You might also like
- Healthcare Information Technology for Cardiovascular Medicine: Telemedicine & Digital HealthFrom EverandHealthcare Information Technology for Cardiovascular Medicine: Telemedicine & Digital HealthAmi B. BhattNo ratings yet
- Management Information System in HealthcareDocument3 pagesManagement Information System in HealthcareThirdy AquinoNo ratings yet
- NCM110 LP2Document10 pagesNCM110 LP2Daisy RoseteNo ratings yet
- Jennifer Bautista A.K.A. Minah Bautista A.K.A. Mildred Narvarte A.K.A. Malinda Sirue A.K.ADocument24 pagesJennifer Bautista A.K.A. Minah Bautista A.K.A. Mildred Narvarte A.K.A. Malinda Sirue A.K.AmalindaNo ratings yet
- Hospital InformationDocument26 pagesHospital InformationTushar GhuleNo ratings yet
- 1NURSING INFORMATICS - IT Application in Nursing PracticeDocument13 pages1NURSING INFORMATICS - IT Application in Nursing PracticeANHIBEY, JEZREEL ACE S.0% (1)
- Nursing InformaticsDocument5 pagesNursing InformaticsYmer Gelladuga0% (2)
- Managementinformationsysteminhealthcare 120114161332 Phpapp01Document20 pagesManagementinformationsysteminhealthcare 120114161332 Phpapp01MARY VIENNE PASCUALNo ratings yet
- Information Technology System Applicable in Nursing PracticeDocument4 pagesInformation Technology System Applicable in Nursing PracticeEstelle RhineNo ratings yet
- Information System: Administrative and Clinical Health Information SystemsDocument3 pagesInformation System: Administrative and Clinical Health Information SystemsWinell GutierrezNo ratings yet
- Information Technology System Applicable in Nursing PracticeDocument92 pagesInformation Technology System Applicable in Nursing PracticeATEHAN BORDS100% (1)
- Critical Care ApplicationsDocument35 pagesCritical Care ApplicationsrdelmoroNo ratings yet
- Information Technology System Applicable To Nursing PracticeDocument54 pagesInformation Technology System Applicable To Nursing PracticeKristle Ann VillarealNo ratings yet
- Introduction to Health Information Systems (HISDocument36 pagesIntroduction to Health Information Systems (HISmariel santosNo ratings yet
- Unit 8 PDFDocument8 pagesUnit 8 PDFratherazhar31No ratings yet
- Critical Care ApplicationDocument39 pagesCritical Care ApplicationjimwelluismNo ratings yet
- Hospital Information Management SystemDocument13 pagesHospital Information Management SystemSarita yadavNo ratings yet
- Nursing InformaticsDocument5 pagesNursing InformaticsQuaynie SulongNo ratings yet
- What Is Nursing InformaticsDocument3 pagesWhat Is Nursing InformaticsRose JoyNo ratings yet
- Nursing Informatics - Computers and NursingDocument5 pagesNursing Informatics - Computers and NursingAllia Rae Diaz GuiaoNo ratings yet
- Ambulatory Care System and Telehealth Nursing InfoDocument59 pagesAmbulatory Care System and Telehealth Nursing InfoCharmm LinnamNo ratings yet
- Role of Information Technology in MedicineDocument7 pagesRole of Information Technology in MedicineFahadghaznavi100% (1)
- Application of Heath InformaticsDocument12 pagesApplication of Heath InformaticsWrenzie NanagadNo ratings yet
- Introduction HISDocument11 pagesIntroduction HISAmr Ibrahim Mohammed ShetaNo ratings yet
- An Intelligent Architecture For Multi-Agent Based M-Health Care SystemDocument5 pagesAn Intelligent Architecture For Multi-Agent Based M-Health Care SystemDhayanithi JaganathanNo ratings yet
- Information Technology System Applicable in Nursing Practice Notes 1Document7 pagesInformation Technology System Applicable in Nursing Practice Notes 1Stephanie Lee100% (2)
- Infochap10 12Document18 pagesInfochap10 12Nareeza AbdullaNo ratings yet
- EHR, telemedicine, e-health: The role of medical informaticsDocument9 pagesEHR, telemedicine, e-health: The role of medical informaticsFaith SarmientoNo ratings yet
- Week 3Document37 pagesWeek 3Rasmina Jhoy Roque Quintana33% (3)
- Medical Information Systems in Healthcare OrganisationsDocument38 pagesMedical Information Systems in Healthcare OrganisationsFatimaNo ratings yet
- G 3Document17 pagesG 3Bernadette Dangate MalbasNo ratings yet
- Unit 1 Overview of Health Information SystemDocument4 pagesUnit 1 Overview of Health Information SystemMr. PotatoheadNo ratings yet
- Nursing Informatics Key ConceptsDocument9 pagesNursing Informatics Key Conceptsluchi darkNo ratings yet
- Mental Health Care Patient Management System Case StudyDocument8 pagesMental Health Care Patient Management System Case StudyIqra farooqNo ratings yet
- Nursing Tics Lecture NotesDocument4 pagesNursing Tics Lecture NotesMichael Gustilo100% (1)
- 1 - Class 5 - Healthcare Information Systems - DR - HananDocument35 pages1 - Class 5 - Healthcare Information Systems - DR - HananHanan AlkorashyNo ratings yet
- CHN1 Lec Session #22 SASDocument9 pagesCHN1 Lec Session #22 SASspooderm4nNo ratings yet
- Nursing Informatics: Bachelor of Science in NursingDocument7 pagesNursing Informatics: Bachelor of Science in NursingANGELICA MACASONo ratings yet
- Critical Care ApplicationsDocument3 pagesCritical Care ApplicationsJustine Bianca NayreNo ratings yet
- Computers and NursingDocument5 pagesComputers and NursingZharah Ruz100% (1)
- Hospital Information System: Prof - DR/ Safaa Mohamed Abd Elrahman DR/ Mona Thabet AbdelbasetDocument16 pagesHospital Information System: Prof - DR/ Safaa Mohamed Abd Elrahman DR/ Mona Thabet AbdelbasetYoussef MohsenNo ratings yet
- Nursing Informatics: Unit 1 Information ScienceDocument3 pagesNursing Informatics: Unit 1 Information ScienceGabbi KimNo ratings yet
- Mentcare Case Study 05042021 072850pmDocument3 pagesMentcare Case Study 05042021 072850pmatifNo ratings yet
- PERIA TRISHIA MAE 2nd Activity NI Lab MidtermDocument3 pagesPERIA TRISHIA MAE 2nd Activity NI Lab MidtermTrishia Mae PeriaNo ratings yet
- Activity 1. (Nursing Informatics)Document2 pagesActivity 1. (Nursing Informatics)emielyn marcosNo ratings yet
- Information-Technology-applicable-in-nursing-practice_G1_BSN2A_MidtermDocument20 pagesInformation-Technology-applicable-in-nursing-practice_G1_BSN2A_Midterm배아No ratings yet
- Informatics in Nursing Practice Education Research and AdministrationDocument76 pagesInformatics in Nursing Practice Education Research and AdministrationHarold DiasanaNo ratings yet
- Contemporary Presentation CHDocument44 pagesContemporary Presentation CHapi-546505804No ratings yet
- INFORMATICSDocument18 pagesINFORMATICSKyle De Sagun Oteda100% (1)
- Critical Care ApplicationDocument49 pagesCritical Care ApplicationGracy CasañaNo ratings yet
- BioethicsDocument7 pagesBioethicsClarissa Anne TabaosaresNo ratings yet
- His Topic 4 Reporting 1Document37 pagesHis Topic 4 Reporting 1Jean Marie FelipeNo ratings yet
- Community Health Application: Home Health Information SystemsDocument4 pagesCommunity Health Application: Home Health Information SystemsKyla CarbonelNo ratings yet
- UNIT 5 Practice Aplication - Doc - NiDocument11 pagesUNIT 5 Practice Aplication - Doc - NiClaire VicenteNo ratings yet
- Electronic Medical Record (EMR) and Electronic Health Record (EHR)Document3 pagesElectronic Medical Record (EMR) and Electronic Health Record (EHR)kathlyn MayoNo ratings yet
- HMIS - Hospital management information system in nursingDocument34 pagesHMIS - Hospital management information system in nursingEsha KuttiNo ratings yet
- Lesson 1.1: Historical Perspectives of Nursing InformaticsDocument33 pagesLesson 1.1: Historical Perspectives of Nursing InformaticsJustine Jean GuillermoNo ratings yet
- His For Mls - Medical Laboratory Science It (Prelim Reviewer)Document3 pagesHis For Mls - Medical Laboratory Science It (Prelim Reviewer)Kyle M. BayangosNo ratings yet
- Improving Patient Care Through Electronic Health RecordsDocument4 pagesImproving Patient Care Through Electronic Health RecordsTrishia Mae PeriaNo ratings yet
- N Ntroduction: H I S (HIS)Document27 pagesN Ntroduction: H I S (HIS)Mule AnduNo ratings yet
- H0meroom Pta OfficersDocument2 pagesH0meroom Pta OfficersCasas, Jo-an Pauline A.No ratings yet
- Mini Case Study 1Document14 pagesMini Case Study 1Casas, Jo-an Pauline A.No ratings yet
- Manipulative Information and Media: Reporters: Jo-An Pauline Casas Jhon Lee CasicasDocument33 pagesManipulative Information and Media: Reporters: Jo-An Pauline Casas Jhon Lee CasicasCasas, Jo-an Pauline A.100% (1)
- Mini Case Study 1Document5 pagesMini Case Study 1Casas, Jo-an Pauline A.No ratings yet
- The Talkative Turtle Who Couldn't FlyDocument2 pagesThe Talkative Turtle Who Couldn't FlyCasas, Jo-an Pauline A.No ratings yet
- King Midas' Golden TouchDocument7 pagesKing Midas' Golden TouchCasas, Jo-an Pauline A.No ratings yet
- Grade IVDocument1 pageGrade IVCasas, Jo-an Pauline A.No ratings yet
- King Midas' Golden TouchDocument7 pagesKing Midas' Golden TouchCasas, Jo-an Pauline A.No ratings yet
- Casas, Jo-An Pauline A. - (LAB) Basic Concepts in NutritionDocument2 pagesCasas, Jo-An Pauline A. - (LAB) Basic Concepts in NutritionCasas, Jo-an Pauline A.No ratings yet
- Psychological Assessment: (Insert and PDF Palihug Te Hehe)Document6 pagesPsychological Assessment: (Insert and PDF Palihug Te Hehe)Casas, Jo-an Pauline A.100% (1)
- The Talkative Turtle Who Couldn't FlyDocument2 pagesThe Talkative Turtle Who Couldn't FlyCasas, Jo-an Pauline A.No ratings yet
- Words of GratitudeDocument1 pageWords of GratitudeCasas, Jo-an Pauline A.100% (1)
- Republic of The PhilippinesdarizaDocument1 pageRepublic of The PhilippinesdarizaCasas, Jo-an Pauline A.No ratings yet
- Movie ReviewDocument4 pagesMovie ReviewCasas, Jo-an Pauline A.No ratings yet
- Dariza ADocument2 pagesDariza ACasas, Jo-an Pauline A.No ratings yet
- Chef's or Cook's Knife - : Name: Casas, Jose Joel Jr. A. Course & YearDocument10 pagesChef's or Cook's Knife - : Name: Casas, Jose Joel Jr. A. Course & YearCasas, Jo-an Pauline A.No ratings yet
- MechanicalDocument4 pagesMechanicalCasas, Jo-an Pauline A.No ratings yet
- Performance Task 1Document4 pagesPerformance Task 1Casas, Jo-an Pauline A.No ratings yet
- Psychological-Assessment ScriptDocument9 pagesPsychological-Assessment ScriptCasas, Jo-an Pauline A.No ratings yet
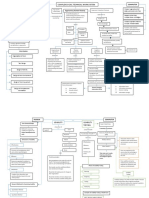
- Concept MapDocument2 pagesConcept MapCasas, Jo-an Pauline A.No ratings yet
- Health Inequity and Inequality in The Philippines During The Covid-19 PandemicDocument2 pagesHealth Inequity and Inequality in The Philippines During The Covid-19 PandemicCasas, Jo-an Pauline A.No ratings yet
- Philosophical Assumptions: Positivistic ParadigmDocument4 pagesPhilosophical Assumptions: Positivistic ParadigmCasas, Jo-an Pauline A.No ratings yet
- Understanding Ergonomic Principles in Complex Work SystemsDocument2 pagesUnderstanding Ergonomic Principles in Complex Work SystemsCasas, Jo-an Pauline A.No ratings yet
- Starlight: Be The Starlight of FashionDocument10 pagesStarlight: Be The Starlight of FashionCasas, Jo-an Pauline A.No ratings yet
- Performance Task 1Document4 pagesPerformance Task 1Casas, Jo-an Pauline A.No ratings yet
- STARLIGHT Business Model Canvas: Customer Segments Value Propositions Key Activities Key Partners Customer RelationshipsDocument1 pageSTARLIGHT Business Model Canvas: Customer Segments Value Propositions Key Activities Key Partners Customer RelationshipsCasas, Jo-an Pauline A.No ratings yet
- Understanding Ergonomic Principles in Complex Work SystemsDocument2 pagesUnderstanding Ergonomic Principles in Complex Work SystemsCasas, Jo-an Pauline A.No ratings yet
- Performance-Task 2Document10 pagesPerformance-Task 2Casas, Jo-an Pauline A.No ratings yet
- Nursing Informatics NotesDocument52 pagesNursing Informatics NotesCasas, Jo-an Pauline A.No ratings yet
- Cortical Deafness: Oleh: Dr. Laila Fajri Pembimbing: Dr. Novina Rahmawati, M.Si, Med, SP - THT-KL, FICSDocument18 pagesCortical Deafness: Oleh: Dr. Laila Fajri Pembimbing: Dr. Novina Rahmawati, M.Si, Med, SP - THT-KL, FICSzikral hadiNo ratings yet
- THE GALLUP ORGANIZATION For The American Board of Internal MedicineDocument38 pagesTHE GALLUP ORGANIZATION For The American Board of Internal MedicineabimorgNo ratings yet
- Grade 10 Health Career PlanningDocument12 pagesGrade 10 Health Career PlanningJenz Rey Justo50% (2)
- Medical: MycologyDocument395 pagesMedical: MycologyEl Fatih MunexNo ratings yet
- GAMBARAN TINGKAT KEBUTUHAN PERAWATAN ORTODONTIDocument6 pagesGAMBARAN TINGKAT KEBUTUHAN PERAWATAN ORTODONTIFerdyelvNo ratings yet
- Final Ger Syllbus Jan16 Bridging 2016 After DR ModificationDocument2 pagesFinal Ger Syllbus Jan16 Bridging 2016 After DR ModificationHaneenNo ratings yet
- Effectiveness of Using Contraceptives of The TeenagersDocument9 pagesEffectiveness of Using Contraceptives of The TeenagersQUEDDENG, CLYDE WALTER D.No ratings yet
- Fact Sheet For Health Care Providers - Arcoxia Tablet Salut Selaput 90 MG - Etorikoksib - DKL1906609417B1 - 2021Document22 pagesFact Sheet For Health Care Providers - Arcoxia Tablet Salut Selaput 90 MG - Etorikoksib - DKL1906609417B1 - 2021Edward LaurentNo ratings yet
- Lewis: Medical-Surgical Nursing, 8 Edition: Chapter 21: Nursing Assessment: Visual and Auditory Systems Test BankDocument8 pagesLewis: Medical-Surgical Nursing, 8 Edition: Chapter 21: Nursing Assessment: Visual and Auditory Systems Test BankMonicaNo ratings yet
- Quality Control Circle - Desk File and WorkDocument26 pagesQuality Control Circle - Desk File and WorkZuhairi MohamedNo ratings yet
- Medical Device Classification GuideDocument30 pagesMedical Device Classification GuideAriska Oktavera 26No ratings yet
- TMU Programs 2020-21Document12 pagesTMU Programs 2020-21Mohammad SharikNo ratings yet
- Gestational Diabetes Mellitus: Case PresentationDocument46 pagesGestational Diabetes Mellitus: Case PresentationATEHAN BORDSNo ratings yet
- Ayurvedic Approach Towards Cerebral PalsyDocument6 pagesAyurvedic Approach Towards Cerebral PalsyHarry BellemareNo ratings yet
- Human Resources For HealthDocument17 pagesHuman Resources For Healthalina petreNo ratings yet
- Philippine Barangay Health PlansDocument23 pagesPhilippine Barangay Health PlansNapieh Bulalaque PolisticoNo ratings yet
- Estudio CesarDocument90 pagesEstudio CesarVeronica DubayNo ratings yet
- Activity Intolerance R/T Generalized WeaknessDocument3 pagesActivity Intolerance R/T Generalized Weaknesschanmin limNo ratings yet
- PRC Case Form Cmo 14Document5 pagesPRC Case Form Cmo 14iamELHIZANo ratings yet
- CV of Indonesian Nursing Professor and ResearcherDocument5 pagesCV of Indonesian Nursing Professor and Researcherwedus2No ratings yet
- 7.1 Pasmeth, Pamet, Laws, Specimen Collection And: Handling, Clinical MicrosDocument24 pages7.1 Pasmeth, Pamet, Laws, Specimen Collection And: Handling, Clinical MicrosMarcoNo ratings yet
- Oxytocin Is Not Associated With Postpartum Hemorrhage in Labor Augmentation in A Retrospective Cohort Study in The United StatesDocument9 pagesOxytocin Is Not Associated With Postpartum Hemorrhage in Labor Augmentation in A Retrospective Cohort Study in The United Statesstat madeeasyNo ratings yet
- KUHS Changes BDS RegulationsDocument1 pageKUHS Changes BDS RegulationsJoseph John K PothanikatNo ratings yet
- Rheumatic Fever and Rheumatic Heart Disease 2017 and IeDocument59 pagesRheumatic Fever and Rheumatic Heart Disease 2017 and IeLipi GautamNo ratings yet
- Pearl Zanker School: Shangrila Mia-Ramzan, Principal Recep Iscan, Assistant PrincipalDocument4 pagesPearl Zanker School: Shangrila Mia-Ramzan, Principal Recep Iscan, Assistant PrincipalsirishaNo ratings yet
- JHS Students' Knowledge of Healthy Food and Their Actual Eating HabitsDocument78 pagesJHS Students' Knowledge of Healthy Food and Their Actual Eating HabitsDessirea FurigayNo ratings yet
- Interview Questions For NursesDocument2 pagesInterview Questions For Nursesshalf0xNo ratings yet
- Australian Dental Journal - 2014 - Ahmed - Rubber Dam Application in Endodontic Practice An Update On Critical EducationalDocument7 pagesAustralian Dental Journal - 2014 - Ahmed - Rubber Dam Application in Endodontic Practice An Update On Critical Educationalneissen MasmoudiNo ratings yet
- Global Assessment (PG-SGA) : Scored Patient-Generated SubjectiveDocument1 pageGlobal Assessment (PG-SGA) : Scored Patient-Generated SubjectiveSafira Ridha UlyaNo ratings yet
- Conscious Sedation: Hayel Gharaibeh, MD. Anesthesia ConsultantDocument84 pagesConscious Sedation: Hayel Gharaibeh, MD. Anesthesia ConsultantKhaled GharaibehNo ratings yet
- The Wires of War: Technology and the Global Struggle for PowerFrom EverandThe Wires of War: Technology and the Global Struggle for PowerRating: 4 out of 5 stars4/5 (34)
- The Digital Marketing Handbook: A Step-By-Step Guide to Creating Websites That SellFrom EverandThe Digital Marketing Handbook: A Step-By-Step Guide to Creating Websites That SellRating: 5 out of 5 stars5/5 (6)
- Defensive Cyber Mastery: Expert Strategies for Unbeatable Personal and Business SecurityFrom EverandDefensive Cyber Mastery: Expert Strategies for Unbeatable Personal and Business SecurityRating: 5 out of 5 stars5/5 (1)
- How to Do Nothing: Resisting the Attention EconomyFrom EverandHow to Do Nothing: Resisting the Attention EconomyRating: 4 out of 5 stars4/5 (421)
- So You Want to Start a Podcast: Finding Your Voice, Telling Your Story, and Building a Community that Will ListenFrom EverandSo You Want to Start a Podcast: Finding Your Voice, Telling Your Story, and Building a Community that Will ListenRating: 4.5 out of 5 stars4.5/5 (35)
- Ultimate Guide to YouTube for BusinessFrom EverandUltimate Guide to YouTube for BusinessRating: 5 out of 5 stars5/5 (1)
- Python for Beginners: The 1 Day Crash Course For Python Programming In The Real WorldFrom EverandPython for Beginners: The 1 Day Crash Course For Python Programming In The Real WorldNo ratings yet
- The Internet Con: How to Seize the Means of ComputationFrom EverandThe Internet Con: How to Seize the Means of ComputationRating: 5 out of 5 stars5/5 (6)
- Social Media Marketing 2024, 2025: Build Your Business, Skyrocket in Passive Income, Stop Working a 9-5 Lifestyle, True Online Working from HomeFrom EverandSocial Media Marketing 2024, 2025: Build Your Business, Skyrocket in Passive Income, Stop Working a 9-5 Lifestyle, True Online Working from HomeNo ratings yet
- How to Be Fine: What We Learned by Living by the Rules of 50 Self-Help BooksFrom EverandHow to Be Fine: What We Learned by Living by the Rules of 50 Self-Help BooksRating: 4.5 out of 5 stars4.5/5 (48)
- Content Rules: How to Create Killer Blogs, Podcasts, Videos, Ebooks, Webinars (and More) That Engage Customers and Ignite Your BusinessFrom EverandContent Rules: How to Create Killer Blogs, Podcasts, Videos, Ebooks, Webinars (and More) That Engage Customers and Ignite Your BusinessRating: 4.5 out of 5 stars4.5/5 (42)
- Ultimate Guide to LinkedIn for Business: Access more than 500 million people in 10 minutesFrom EverandUltimate Guide to LinkedIn for Business: Access more than 500 million people in 10 minutesRating: 5 out of 5 stars5/5 (5)
- TikTok Algorithms 2024 $15,000/Month Guide To Escape Your Job And Build an Successful Social Media Marketing Business From Home Using Your Personal Account, Branding, SEO, InfluencerFrom EverandTikTok Algorithms 2024 $15,000/Month Guide To Escape Your Job And Build an Successful Social Media Marketing Business From Home Using Your Personal Account, Branding, SEO, InfluencerRating: 4 out of 5 stars4/5 (4)
- The $1,000,000 Web Designer Guide: A Practical Guide for Wealth and Freedom as an Online FreelancerFrom EverandThe $1,000,000 Web Designer Guide: A Practical Guide for Wealth and Freedom as an Online FreelancerRating: 4.5 out of 5 stars4.5/5 (22)
- Nine Algorithms That Changed the Future: The Ingenious Ideas That Drive Today's ComputersFrom EverandNine Algorithms That Changed the Future: The Ingenious Ideas That Drive Today's ComputersRating: 5 out of 5 stars5/5 (7)
- SEO 2021: Learn search engine optimization with smart internet marketing strategiesFrom EverandSEO 2021: Learn search engine optimization with smart internet marketing strategiesRating: 5 out of 5 stars5/5 (6)
- HTML5 and CSS3 Masterclass: In-depth Web Design Training with Geolocation, the HTML5 Canvas, 2D and 3D CSS Transformations, Flexbox, CSS Grid, and More (English Edition)From EverandHTML5 and CSS3 Masterclass: In-depth Web Design Training with Geolocation, the HTML5 Canvas, 2D and 3D CSS Transformations, Flexbox, CSS Grid, and More (English Edition)No ratings yet
- More Porn - Faster!: 50 Tips & Tools for Faster and More Efficient Porn BrowsingFrom EverandMore Porn - Faster!: 50 Tips & Tools for Faster and More Efficient Porn BrowsingRating: 3.5 out of 5 stars3.5/5 (23)
- The Designer’s Guide to Figma: Master Prototyping, Collaboration, Handoff, and WorkflowFrom EverandThe Designer’s Guide to Figma: Master Prototyping, Collaboration, Handoff, and WorkflowNo ratings yet