You might also like
- Extracranial Carotid and Vertebral Artery Disease: Contemporary ManagementFrom EverandExtracranial Carotid and Vertebral Artery Disease: Contemporary ManagementNo ratings yet
- Traumatic CSF LeaksDocument17 pagesTraumatic CSF LeaksNada AhmedNo ratings yet
- Posterior Circulation Stroke: Advances in Understanding and ManagementFrom EverandPosterior Circulation Stroke: Advances in Understanding and ManagementJong S. KimNo ratings yet
- CSF and Hydrocephalus: Physiology, Diagnosis, and TreatmentDocument3 pagesCSF and Hydrocephalus: Physiology, Diagnosis, and TreatmentagriNo ratings yet
- Hydrocephalus & ShuntsDocument9 pagesHydrocephalus & ShuntsVaseem ZamairNo ratings yet
- Ajns 11 183Document11 pagesAjns 11 183Salomo MahaputraNo ratings yet
- Hydro Cep Hal UsDocument7 pagesHydro Cep Hal Usalex soaresNo ratings yet
- CSF LeaksDocument3 pagesCSF LeaksDrTarek Mahmoud Abo KammerNo ratings yet
- CSF Rhinorrhea ReviewDocument7 pagesCSF Rhinorrhea ReviewPranave PNo ratings yet
- Traumatic Cerebrospinal Fluid Leak: Diagnosis and ManagementDocument5 pagesTraumatic Cerebrospinal Fluid Leak: Diagnosis and ManagementdittttttNo ratings yet
- HydrocephalusDocument50 pagesHydrocephalusedmelitanteNo ratings yet
- The Long-Term Sustainability of Procedures Identified With HydrocephalusDocument2 pagesThe Long-Term Sustainability of Procedures Identified With HydrocephalusInternational Journal of Innovative Science and Research Technology100% (1)
- Case Pres - HydrocephalusDocument26 pagesCase Pres - HydrocephalusJack Bisarra Sanchez100% (1)
- Cerebrospinal Fluid Circulation and HydrocephalusDocument12 pagesCerebrospinal Fluid Circulation and HydrocephalusI'Jaz Farritz MuhammadNo ratings yet
- A Lumbar PunctureDocument6 pagesA Lumbar PunctureNivinj KennedyNo ratings yet
- Ana & Physio HydrocephalusDocument4 pagesAna & Physio HydrocephalusJane VargasNo ratings yet
- Hydrocephalus Brain Condition Causes Fluid BuildupDocument6 pagesHydrocephalus Brain Condition Causes Fluid BuildupAntok ImanuelNo ratings yet
- Cerebrospinal Fluid Rhinorrhea: Diagnosis and Management: Julie T. Kerr, MD, Felix W.K. Chu, MD, Stephen W. Bayles, MDDocument15 pagesCerebrospinal Fluid Rhinorrhea: Diagnosis and Management: Julie T. Kerr, MD, Felix W.K. Chu, MD, Stephen W. Bayles, MDapasic9833No ratings yet
- HydrocephalusDocument40 pagesHydrocephalusAstrid Sabirin100% (1)
- What is HydrocephalusDocument16 pagesWhat is HydrocephalusYos AkbarNo ratings yet
- (19330693 - Journal of Neurosurgery) Superior Semicircular Canal Dehiscence Syndrome - CopieDocument9 pages(19330693 - Journal of Neurosurgery) Superior Semicircular Canal Dehiscence Syndrome - CopieCarmen-BadeaNo ratings yet
- Review of The Treatment & Management of Hydrocephalus: Jacqueline Groat, Pharmd CandidateDocument9 pagesReview of The Treatment & Management of Hydrocephalus: Jacqueline Groat, Pharmd CandidateAsif KhanNo ratings yet
- Hydrocephalus: Prepared By: Sita PariyarDocument38 pagesHydrocephalus: Prepared By: Sita PariyarSarita PariyarNo ratings yet
- Understanding Hydrocephalus: Causes, Symptoms and TreatmentDocument39 pagesUnderstanding Hydrocephalus: Causes, Symptoms and TreatmentAjeng Aristiany Rahawarin100% (1)
- Documento PDFDocument5 pagesDocumento PDFJose Miguel CastellonNo ratings yet
- Cerebrospinal Fluid Leaks: Michael E. Decherd, MD Byron J. Bailey, MD May 26, 1999Document6 pagesCerebrospinal Fluid Leaks: Michael E. Decherd, MD Byron J. Bailey, MD May 26, 1999Lina PratiwiNo ratings yet
- Congenitalhydrocephalus: Chelsie M. EsteyDocument13 pagesCongenitalhydrocephalus: Chelsie M. Esteyfalon papalangiNo ratings yet
- Adenosine-Induced Transient Asystole: Gavin W. Britz, M.D., M.P.HDocument4 pagesAdenosine-Induced Transient Asystole: Gavin W. Britz, M.D., M.P.HAnkitaNo ratings yet
- Cerebral Venous ThrombosisDocument19 pagesCerebral Venous ThrombosisgresiaNo ratings yet
- Persistent Posttraumatic Cerebrospinal Fluid Leakage: J A. F, M.D., M J. E, M.D., L M. Q, R.NDocument5 pagesPersistent Posttraumatic Cerebrospinal Fluid Leakage: J A. F, M.D., M J. E, M.D., L M. Q, R.NAlexanderCahyadiNo ratings yet
- (10920684 - Neurosurgical Focus) Endovascular Management of Fusiform Aneurysms in The Posterior Circulation - The Era of Flow DiversionDocument7 pages(10920684 - Neurosurgical Focus) Endovascular Management of Fusiform Aneurysms in The Posterior Circulation - The Era of Flow DiversionCharles MorrisonNo ratings yet
- 121 Anaesthesia For VP Shunt InsertionDocument8 pages121 Anaesthesia For VP Shunt InsertionMohammed ElSayedNo ratings yet
- Hydrocephalus PDFDocument17 pagesHydrocephalus PDFEdna López100% (1)
- Cs Leak 0210021Document8 pagesCs Leak 0210021Joshua SitorusNo ratings yet
- Procedure: Positioning in Lumbar PunctureDocument7 pagesProcedure: Positioning in Lumbar PunctureUsama El BazNo ratings yet
- CraniectomyDocument6 pagesCraniectomyale saenzNo ratings yet
- Increased Intracranial PressureDocument16 pagesIncreased Intracranial PressureArleth Fabian Sandoval GómezNo ratings yet
- Anesthesia For Cerebral - AneurysmsDocument14 pagesAnesthesia For Cerebral - AneurysmsDaniel BellemareNo ratings yet
- 2016 Pediatric HydrocephalusDocument15 pages2016 Pediatric HydrocephalusYudit Arenita100% (1)
- Hydro Cep Hal UsDocument65 pagesHydro Cep Hal UsKrisna MuhammadNo ratings yet
- Epistaxis: Clinical PracticeDocument8 pagesEpistaxis: Clinical PracticebadrhashmiNo ratings yet
- Ventriculoperitoneal Shunt - StatPearls - NCBI Bookshelf 2Document8 pagesVentriculoperitoneal Shunt - StatPearls - NCBI Bookshelf 2Erick DjuandaNo ratings yet
- Pathophysiology of Cerebral Venous Thrombosis - An Overview.Document4 pagesPathophysiology of Cerebral Venous Thrombosis - An Overview.claudio RivasNo ratings yet
- Lumbar Puncture ResearchDocument6 pagesLumbar Puncture Researchanon_464104226No ratings yet
- Cerebral Venous ThrombosisDocument15 pagesCerebral Venous ThrombosisValentina RobuNo ratings yet
- HydrocephalusDocument13 pagesHydrocephalusKyunaNo ratings yet
- Diagnosis ToxoplasamaDocument15 pagesDiagnosis ToxoplasamaHendik RiawanNo ratings yet
- STENOZA APEDUCTULUI LUI SylviusDocument23 pagesSTENOZA APEDUCTULUI LUI SylviusBogdan ȘtefîrcăNo ratings yet
- CranioplastyDocument9 pagesCranioplastyPamela MierNo ratings yet
- Cornell A 2003Document13 pagesCornell A 2003dnazaryNo ratings yet
- Controversies in The Neurosurgical Management of Cerebellar Hemorrhage and InfarctionDocument10 pagesControversies in The Neurosurgical Management of Cerebellar Hemorrhage and InfarctionThiago SouzaNo ratings yet
- Hydro ManagementDocument7 pagesHydro ManagementHadaAtiyehNo ratings yet
- Aneurysmal Subarachnoid Hemorrhage.6Document19 pagesAneurysmal Subarachnoid Hemorrhage.6Aldy Setiawan PutraNo ratings yet
- Berg Sneider 2008Document18 pagesBerg Sneider 2008dnazaryNo ratings yet
- Cerebrospinal FluidDocument15 pagesCerebrospinal FluidAdriana SandovalNo ratings yet
- DIAGNOSING COMMUNICATING HYDROCEPHALUS IN MPSDocument2 pagesDIAGNOSING COMMUNICATING HYDROCEPHALUS IN MPSNouchan NoupNo ratings yet
- Bahan Hidrosefalus2Document17 pagesBahan Hidrosefalus2Arry Wijaya LieNo ratings yet
- Hydrocephalus 2Document8 pagesHydrocephalus 2caliptra36No ratings yet
- Severe Headache InvestigatedDocument8 pagesSevere Headache Investigatedfire_n_iceNo ratings yet
- Lalou2019 Article CouplingOfCSFAndSagittalSinusPDocument9 pagesLalou2019 Article CouplingOfCSFAndSagittalSinusPDespina Aphroditi LalouNo ratings yet
- A Systemic Approach To Facial Nerve ParalysisDocument11 pagesA Systemic Approach To Facial Nerve Paralysissudheer joelNo ratings yet
- Embolisation in ENTDocument9 pagesEmbolisation in ENTsudheer joelNo ratings yet
- Chemoprevention in HNSDocument16 pagesChemoprevention in HNSsudheer joelNo ratings yet
- Carotid Body Tumors - Chemodectoma - Clinical Features and TreatmentDocument31 pagesCarotid Body Tumors - Chemodectoma - Clinical Features and Treatmentsudheer joelNo ratings yet
- MCQ Final 2014Document19 pagesMCQ Final 2014JohnSon100% (1)
- Won Lee Minimally Invasive Aesthetic Surgery Techniques BotulinumDocument243 pagesWon Lee Minimally Invasive Aesthetic Surgery Techniques Botulinumlorena gurdzNo ratings yet
- Neural Tube DefectDocument21 pagesNeural Tube Defectmariam bassemNo ratings yet
- Chapter 8 Special SensesDocument5 pagesChapter 8 Special SensesEdralyn EgaelNo ratings yet
- LipflpbotoxDocument4 pagesLipflpbotoxAlexandra Luz StodieckNo ratings yet
- Understanding the Structure and Function of NeuronsDocument99 pagesUnderstanding the Structure and Function of Neurons[R2A] Khadijah AzlanNo ratings yet
- Head and Neck Anatomy and Pathology MnemonicsDocument56 pagesHead and Neck Anatomy and Pathology MnemonicsMary Rose JuanNo ratings yet
- IV. Choose the correct answer from between bracketsDocument15 pagesIV. Choose the correct answer from between bracketsMostafa ElsayedNo ratings yet
- Performance Evaluation Checklist Assessment of The Eyes: Tarlac State University College of Science Nursing DepartmentDocument10 pagesPerformance Evaluation Checklist Assessment of The Eyes: Tarlac State University College of Science Nursing DepartmentArt russelNo ratings yet
- Novel Removable Appliance for Intruding Protruded IncisorDocument10 pagesNovel Removable Appliance for Intruding Protruded Incisordinda wrNo ratings yet
- Skin Functions and LayersDocument30 pagesSkin Functions and LayersAswin Gumelar R.No ratings yet
- Skull TopographyDocument43 pagesSkull TopographyGernalyn Ann MagayagaNo ratings yet
- Eye Anatomy MCQsDocument78 pagesEye Anatomy MCQsحلو المذاق100% (2)
- Past Papers 201 400 1Document48 pagesPast Papers 201 400 1shruti manzeNo ratings yet
- Blood Supply of BrainDocument54 pagesBlood Supply of Brainsaniasddq1110No ratings yet
- Pupil AssessmentDocument2 pagesPupil AssessmentJiezl Abellano AfinidadNo ratings yet
- J Ajodo 2010 02 021Document7 pagesJ Ajodo 2010 02 021leoncio cabrera rojasNo ratings yet
- Geographic TongueDocument3 pagesGeographic TongueIrsalina SalmaNo ratings yet
- PerDev - Q1 - Module 5 - Powers of The MindDocument31 pagesPerDev - Q1 - Module 5 - Powers of The MindMary Joy Calimlim Solis100% (1)
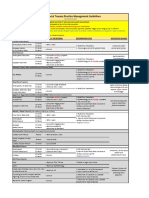
- VUMC Facial Trauma Practice Management GuidelinesDocument1 pageVUMC Facial Trauma Practice Management GuidelinesIndra D KristionoNo ratings yet
- Ophthalmology Set 5Document5 pagesOphthalmology Set 5ajay khadeNo ratings yet
- Cns Ospe Physiology HandoutDocument24 pagesCns Ospe Physiology HandoutBaby HanmiNo ratings yet
- Hear It For Your EarsDocument11 pagesHear It For Your EarsMark Anthony TubioNo ratings yet
- Detecting The Environment: Multiple-Choice QuestionsDocument111 pagesDetecting The Environment: Multiple-Choice Questionsdds uwuNo ratings yet
- Posterior Tooth Arrangement LectureDocument5 pagesPosterior Tooth Arrangement LectureDr.Maher MohammedNo ratings yet
- اسئلة تشريحDocument20 pagesاسئلة تشريحابراهيم فلاح حسنNo ratings yet
- SBF3033 Lab 1Document22 pagesSBF3033 Lab 1Nadia NasirNo ratings yet
- Arnett Combined Orthodontic and Surgical Open Bite CorrectionDocument12 pagesArnett Combined Orthodontic and Surgical Open Bite CorrectionAlex ReaNo ratings yet
- Year 9 Chapter 8 Sense and Control Sample AnswersDocument80 pagesYear 9 Chapter 8 Sense and Control Sample Answerskyle leeNo ratings yet
- The Brain Fitness Book Activities and Puzzles To Keep Your Mind Active and Healthy (Rita Carter) (Z-Library)Document192 pagesThe Brain Fitness Book Activities and Puzzles To Keep Your Mind Active and Healthy (Rita Carter) (Z-Library)Richard Wokard100% (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)