like
- Case Study (Preeclampsia)Document6 pagesCase Study (Preeclampsia)Jobelle AcenaNo ratings yet
- Case Study of Chronic Hypertension with Superimposed PreeclampsiaDocument13 pagesCase Study of Chronic Hypertension with Superimposed PreeclampsiaIvan Laurentine AceretNo ratings yet
- Pa Tho ReviseDocument10 pagesPa Tho ReviseCharl SembranoNo ratings yet
- Obstetric EmergenciesDocument44 pagesObstetric EmergenciesVijith.V.kumarNo ratings yet
- Amniotic Fluid EmbolismDocument51 pagesAmniotic Fluid EmbolismDenyse Mayer Atutubo100% (2)
- Preeclampsia and EclampsiaDocument23 pagesPreeclampsia and Eclampsiaapi-3705046100% (6)
- Endothelin's role in renal diseases and hypertensionDocument7 pagesEndothelin's role in renal diseases and hypertensionElena EllaNo ratings yet
- Pediatric Heart FailureDocument16 pagesPediatric Heart FailureCharlie LeeNo ratings yet
- Seeking Closure For Pda - Neonatal Care UpdateDocument46 pagesSeeking Closure For Pda - Neonatal Care Updateapi-602288180No ratings yet
- A 2 Year Old Boy With Hypoxemia, Pulmonary HyperteDocument4 pagesA 2 Year Old Boy With Hypoxemia, Pulmonary HyperteagamerocallejasNo ratings yet
- Lecture 01 Hemorrh-Diat KaplanDocument53 pagesLecture 01 Hemorrh-Diat KaplanАбдул Насер МохаммадізмаелNo ratings yet
- Shock: Syahbuddin HarahapDocument41 pagesShock: Syahbuddin Harahapprima suci angrainiNo ratings yet
- Palpitation Kel 14Document28 pagesPalpitation Kel 14Mufthiar MuhtarNo ratings yet
- Shock and Its Management: Presented byDocument72 pagesShock and Its Management: Presented bysheme171150% (2)
- Right-Sided Heart Failure: College of NursingDocument30 pagesRight-Sided Heart Failure: College of NursingMatelyn OargaNo ratings yet
- Report EndocarditisDocument38 pagesReport EndocarditisCamille MarasiganNo ratings yet
- MaeDocument9 pagesMaeCharmaigne Mae Padilla Sotelo100% (1)
- MK Final PaperworkDocument15 pagesMK Final Paperworkapi-727427971No ratings yet
- Congenital Heart DefectDocument12 pagesCongenital Heart Defectsangkularosmina837No ratings yet
- Case Study Trauma and Emergency Nursing NRSG 467-SHOCKDocument21 pagesCase Study Trauma and Emergency Nursing NRSG 467-SHOCKErickNabiswa100% (2)
- Cardiovascular System Diseases Part 2Document9 pagesCardiovascular System Diseases Part 2Prince Rener Velasco PeraNo ratings yet
- Cardiovascular System Diseases Part 2Document9 pagesCardiovascular System Diseases Part 2Prince Rener Velasco PeraNo ratings yet
- Short Case Hydrocephalus: by Febrianto Haba Bunga, S.Ked Consultant DR .Donny Argie, SP - BSDocument29 pagesShort Case Hydrocephalus: by Febrianto Haba Bunga, S.Ked Consultant DR .Donny Argie, SP - BSErkoNo ratings yet
- Mrcs NotesDocument24 pagesMrcs Notesnob2011nob67% (3)
- Assessment and Diagnostic TestsDocument55 pagesAssessment and Diagnostic TestsEmma IntiaNo ratings yet
- Shock BBDocument31 pagesShock BBVirang ParikhNo ratings yet
- PPHNDocument25 pagesPPHNFunda TüzünNo ratings yet
- Hypovolemic Shock Nursing Care Management and Study GuideDocument1 pageHypovolemic Shock Nursing Care Management and Study GuideRoselyn VelascoNo ratings yet
- Protocol - Lymphangioleiomyomatosis (HCC 02242023)Document15 pagesProtocol - Lymphangioleiomyomatosis (HCC 02242023)Brian OlajeNo ratings yet
- Neonatal Anesthesia Preoperative Evaluation and PreparationDocument168 pagesNeonatal Anesthesia Preoperative Evaluation and PreparationAlyssa GarciaNo ratings yet
- Nurul Ilmi Hajar (PO.71.3.201.14.1.130) Nurul Khabliana (PO.71.3.201.14.1.131)Document27 pagesNurul Ilmi Hajar (PO.71.3.201.14.1.130) Nurul Khabliana (PO.71.3.201.14.1.131)Nurulilmi hajarNo ratings yet
- Alterations in Tissue PerfusionDocument16 pagesAlterations in Tissue PerfusionPatricia CaladoNo ratings yet
- Measure Blood Pressure CorrectlyDocument56 pagesMeasure Blood Pressure CorrectlyAnna HaritonencoNo ratings yet
- Pre Eclampsia and EclampsiaDocument40 pagesPre Eclampsia and EclampsiaDakshayini MbNo ratings yet
- Pregnancy Induced HypertensionDocument38 pagesPregnancy Induced HypertensionЕрнур КасымбаевNo ratings yet
- Adult Health Exam Hematology and LeukemiaDocument11 pagesAdult Health Exam Hematology and Leukemiabrandie webbNo ratings yet
- Truncus ArteriosusDocument20 pagesTruncus ArteriosusjustinahorroNo ratings yet
- Cardiovascular Diseases FinalDocument119 pagesCardiovascular Diseases FinalabhieghailNo ratings yet
- Hematopoiesis Is The Complex Process of The Formation and Maturation of Blood CellsDocument35 pagesHematopoiesis Is The Complex Process of The Formation and Maturation of Blood CellsYary MayorNo ratings yet
- Understanding the Pathophysiology of Coronary Artery DiseaseDocument14 pagesUnderstanding the Pathophysiology of Coronary Artery DiseasejohnhenryvNo ratings yet
- Shock in Obgyn: Michelle Schroeder, MD Busitema University Faculty of Health SciencesDocument30 pagesShock in Obgyn: Michelle Schroeder, MD Busitema University Faculty of Health SciencesMwanja MosesNo ratings yet
- SHOCKDocument60 pagesSHOCKJoseph John K PothanikatNo ratings yet
- High Risk Pregnancy 1Document205 pagesHigh Risk Pregnancy 1Vanessa Angel Bugarin100% (3)
- 4 - ShockDocument14 pages4 - ShockRENEROSE TORRESNo ratings yet
- Guideline on managing and investigating hypertension in childrenDocument13 pagesGuideline on managing and investigating hypertension in childrenJohn Romero CevallosNo ratings yet
- Melbourne 14 May 2005: Case 1: Rotator Cuff InjuryDocument9 pagesMelbourne 14 May 2005: Case 1: Rotator Cuff InjuryZweNo ratings yet
- Final Exam NotesDocument24 pagesFinal Exam NotesNicholeGarcesCisnerosNo ratings yet
- ShockDocument25 pagesShockAvneet Maan100% (1)
- Portal Hypertension, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPortal Hypertension, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Case study of Anterior Wall MIDocument32 pagesCase study of Anterior Wall MIسوما الشمريNo ratings yet
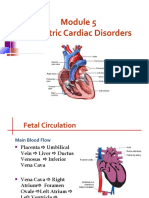
- Pediatric Cardiac Disorders: Fetal Circulation and Congestive Heart FailureDocument62 pagesPediatric Cardiac Disorders: Fetal Circulation and Congestive Heart FailureMarie Queenly Pagaran100% (1)
- Cell Injury - Part 1Document58 pagesCell Injury - Part 1Mirleyka GonzálezNo ratings yet
- Eclampsia Pre EclampsiaDocument3 pagesEclampsia Pre EclampsiaOona Nicole Diorico100% (2)
- Pelvis Perineum Cases 04Document5 pagesPelvis Perineum Cases 04Uloko ChristopherNo ratings yet
- Case StudyDocument10 pagesCase StudyEMANUEL SAGUIPEDNo ratings yet
- SHOCKDocument28 pagesSHOCKMohammad Azzlan Abd RahmanNo ratings yet
- Acute GlumerulonephritisDocument77 pagesAcute GlumerulonephritisNicoleNo ratings yet
- H0meroom Pta OfficersDocument2 pagesH0meroom Pta OfficersCasas, Jo-an Pauline A.No ratings yet
- The Talkative Turtle Who Couldn't FlyDocument2 pagesThe Talkative Turtle Who Couldn't FlyCasas, Jo-an Pauline A.No ratings yet
- Manipulative Information and Media: Reporters: Jo-An Pauline Casas Jhon Lee CasicasDocument33 pagesManipulative Information and Media: Reporters: Jo-An Pauline Casas Jhon Lee CasicasCasas, Jo-an Pauline A.100% (1)
- Mini Case Study 1Document5 pagesMini Case Study 1Casas, Jo-an Pauline A.No ratings yet
- Grade IVDocument1 pageGrade IVCasas, Jo-an Pauline A.No ratings yet
- Casas, Jo-An Pauline A. - (LAB) Basic Concepts in NutritionDocument2 pagesCasas, Jo-An Pauline A. - (LAB) Basic Concepts in NutritionCasas, Jo-an Pauline A.No ratings yet
- Republic of The PhilippinesdarizaDocument1 pageRepublic of The PhilippinesdarizaCasas, Jo-an Pauline A.No ratings yet
- Words of GratitudeDocument1 pageWords of GratitudeCasas, Jo-an Pauline A.100% (1)
- King Midas' Golden TouchDocument7 pagesKing Midas' Golden TouchCasas, Jo-an Pauline A.No ratings yet
- The Talkative Turtle Who Couldn't FlyDocument2 pagesThe Talkative Turtle Who Couldn't FlyCasas, Jo-an Pauline A.No ratings yet
- Chef's or Cook's Knife - : Name: Casas, Jose Joel Jr. A. Course & YearDocument10 pagesChef's or Cook's Knife - : Name: Casas, Jose Joel Jr. A. Course & YearCasas, Jo-an Pauline A.No ratings yet
- King Midas' Golden TouchDocument7 pagesKing Midas' Golden TouchCasas, Jo-an Pauline A.No ratings yet
- Psychological Assessment: (Insert and PDF Palihug Te Hehe)Document6 pagesPsychological Assessment: (Insert and PDF Palihug Te Hehe)Casas, Jo-an Pauline A.100% (1)
- Movie ReviewDocument4 pagesMovie ReviewCasas, Jo-an Pauline A.No ratings yet
- MechanicalDocument4 pagesMechanicalCasas, Jo-an Pauline A.No ratings yet
- Philosophical Assumptions: Positivistic ParadigmDocument4 pagesPhilosophical Assumptions: Positivistic ParadigmCasas, Jo-an Pauline A.No ratings yet
- Performance Task 1Document4 pagesPerformance Task 1Casas, Jo-an Pauline A.No ratings yet
- Dariza ADocument2 pagesDariza ACasas, Jo-an Pauline A.No ratings yet
- Health Inequity and Inequality in The Philippines During The Covid-19 PandemicDocument2 pagesHealth Inequity and Inequality in The Philippines During The Covid-19 PandemicCasas, Jo-an Pauline A.No ratings yet
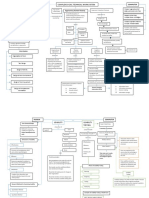
- Concept MapDocument2 pagesConcept MapCasas, Jo-an Pauline A.No ratings yet
- Psychological-Assessment ScriptDocument9 pagesPsychological-Assessment ScriptCasas, Jo-an Pauline A.No ratings yet
- Performance Task 1Document4 pagesPerformance Task 1Casas, Jo-an Pauline A.No ratings yet
- STARLIGHT Business Model Canvas: Customer Segments Value Propositions Key Activities Key Partners Customer RelationshipsDocument1 pageSTARLIGHT Business Model Canvas: Customer Segments Value Propositions Key Activities Key Partners Customer RelationshipsCasas, Jo-an Pauline A.No ratings yet
- Understanding Ergonomic Principles in Complex Work SystemsDocument2 pagesUnderstanding Ergonomic Principles in Complex Work SystemsCasas, Jo-an Pauline A.No ratings yet
- Nursing Informatics NotesDocument52 pagesNursing Informatics NotesCasas, Jo-an Pauline A.No ratings yet
- Understanding Ergonomic Principles in Complex Work SystemsDocument2 pagesUnderstanding Ergonomic Principles in Complex Work SystemsCasas, Jo-an Pauline A.No ratings yet
- Starlight: Be The Starlight of FashionDocument10 pagesStarlight: Be The Starlight of FashionCasas, Jo-an Pauline A.No ratings yet
- Performance-Task 2Document10 pagesPerformance-Task 2Casas, Jo-an Pauline A.No ratings yet
- Critical Care Applications: ExampleDocument19 pagesCritical Care Applications: ExampleCasas, Jo-an Pauline A.No ratings yet
- H. PyloriDocument5 pagesH. PyloriWaleed El SaidNo ratings yet
- Physical and Healthy ImpairmentsDocument27 pagesPhysical and Healthy ImpairmentsMwanalushi KanjalaNo ratings yet
- Projective Tests GuideDocument35 pagesProjective Tests GuideHera FakherNo ratings yet
- H2O2 Nebulization Therapy 3.19.2020Document5 pagesH2O2 Nebulization Therapy 3.19.2020Theodosius Arcadius100% (1)
- Hes 005 Session 12 SasDocument12 pagesHes 005 Session 12 SasBread PartyNo ratings yet
- Restored Republic Via A GCR 9-12-2023Document15 pagesRestored Republic Via A GCR 9-12-2023XRPLion1 On TwitterNo ratings yet
- IUD Office Order No. 001-2021Document5 pagesIUD Office Order No. 001-2021Ashish RajNo ratings yet
- Fetal DistressDocument33 pagesFetal DistressYara H QaisiNo ratings yet
- KSADS DSM 5 Supp4 DevelopmentalDisruptiveDO FinalDocument28 pagesKSADS DSM 5 Supp4 DevelopmentalDisruptiveDO FinalKsenia Startseva-LoraNo ratings yet
- Hemolytic Disease of Newborn (HDN): Causes, Symptoms & TreatmentDocument26 pagesHemolytic Disease of Newborn (HDN): Causes, Symptoms & Treatmentmaher Haji officialNo ratings yet
- Rehab Centre For DisabledDocument48 pagesRehab Centre For DisabledHanan Mohammed KhalidNo ratings yet
- Group 5 - Immunotherapy and VaccineDocument78 pagesGroup 5 - Immunotherapy and VaccineThe KingNo ratings yet
- Training PrinciplesDocument22 pagesTraining PrinciplesgundadanNo ratings yet
- Cosmetic Animal TestingDocument17 pagesCosmetic Animal Testingapi-449963555No ratings yet
- Effect of Bhramari Pranayama and Yoga NidraDocument3 pagesEffect of Bhramari Pranayama and Yoga Nidrajuan_emilioNo ratings yet
- Lung CancerDocument12 pagesLung CancerАнастасия ОстапенкоNo ratings yet
- Case Mannequin Body InteractDocument5 pagesCase Mannequin Body InteractAVITA TRISTA NINGRUM100% (1)
- New Normal Safety Guidelines HotelsDocument12 pagesNew Normal Safety Guidelines HotelsMark Kenneth B. CamamaNo ratings yet
- Welding, Cutting & Grinding-1Document131 pagesWelding, Cutting & Grinding-1like saddamNo ratings yet
- Microbiome risk profiles as biomarkers for inflammatory and metabolic disordersDocument15 pagesMicrobiome risk profiles as biomarkers for inflammatory and metabolic disordersMartinaNo ratings yet
- Opiod CrisisDocument3 pagesOpiod Crisisapi-583806911No ratings yet
- Occupational English Test Oet Reading Test 04 Part A Text BookletDocument4 pagesOccupational English Test Oet Reading Test 04 Part A Text BookletAndreaNo ratings yet
- Official Reprint From Uptodate ©2018 Uptodate, Inc. And/Or Its Affiliates. All Rights ReservedDocument13 pagesOfficial Reprint From Uptodate ©2018 Uptodate, Inc. And/Or Its Affiliates. All Rights ReservedAnh NguyenNo ratings yet
- Biology Notes IGCSE Excretion NoteDocument9 pagesBiology Notes IGCSE Excretion NoteCorina HuNo ratings yet
- Aspirin Paracetamol CaffeineDocument3 pagesAspirin Paracetamol CaffeineMariusNeicuNo ratings yet
- Arvind Eye CareDocument9 pagesArvind Eye CareNaman SharmaNo ratings yet
- Eyes and Ears AssessmentDocument2 pagesEyes and Ears AssessmentAngela EstolasNo ratings yet
- Contemporary Approach To Dental CariesDocument465 pagesContemporary Approach To Dental CariesGeorgiana IlincaNo ratings yet
- Readers Digest International - March 2017Document130 pagesReaders Digest International - March 2017Alfredo Rafael AcostaNo ratings yet
- Final Exam MCQsDocument23 pagesFinal Exam MCQsTrang Nguyen50% (2)