You might also like
- (For More Information Please Visit:) : Table 5. Oral Care Plans (Adapted From CCNS (1), BCCA (3,4) and Su Et Al (14) )Document2 pages(For More Information Please Visit:) : Table 5. Oral Care Plans (Adapted From CCNS (1), BCCA (3,4) and Su Et Al (14) )Kateryna BondarenkoNo ratings yet
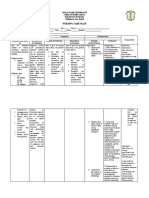
- Nursing Diagnosis: Assessment Nursing Diagnosis Planning Nursing Interventions Rationale Evaluation SubjectiveDocument2 pagesNursing Diagnosis: Assessment Nursing Diagnosis Planning Nursing Interventions Rationale Evaluation SubjectiveLen meloNo ratings yet
- Performing Oral Care (Providing Oral Care For Dependent Client)Document6 pagesPerforming Oral Care (Providing Oral Care For Dependent Client)Gladys SariowanNo ratings yet
- Nursing Care Plans DiagnosisDocument17 pagesNursing Care Plans DiagnosisSeham AliNo ratings yet
- Nursing Care Plan For Patient C (Problem 2)Document3 pagesNursing Care Plan For Patient C (Problem 2)Jesabel DocdocanNo ratings yet
- Course Task 7 Dengue Fever, Filariasis, Malaria and EncephalitisDocument4 pagesCourse Task 7 Dengue Fever, Filariasis, Malaria and EncephalitisBunnie AlphaNo ratings yet
- Mouth CareDocument11 pagesMouth CareKedamObulesu Kedam50% (2)
- Care PlansDocument14 pagesCare Plansapoc lordNo ratings yet
- Basic Nursing SkillsDocument43 pagesBasic Nursing SkillsBernardo NañoNo ratings yet
- Counseling For Gargle, Magic Mouth Wash & Mucositis in Cancer PTDocument3 pagesCounseling For Gargle, Magic Mouth Wash & Mucositis in Cancer PTAthirah BidinNo ratings yet
- Assignment 2 First AidDocument2 pagesAssignment 2 First AidEmma PataNo ratings yet
- NCP EbuenDocument3 pagesNCP EbuenNocReyesNo ratings yet
- Assessment Diagnosis Intervention Rationale EvaluationDocument11 pagesAssessment Diagnosis Intervention Rationale EvaluationBenjie DimayacyacNo ratings yet
- Drugs ReviewedDocument7 pagesDrugs ReviewedJamil LorcaNo ratings yet
- Radiotheraphy and Chemotherapy - HuppDocument7 pagesRadiotheraphy and Chemotherapy - HuppJamm ReaNo ratings yet
- Exercise Treatment: Medication Hygiene Outpatient DietDocument5 pagesExercise Treatment: Medication Hygiene Outpatient DietCarla Tongson MaravillaNo ratings yet
- Mouth, Hands, Neck, Extremities.: Disease Assesment Findings Medications Nsg. Considerations ImpetigoDocument8 pagesMouth, Hands, Neck, Extremities.: Disease Assesment Findings Medications Nsg. Considerations ImpetigoYna RamiroNo ratings yet
- Instillations and IrrigationsDocument40 pagesInstillations and IrrigationsAnn Merlin JobinNo ratings yet
- OralDocument3 pagesOralShaii Whomewhat GuyguyonNo ratings yet
- Skill 3 Skills Rel TO Personal Hyg ENE: Ated IDocument26 pagesSkill 3 Skills Rel TO Personal Hyg ENE: Ated IerkfcNo ratings yet
- Hair Care and Foot CareDocument6 pagesHair Care and Foot CareKelsey MacaraigNo ratings yet
- Wound ManagementDocument25 pagesWound ManagementAlwin RaisNo ratings yet
- Oral Hygiene Word FileDocument13 pagesOral Hygiene Word FileManoj DongarwarNo ratings yet
- O o o o o o O: DescriptionDocument34 pagesO o o o o o O: DescriptionDarren BalbasNo ratings yet
- Saliva and Its Prosthodontic ImplicationsDocument3 pagesSaliva and Its Prosthodontic Implicationsdrvivek reddyNo ratings yet
- Nursing Care Plan For "Fecal Diversions"Document14 pagesNursing Care Plan For "Fecal Diversions"jhonroks78% (9)
- Pediatric Dentistry: Nathalya Bmay A. Subido, DMDDocument118 pagesPediatric Dentistry: Nathalya Bmay A. Subido, DMDMaryjoy PaladanNo ratings yet
- NappyRash WebDocument4 pagesNappyRash WebGhea Tahara SugiantoNo ratings yet
- Perineal-Genital Area: Purposes: To Remove Normal Perineal Secretions and Odor To Prevent Infection To Promote ComfortDocument58 pagesPerineal-Genital Area: Purposes: To Remove Normal Perineal Secretions and Odor To Prevent Infection To Promote ComfortRuffa Mae CalimagNo ratings yet
- Mouthwashs: Asmaa Bassam Abu Amer Besan Montaser JoudaDocument32 pagesMouthwashs: Asmaa Bassam Abu Amer Besan Montaser JoudaAssssssNo ratings yet
- Male Genital EczemeDocument4 pagesMale Genital EczemewandalexNo ratings yet
- Impaired Skin IntegrityDocument3 pagesImpaired Skin IntegrityNeriz Pineda0% (1)
- Personal Hygiene: MaterialsDocument6 pagesPersonal Hygiene: Materialssannu ahmedNo ratings yet
- Impaired Oral Mucous Membranes - NCPDocument2 pagesImpaired Oral Mucous Membranes - NCPXtianna Jade Doquila100% (1)
- NGT and OstomyDocument2 pagesNGT and OstomyDarianne B. BasaNo ratings yet
- Skin Picking 2022Document3 pagesSkin Picking 2022Оксана ДиткунNo ratings yet
- NCP Impaired Oral Mucous MembraneDocument2 pagesNCP Impaired Oral Mucous Membraneklemtot83% (6)
- Things Inside The First Aid Kit: Name: Emplamado, RG B. Course and Section: BS Accountancy - 1BDocument4 pagesThings Inside The First Aid Kit: Name: Emplamado, RG B. Course and Section: BS Accountancy - 1BArgNo ratings yet
- Post Insertion Problems For Complete Denture and Their ManagementDocument8 pagesPost Insertion Problems For Complete Denture and Their ManagementTaha AlaamryNo ratings yet
- Physical and Emotional Assessment: Checklist 87: Changing A Pouching System/Ostomy Appliance (Ileostomy or Colostomy)Document4 pagesPhysical and Emotional Assessment: Checklist 87: Changing A Pouching System/Ostomy Appliance (Ileostomy or Colostomy)Vincent Paul SantosNo ratings yet
- Coxsackievirus NCP W Patho 3Document3 pagesCoxsackievirus NCP W Patho 3Chryst Louise SaavedraNo ratings yet
- Adult Skin Care GuideDocument1 pageAdult Skin Care GuideNazir AhmadNo ratings yet
- Assignment 3: Lama Al-MashhrawiDocument12 pagesAssignment 3: Lama Al-MashhrawiLama NahedNo ratings yet
- Public Health - Prevention of Dental Caries - PPTX (Autosaved)Document138 pagesPublic Health - Prevention of Dental Caries - PPTX (Autosaved)Ahmed ElhossanyNo ratings yet
- Medication Exercise Treatment Hygiene Outpatient DietDocument6 pagesMedication Exercise Treatment Hygiene Outpatient DietCarla Tongson MaravillaNo ratings yet
- BathingDocument5 pagesBathingchristianjomariNo ratings yet
- UntitledDocument23 pagesUntitledNympha NiñoNo ratings yet
- What Is Dry MouthDocument1 pageWhat Is Dry Mouthالعمري العمريNo ratings yet
- Insect Bites StingsDocument1 pageInsect Bites StingsnamibadiNo ratings yet
- Scabies: How Is It Treated?: Patient Information LeafletDocument2 pagesScabies: How Is It Treated?: Patient Information LeafletRatu IntaniaNo ratings yet
- Mangment of Dentin Hypersensitivity.Document60 pagesMangment of Dentin Hypersensitivity.فاطمه شبانهNo ratings yet
- BAQUIRAN - HUME 124 Activity 2.2. Hazards at HomeDocument8 pagesBAQUIRAN - HUME 124 Activity 2.2. Hazards at HomeMa.angeli BaquiranNo ratings yet
- Suppositories: Presented byDocument21 pagesSuppositories: Presented byVanessa PatraoNo ratings yet
- Principles of Topical Dermatologic Therapy - Dermatologic Disorders - MSD Manual Professional EditionDocument6 pagesPrinciples of Topical Dermatologic Therapy - Dermatologic Disorders - MSD Manual Professional EditionFantahunNo ratings yet
- Safety Advice Sheet: Product Name: Interfine 979 Ref No: 0006Document1 pageSafety Advice Sheet: Product Name: Interfine 979 Ref No: 0006Mohamed NouzerNo ratings yet
- Rabbit Diseases: Disease Cause Symptoms Prevention TreatmentDocument3 pagesRabbit Diseases: Disease Cause Symptoms Prevention TreatmentAkinwumiNo ratings yet
- Wound Care ChecklistDocument5 pagesWound Care Checklistacademic purposes100% (1)
- Bromination of ArenesDocument13 pagesBromination of ArenesDaniel O ZamoraNo ratings yet
- CHN HandiesDocument10 pagesCHN HandiesFreeNursingNotesNo ratings yet
- Intra ReviewerDocument10 pagesIntra ReviewerL Rean Carmelle MAGALLONESNo ratings yet
- Care of The Older AdultsDocument17 pagesCare of The Older AdultsL Rean Carmelle MAGALLONESNo ratings yet
- Care of Older AdultsDocument13 pagesCare of Older AdultsL Rean Carmelle MAGALLONESNo ratings yet
- Maternal and Child Health Nursing Reviewer Compiled by NURSEHOOMANDocument122 pagesMaternal and Child Health Nursing Reviewer Compiled by NURSEHOOMANL Rean Carmelle MAGALLONESNo ratings yet
- Notes Maternal Health NursingdsdsDocument21 pagesNotes Maternal Health NursingdsdsL Rean Carmelle MAGALLONESNo ratings yet
- Care of The Older Adults: Skin Structure and Function of Desquamation HemoglobinDocument15 pagesCare of The Older Adults: Skin Structure and Function of Desquamation HemoglobinL Rean Carmelle MAGALLONESNo ratings yet
- Ante Sample Exam of All TiessDocument30 pagesAnte Sample Exam of All TiessL Rean Carmelle MAGALLONESNo ratings yet
- CHEMOTHERAPYDocument5 pagesCHEMOTHERAPYL Rean Carmelle MAGALLONESNo ratings yet
- Decoding CancerDocument6 pagesDecoding CancerL Rean Carmelle MAGALLONESNo ratings yet
- Gestational DiabetesDocument3 pagesGestational DiabetesL Rean Carmelle MAGALLONESNo ratings yet
- Effects of Cancer What Is CancerDocument4 pagesEffects of Cancer What Is CancerL Rean Carmelle MAGALLONESNo ratings yet
- RequirementDocument3 pagesRequirementL Rean Carmelle MAGALLONESNo ratings yet
- Intro To NCM 109Document3 pagesIntro To NCM 109L Rean Carmelle MAGALLONESNo ratings yet
- FdarDocument2 pagesFdarL Rean Carmelle MAGALLONESNo ratings yet
- Drug StudyDocument13 pagesDrug StudyL Rean Carmelle MAGALLONESNo ratings yet
- PreschoolDocument15 pagesPreschoolL Rean Carmelle MAGALLONESNo ratings yet
- InfantDocument25 pagesInfantL Rean Carmelle MAGALLONESNo ratings yet
- Stages of LaborDocument5 pagesStages of LaborL Rean Carmelle MAGALLONES100% (1)
- Nursing Care Plan: Holy Name University College of Health Sciences Department of Nursing Tagbilaran City, BoholDocument8 pagesNursing Care Plan: Holy Name University College of Health Sciences Department of Nursing Tagbilaran City, BoholL Rean Carmelle MAGALLONESNo ratings yet
- GeronDocument54 pagesGeronL Rean Carmelle MAGALLONESNo ratings yet
- Cesarean Section With Gestational Diabetes Mellitus: Case Study ofDocument19 pagesCesarean Section With Gestational Diabetes Mellitus: Case Study ofL Rean Carmelle MAGALLONESNo ratings yet
- Concept Mapping FormatDocument2 pagesConcept Mapping FormatL Rean Carmelle MAGALLONESNo ratings yet
- CancerDocument77 pagesCancerL Rean Carmelle MAGALLONESNo ratings yet
- Drug PoemDocument1 pageDrug PoemL Rean Carmelle MAGALLONESNo ratings yet
- GeronDocument54 pagesGeronL Rean Carmelle MAGALLONESNo ratings yet
- Get The Facts On Kindey DiseaseDocument1 pageGet The Facts On Kindey DiseaseL Rean Carmelle MAGALLONESNo ratings yet
- 2 - 5201750207762531221 EntDocument561 pages2 - 5201750207762531221 EntArun Raj100% (1)
- Patient ProfileDocument19 pagesPatient Profilebangus08No ratings yet
- Transverse MyelitisDocument7 pagesTransverse MyelitisAmr BashaNo ratings yet
- 4 - Nephritic SyndromeDocument2 pages4 - Nephritic SyndromeDrhisham AttiaNo ratings yet
- Abstract Leftsidest SetDocument1,047 pagesAbstract Leftsidest Setpokharelriwaj82No ratings yet
- CH 5 Providing Psychosocial CareDocument79 pagesCH 5 Providing Psychosocial CareKevin FacunNo ratings yet
- Microbiology Exam - Parasitology Flashcards - QuizletDocument17 pagesMicrobiology Exam - Parasitology Flashcards - QuizletIdrissa ContehNo ratings yet
- FULL-TEXT - NCLEX-RN Practice Quiz Test Bank 3 - NurseslabsDocument91 pagesFULL-TEXT - NCLEX-RN Practice Quiz Test Bank 3 - NurseslabsRonaldo Matos Perez100% (1)
- Cadila Pharmaceuticals Ltd. ProfileDocument3 pagesCadila Pharmaceuticals Ltd. Profilemail_garaiNo ratings yet
- 5 Patcharee Komvilaisak - Approaching To Pancytopenia 24112017Document43 pages5 Patcharee Komvilaisak - Approaching To Pancytopenia 24112017Satvik BansalNo ratings yet
- Focus On Adult Health Medical Surgical Nursing Pellico Edition Test BankDocument8 pagesFocus On Adult Health Medical Surgical Nursing Pellico Edition Test BankCarolineAndersoneacmg100% (33)
- Hospital Use CaseDocument3 pagesHospital Use Caseprashant gauravNo ratings yet
- Manejo de Conducta en Niños Ansiosos. (ING)Document6 pagesManejo de Conducta en Niños Ansiosos. (ING)Ale RamírezNo ratings yet
- Biotechnology & Drug Discovery.Document35 pagesBiotechnology & Drug Discovery.IrsaNo ratings yet
- 2021 Impact of Change Forecast Highlights: COVID-19 Recovery and Impact On Future UtilizationDocument17 pages2021 Impact of Change Forecast Highlights: COVID-19 Recovery and Impact On Future UtilizationwahidNo ratings yet
- Primitive ReflexesDocument10 pagesPrimitive Reflexesbun_yulianaNo ratings yet
- Plague ProjectDocument3 pagesPlague ProjectTushant SharmaNo ratings yet
- PulpotecDocument5 pagesPulpotecRuel MarmolejoNo ratings yet
- Head To Toe Assessment Checklist Older Adults-1Document1 pageHead To Toe Assessment Checklist Older Adults-1spatrick32100% (4)
- D5LRDocument2 pagesD5LRLouiseville Ann Arcilla PilNo ratings yet
- Nbde Study Resources PDFDocument3 pagesNbde Study Resources PDFMichael GarciaNo ratings yet
- High Dose Rate Interstitial Brachytherapy Using Two Weekly SessionsDocument1 pageHigh Dose Rate Interstitial Brachytherapy Using Two Weekly SessionsZuriNo ratings yet
- Ehmer Sling 24461 ArticleDocument4 pagesEhmer Sling 24461 Articlesuresh sellamuthuNo ratings yet
- Anatomy of Trigeminal Nerve & Trigeminal Neuralgia: Presented By: DR - Vansh Vardhan Madahar PG1 YearDocument47 pagesAnatomy of Trigeminal Nerve & Trigeminal Neuralgia: Presented By: DR - Vansh Vardhan Madahar PG1 YearVansh Vardhan MadaharNo ratings yet
- The Use of Vancomycin With Its Therapeutic and Adverse Effects: A ReviewDocument11 pagesThe Use of Vancomycin With Its Therapeutic and Adverse Effects: A Reviewdea yuniarNo ratings yet
- Neoblade Trial Slides For NCRI Bladder Cancer MeetingDocument10 pagesNeoblade Trial Slides For NCRI Bladder Cancer MeetingProf_Nick_JamesNo ratings yet
- Immunology: 'S CompanionsDocument74 pagesImmunology: 'S CompanionsRoahit RajanNo ratings yet
- Dialysis MachineDocument1 pageDialysis MachineMarifer NazNo ratings yet
- TetanusDocument22 pagesTetanusAlec AnonNo ratings yet
- Psychological Aspects of Living With HIV Disease: PracticeDocument4 pagesPsychological Aspects of Living With HIV Disease: PracticeAntro BerrinNo ratings yet