You might also like
- Aortic RegurgitationFrom EverandAortic RegurgitationJan VojacekNo ratings yet
- The Long-Term Outcomes of Physiologic Repair For Cctga (Congenitally Corrected Transposition of The Great Arteries)Document6 pagesThe Long-Term Outcomes of Physiologic Repair For Cctga (Congenitally Corrected Transposition of The Great Arteries)paul00040No ratings yet
- Modelo 2Document5 pagesModelo 2kodagaNo ratings yet
- 1 s2.0 S0929664608602041 MainDocument9 pages1 s2.0 S0929664608602041 MainEko SiswantoNo ratings yet
- Tetralogy of Fallot: What Operation, at Which Age: Marco Pozzi, Dipesh B. Trivedi, Denise Kitchiner, Robert A. ArnoldDocument6 pagesTetralogy of Fallot: What Operation, at Which Age: Marco Pozzi, Dipesh B. Trivedi, Denise Kitchiner, Robert A. ArnoldResiden KardiologiNo ratings yet
- Jurnal PVRDocument7 pagesJurnal PVRhans hulkNo ratings yet
- Dr. M Sahal - MitralDocument35 pagesDr. M Sahal - MitralHari Mas KuncoroNo ratings yet
- Long-Term Outcomes After Valve-Sparing Anatomical Aortic Root Reconstruction in Acute Dissection Involving The RootDocument10 pagesLong-Term Outcomes After Valve-Sparing Anatomical Aortic Root Reconstruction in Acute Dissection Involving The RootMaghfirah MahmuddinNo ratings yet
- Korean QX Total Pulm Veins 2010Document5 pagesKorean QX Total Pulm Veins 2010Dr. LicónNo ratings yet
- Midterm Outcomes of Minimally Invasive Mitral Valve Surgery in A Heterogeneous Valve Pathology Cohort: Respect or Resect?Document12 pagesMidterm Outcomes of Minimally Invasive Mitral Valve Surgery in A Heterogeneous Valve Pathology Cohort: Respect or Resect?mony saNo ratings yet
- Tga Lagi PDFDocument4 pagesTga Lagi PDFMYMANo ratings yet
- Outcome After Repair of Tetralogy of Fallot in The First Year of LifeDocument7 pagesOutcome After Repair of Tetralogy of Fallot in The First Year of LifeRadioputro WicaksonoNo ratings yet
- The Fate of The Distal Aorta After Repair of Acute Type A Aortic DissectionDocument10 pagesThe Fate of The Distal Aorta After Repair of Acute Type A Aortic Dissectionapi-160333876No ratings yet
- Late Surgical Treatment of Tetralogy of FallotDocument3 pagesLate Surgical Treatment of Tetralogy of FallotBryan NguyenNo ratings yet
- Minimally Invasive Mitral Valve Repair Through Right MinithoracotomyDocument7 pagesMinimally Invasive Mitral Valve Repair Through Right MinithoracotomyEnrico SquiccimarroNo ratings yet
- Mid Term Outcomes of Stentless Bio Bentall vs. David Reimplantation For Aortic Root ReplacementDocument8 pagesMid Term Outcomes of Stentless Bio Bentall vs. David Reimplantation For Aortic Root ReplacementStefanie MelisaNo ratings yet
- Pulmonary Atresia, Ventricular Septal Defect, and MAPCAs, Neonate Rehab On PADocument7 pagesPulmonary Atresia, Ventricular Septal Defect, and MAPCAs, Neonate Rehab On PAdinaNo ratings yet
- 2006 - Longterm Outcome After Surgery For Pulmonary Stenosis (A Longitudinal Study of 22-33 Years)Document7 pages2006 - Longterm Outcome After Surgery For Pulmonary Stenosis (A Longitudinal Study of 22-33 Years)Tammy Utami DewiNo ratings yet
- 3-Dimensional EchocardiographicDocument12 pages3-Dimensional EchocardiographicGeorgiana IonescuNo ratings yet
- Single-Stage Versus 2-Stage Repair of Coarctation of The Aorta With Ventricular Septal DefectDocument8 pagesSingle-Stage Versus 2-Stage Repair of Coarctation of The Aorta With Ventricular Septal DefectEko SiswantoNo ratings yet
- Clinical Effects of Pleurotomy On Patients Undergoing CABGDocument5 pagesClinical Effects of Pleurotomy On Patients Undergoing CABGBeshoy KhelaNo ratings yet
- Efficacy of TTK Chitra Mechanical Heart Valve Versus ST Jude Mechanical Heart Valve in Aortic Valve ReplacementDocument7 pagesEfficacy of TTK Chitra Mechanical Heart Valve Versus ST Jude Mechanical Heart Valve in Aortic Valve ReplacementIJAR JOURNALNo ratings yet
- Tamagond 2011Document5 pagesTamagond 2011Eko SiswantoNo ratings yet
- PIIS1078588419310755Document7 pagesPIIS1078588419310755zeeshan qurbanNo ratings yet
- Repair of Functional Tricuspid Regurgitation: Comparison Between Suture Annuloplasty and Rings AnnuloplastyDocument7 pagesRepair of Functional Tricuspid Regurgitation: Comparison Between Suture Annuloplasty and Rings AnnuloplastyKarthik RamanNo ratings yet
- Terapia de Resincronización en Pacientes Con Insuficiencia Cardiaca Experiencia Acumulada de 10 AñosDocument9 pagesTerapia de Resincronización en Pacientes Con Insuficiencia Cardiaca Experiencia Acumulada de 10 AñosKevin Alegre AguileraNo ratings yet
- Short - and Long-Term Outcomes at A Single InstitutionDocument7 pagesShort - and Long-Term Outcomes at A Single InstitutionJonathan Frimpong AnsahNo ratings yet
- Early and Intermediate-Term Results of The Extracardiac Conduit Total Cavopulmonary Connection For Functional Single-Ventricle HeartsDocument7 pagesEarly and Intermediate-Term Results of The Extracardiac Conduit Total Cavopulmonary Connection For Functional Single-Ventricle HeartstedejoNo ratings yet
- Yokawa (2019) - David Tidak SpesifikDocument6 pagesYokawa (2019) - David Tidak SpesifikStefanie MelisaNo ratings yet
- Percutaneous Aortic Valve Implantation: The Anesthesiologist PerspectiveDocument11 pagesPercutaneous Aortic Valve Implantation: The Anesthesiologist Perspectiveserena7205No ratings yet
- Disseccao Tipo b2Document6 pagesDisseccao Tipo b2coopervascba.diradmNo ratings yet
- Safety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaDocument9 pagesSafety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaSisca Dwi AgustinaNo ratings yet
- Effect of The Preservation of Annulo-Papillary Continuity On Left Ventricular Ejection Fraction After Mitral Valve ReplacementDocument4 pagesEffect of The Preservation of Annulo-Papillary Continuity On Left Ventricular Ejection Fraction After Mitral Valve ReplacementThanh BinhNo ratings yet
- Minimally Invasive Direct Cardiac MassagDocument13 pagesMinimally Invasive Direct Cardiac MassagTM AnNo ratings yet
- DeNino (2014)Document11 pagesDeNino (2014)Stefanie MelisaNo ratings yet
- Concomitant Bentall Operation Plus Aortic Arch Replacement SurgeryDocument7 pagesConcomitant Bentall Operation Plus Aortic Arch Replacement Surgeryprofarmah6150No ratings yet
- Kim2012Document5 pagesKim2012Stefanie MelisaNo ratings yet
- J Jacc 2012 10 036Document6 pagesJ Jacc 2012 10 036Ertan ALNo ratings yet
- Midterm Results of Mitral Valve Repair With Homemade Annuloplasty RingsDocument4 pagesMidterm Results of Mitral Valve Repair With Homemade Annuloplasty Ringsadel husseinNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyAldo AtjehNo ratings yet
- Open Fixation in Flail Chest: Review of 64 Patients: Riginal OntributionDocument6 pagesOpen Fixation in Flail Chest: Review of 64 Patients: Riginal OntributionDian PermatasariNo ratings yet
- IJGMP - RV Function Assessment Pre and Post PTMC in Patients With Severe - AutosavedDocument8 pagesIJGMP - RV Function Assessment Pre and Post PTMC in Patients With Severe - AutosavedImpact JournalsNo ratings yet
- Destete ECMO VADocument8 pagesDestete ECMO VADaniela PekeNo ratings yet
- PIIS091450871930084XDocument7 pagesPIIS091450871930084XdrewantaNo ratings yet
- Lemus Rangel 2010Document2 pagesLemus Rangel 2010audiNo ratings yet
- Pen Surgery For Thoracoabdominal Aortic Aneurysm-Is It Still A Horrible SurgeryDocument11 pagesPen Surgery For Thoracoabdominal Aortic Aneurysm-Is It Still A Horrible SurgeryJonathan Frimpong AnsahNo ratings yet
- International Journal of Surgery Case ReportsDocument6 pagesInternational Journal of Surgery Case ReportsUmar UsmanNo ratings yet
- Chandra 2013Document5 pagesChandra 2013Jose YoveraNo ratings yet
- Pi Is 0003497500014818Document7 pagesPi Is 0003497500014818GKNo ratings yet
- Openhrt 2021 001732Document9 pagesOpenhrt 2021 001732benypermadiNo ratings yet
- Elective Frozen Elephant Trunk Procedure Using The E-Vita Open Plus Prosthesis in 94 Patients: A Multicentre French RegistryDocument7 pagesElective Frozen Elephant Trunk Procedure Using The E-Vita Open Plus Prosthesis in 94 Patients: A Multicentre French RegistryrédaNo ratings yet
- Nejmoa 1805374Document10 pagesNejmoa 1805374Lia Diana RaileanuNo ratings yet
- Percutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaDocument6 pagesPercutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaCotaga IgorNo ratings yet
- New England Journal Medicine: The ofDocument9 pagesNew England Journal Medicine: The ofHesbon MomanyiNo ratings yet
- Dco 5 PDFDocument10 pagesDco 5 PDFGauda GranthanaNo ratings yet
- The Expanding Role of Peri Procedural EchocardiogrDocument2 pagesThe Expanding Role of Peri Procedural Echocardiogrxrszbkr77dNo ratings yet
- Study 3Document7 pagesStudy 3OstazNo ratings yet
- Narasimha Pai Issue 27 Mamatha RathnaDocument7 pagesNarasimha Pai Issue 27 Mamatha RathnadrpklalNo ratings yet
- Zheng 2016Document6 pagesZheng 2016Arindya RezekiNo ratings yet
- Impact of Optimal Medical Therapy On 10-Year Mortality After Coronary RevascularizationDocument12 pagesImpact of Optimal Medical Therapy On 10-Year Mortality After Coronary RevascularizationsarahNo ratings yet
- PIIS0894731723006235Document45 pagesPIIS0894731723006235paul00040No ratings yet
- Olfactory Outcomes After Middle Turbinate Resection in Endoscopic Transsphenoidal Surgery: A Prospective Randomized StudyDocument7 pagesOlfactory Outcomes After Middle Turbinate Resection in Endoscopic Transsphenoidal Surgery: A Prospective Randomized Studypaul00040No ratings yet
- Circinterventions 120 010154Document12 pagesCircinterventions 120 010154paul00040No ratings yet
- Physiologic Versus Anatomic Repair of Congenitally Corrected Transposition of The Great Arteries: Meta-Analysis of Individual Patient DataDocument7 pagesPhysiologic Versus Anatomic Repair of Congenitally Corrected Transposition of The Great Arteries: Meta-Analysis of Individual Patient Datapaul00040No ratings yet
- Critrios Phoenix para Sepsis NiñosDocument12 pagesCritrios Phoenix para Sepsis NiñosJorge MéndezNo ratings yet
- 1 s2.0 S0894731723006223 MainDocument52 pages1 s2.0 S0894731723006223 Mainpaul00040No ratings yet
- Management of Systemic Right Ventricular Failure in Patients With Congenitally Corrected Transposition of The Great ArteriesDocument10 pagesManagement of Systemic Right Ventricular Failure in Patients With Congenitally Corrected Transposition of The Great Arteriespaul00040No ratings yet
- Long-Term Outcome in Congenitally Corrected Transposition of The Great ArteriesDocument7 pagesLong-Term Outcome in Congenitally Corrected Transposition of The Great Arteriespaul00040No ratings yet
- E Book Nursing Congenital Heart DeseasesDocument302 pagesE Book Nursing Congenital Heart DeseasesKkvd pjt10No ratings yet
- Congenital Heart Disease and Adolescence (2016, Springer International Publishing)Document235 pagesCongenital Heart Disease and Adolescence (2016, Springer International Publishing)paul00040No ratings yet
- Circulationaha 117 032047 FullDocument28 pagesCirculationaha 117 032047 Fullpaul00040No ratings yet
- Deepika Thacker, Jack Rychik (Auth.), Robert. E Shaddy (Eds.) - Heart Failure in Congenital Heart Disease - From Fetus To Adult (2011, Springer-Verlag London)Document187 pagesDeepika Thacker, Jack Rychik (Auth.), Robert. E Shaddy (Eds.) - Heart Failure in Congenital Heart Disease - From Fetus To Adult (2011, Springer-Verlag London)paul00040No ratings yet
- (Pocket Notebook) Wooin Ahn, Jai Radhakrishnan - Pocket Nephrology-LWW Wolters Kluwer (2019)Document695 pages(Pocket Notebook) Wooin Ahn, Jai Radhakrishnan - Pocket Nephrology-LWW Wolters Kluwer (2019)paul0004090% (10)
- Nelson's Pediatric Antimicrobial PDFDocument331 pagesNelson's Pediatric Antimicrobial PDFMADHANKUMAR MANICKAVELNo ratings yet
- Mehta Et Al-2018-American Journal of TransplantationDocument8 pagesMehta Et Al-2018-American Journal of Transplantationpaul00040No ratings yet
- Orthotopic Mouse Liver Transplantation To Study Liver Biology and Allograft ToleranceDocument12 pagesOrthotopic Mouse Liver Transplantation To Study Liver Biology and Allograft Tolerancepaul00040No ratings yet
- Easily Missed Radiologic InjuriesDocument61 pagesEasily Missed Radiologic Injuriespaul00040No ratings yet
- Med by DesignDocument60 pagesMed by DesignkthaiNo ratings yet
- Brix Et Al-2017-Immunological ReviewsDocument31 pagesBrix Et Al-2017-Immunological Reviewspaul00040No ratings yet
- Lgner 2017Document8 pagesLgner 2017paul00040No ratings yet
- PMS PyDocument14 pagesPMS Pypaul00040No ratings yet
- PBLDocument8 pagesPBLpaul00040No ratings yet
- Modificari Electrocardiografice in Ischemia Miocardica Acuta - PPTX 2Document180 pagesModificari Electrocardiografice in Ischemia Miocardica Acuta - PPTX 2Andra RaducuNo ratings yet
- Accelerated Idioventricular RhythymDocument4 pagesAccelerated Idioventricular RhythymtjelongNo ratings yet
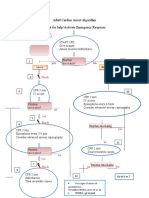
- Adult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseDocument1 pageAdult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseICU RSBMNo ratings yet
- Congenital Heart DefectsDocument19 pagesCongenital Heart DefectsNader Smadi67% (3)
- Acls Drug OverviewDocument2 pagesAcls Drug OverviewShannon Davis100% (1)
- Cardiac Surgery - Postoperative ArrhythmiasDocument9 pagesCardiac Surgery - Postoperative ArrhythmiaswanariaNo ratings yet
- ECG Interpretation Cheat SheetDocument14 pagesECG Interpretation Cheat Sheetrenet_alexandre75% (4)
- Heart Pathology MCQs (ANSWERS)Document9 pagesHeart Pathology MCQs (ANSWERS)juanNo ratings yet
- ECG InterpretationDocument52 pagesECG InterpretationMarcus, RN98% (44)
- Defibrillation and Electrical CardioversionDocument27 pagesDefibrillation and Electrical CardioversionYui Hirasawa100% (1)
- Model Test PapersDocument2 pagesModel Test Papersprofarmah6150No ratings yet
- Angina Pharmacology YeahDocument16 pagesAngina Pharmacology YeahMuhammad AfifuddinNo ratings yet
- Lutembacher's Syndrome - A Case ReportDocument2 pagesLutembacher's Syndrome - A Case ReportInternational Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- VT CriteriaDocument8 pagesVT CriterianitipatNo ratings yet
- Pediatric Cardiovascular System History & ExaminationDocument74 pagesPediatric Cardiovascular System History & Examinationعبدالله Abdullah INo ratings yet
- Incomplete Right Bundle Branch Block: Challenges in Electrocardiogram DiagnosisDocument7 pagesIncomplete Right Bundle Branch Block: Challenges in Electrocardiogram Diagnosisheni arisNo ratings yet
- Simposium Iii. 2. Guch. Dr. L. Krisdinarti SPPD SPJPK PDFDocument33 pagesSimposium Iii. 2. Guch. Dr. L. Krisdinarti SPPD SPJPK PDFbagus krisnaNo ratings yet
- Ecg ReadingsDocument11 pagesEcg ReadingsAnton Laurenciana100% (5)
- Almaghrabi Cardio ExaminationDocument22 pagesAlmaghrabi Cardio ExaminationSagit Nauman81No ratings yet
- Prometric McqsDocument30 pagesPrometric Mcqsjishan8250% (2)
- ECG QuizDocument6 pagesECG QuizIsland Rae100% (1)
- Singh-Vaughan Williams ClassificationDocument2 pagesSingh-Vaughan Williams ClassificationMajeed QasimNo ratings yet
- Mitral Valve ProlapseDocument6 pagesMitral Valve ProlapseMary Joy FrancoNo ratings yet
- Lapkas PP (STEMI)Document68 pagesLapkas PP (STEMI)KurbulNo ratings yet
- Normal Sinus RhythmDocument97 pagesNormal Sinus RhythmNatasha LiberisNo ratings yet
- ACLS AritmiaDocument18 pagesACLS AritmiaZega AgustianNo ratings yet
- ACLS Tachycardia Algorithm For Managing Unstable TachycardiaDocument2 pagesACLS Tachycardia Algorithm For Managing Unstable TachycardiaLady MuffinsNo ratings yet
- Electrophysiology Study and Cardiac AblationDocument29 pagesElectrophysiology Study and Cardiac AblationBat ManNo ratings yet
- 2.2 Arrhythmia Dr. PayawalDocument7 pages2.2 Arrhythmia Dr. PayawalRaymond SantiagoNo ratings yet
- Cubeholter ENG Rev02Document2 pagesCubeholter ENG Rev02Maria Fernanda Hurtado0% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (79)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)