You might also like
- Dark Digital Planner - World of PrintablesDocument58 pagesDark Digital Planner - World of PrintablesS Co67% (3)
- Adolescence NutritionDocument43 pagesAdolescence NutritiontatadhNo ratings yet
- Pathophysiology of Diabetes Mellitus Type IIDocument4 pagesPathophysiology of Diabetes Mellitus Type IIEricka Genove100% (1)
- Teaching Exercise to Children: A Complete Guide to Theory and PracticeFrom EverandTeaching Exercise to Children: A Complete Guide to Theory and PracticeRating: 5 out of 5 stars5/5 (1)
- Sedentary Lifestyle: Health ImplicationsDocument6 pagesSedentary Lifestyle: Health ImplicationsInternational Organization of Scientific Research (IOSR)100% (1)
- USWR v5n1p11 enDocument8 pagesUSWR v5n1p11 enSoare Elena-CosminaNo ratings yet
- Klapp MethodDocument7 pagesKlapp MethodRJLeddaNo ratings yet
- ARTICLEMuscle Mass Measured Using Bioelectrical Impedanceanalysis, Calf Circumference and Grip Strength in OlderadultsDocument5 pagesARTICLEMuscle Mass Measured Using Bioelectrical Impedanceanalysis, Calf Circumference and Grip Strength in OlderadultsPPDS Rehab Medik UnhasNo ratings yet
- JKPT027 03 169Document5 pagesJKPT027 03 169Hendra Guntur BarunaNo ratings yet
- 2017 - Kwon - A Study On The Physical Fitness On Children With JRADocument6 pages2017 - Kwon - A Study On The Physical Fitness On Children With JRAkenmitaNo ratings yet
- A Study of The Clinical Test of Sensory Interaction and Balance.Document6 pagesA Study of The Clinical Test of Sensory Interaction and Balance.Olivia XuNo ratings yet
- Clinical Biomechanics: A A C C A BDocument6 pagesClinical Biomechanics: A A C C A BJorge De Araujo RochaNo ratings yet
- Effects of Obesity and Chronic Low Back Pain On Gait: Research Open AccessDocument7 pagesEffects of Obesity and Chronic Low Back Pain On Gait: Research Open AccessHumberto CastroNo ratings yet
- Changes in Gait Parameter With Adolescent Idiopatic ScoliosisDocument4 pagesChanges in Gait Parameter With Adolescent Idiopatic ScoliosisDariusNo ratings yet
- Inclination, Hip Abduction, Orientation, andDocument9 pagesInclination, Hip Abduction, Orientation, andFelipe AmorimNo ratings yet
- Correlation Between Waist and Mid-Thigh Circumference and Cardiovascular Fitness in Korean College Students: A Case StudyDocument3 pagesCorrelation Between Waist and Mid-Thigh Circumference and Cardiovascular Fitness in Korean College Students: A Case StudyAndres CaceresNo ratings yet
- Fatiga y Control Postural DinamicoDocument19 pagesFatiga y Control Postural DinamicoPatricio Alejandro Gaete PobleteNo ratings yet
- Comparison of The Effects of Exercise by Chronic Stroke Patients in Aquatic and Land EnvironmentsDocument4 pagesComparison of The Effects of Exercise by Chronic Stroke Patients in Aquatic and Land Environmentsilona ilincaNo ratings yet
- Does Sarcopenia Predict Change in Mobility After Hip Fracture? A Multicenter Observational Study With One-Year Follow-UpDocument10 pagesDoes Sarcopenia Predict Change in Mobility After Hip Fracture? A Multicenter Observational Study With One-Year Follow-UpliantariNo ratings yet
- Gait & Posture: SciencedirectDocument8 pagesGait & Posture: Sciencedirectاحمد العايديNo ratings yet
- Tai chi improves proprioception in elderlyDocument5 pagesTai chi improves proprioception in elderlyPhooi Yee LauNo ratings yet
- Physical Activity and Sarcopenic Obesity: Definition, Assessment, Prevalence and MechanismDocument19 pagesPhysical Activity and Sarcopenic Obesity: Definition, Assessment, Prevalence and MechanismCaro ArduzoNo ratings yet
- Jpts 27 2621Document4 pagesJpts 27 2621vvNo ratings yet
- Relationship Between Standing Posture Stability: WordsDocument16 pagesRelationship Between Standing Posture Stability: WordsVizaNo ratings yet
- Ggi12193 PDF Jsessionid f01t02Document9 pagesGgi12193 PDF Jsessionid f01t02omboNo ratings yet
- 2021 Dynapenia Roberta Age and AgingDocument10 pages2021 Dynapenia Roberta Age and Agingmariasol63No ratings yet
- Adolescent Obesity, Joint Pain, and Hypermobility: Shortreport Open AccessDocument5 pagesAdolescent Obesity, Joint Pain, and Hypermobility: Shortreport Open AccessMCuk2606No ratings yet
- Assessing The Relationship BetweenDocument6 pagesAssessing The Relationship BetweenTri Eka JuliantoNo ratings yet
- Effect of Passive Range of MotionDocument13 pagesEffect of Passive Range of Motionanggaarfina051821No ratings yet
- Balace 2Document7 pagesBalace 2astrinila fauziNo ratings yet
- Aging, Muscle Activity, and Balance Control: Physiologic Changes Associated With Balance ImpairmentDocument8 pagesAging, Muscle Activity, and Balance Control: Physiologic Changes Associated With Balance ImpairmentFrancisco Vicent PachecoNo ratings yet
- 10 30621-Jbachs 1261701-2996283Document10 pages10 30621-Jbachs 1261701-2996283Mina RizqinaNo ratings yet
- Comparing The Effects of Aquatic and Land-Based Exercises On Balance and Walking in Spastic Diplegic Cerebral Palsy ChildrenDocument8 pagesComparing The Effects of Aquatic and Land-Based Exercises On Balance and Walking in Spastic Diplegic Cerebral Palsy ChildrenJorgeAdalbertoCabralPerezNo ratings yet
- Rehabilitacion en NiñosDocument6 pagesRehabilitacion en NiñosYasser SaraviaNo ratings yet
- Correlation Between Gait and Balance in People With and Without Type 2 Diabetes in Normal and Subdued LightDocument9 pagesCorrelation Between Gait and Balance in People With and Without Type 2 Diabetes in Normal and Subdued LightFelipe RetamalNo ratings yet
- Balance-And Strength-Training Protocols To Improve Chronic Ankle Instability Deficits, Part I: Assessing Clinical Outcome MeasuresDocument10 pagesBalance-And Strength-Training Protocols To Improve Chronic Ankle Instability Deficits, Part I: Assessing Clinical Outcome MeasuresGorkaBuesaNo ratings yet
- Beyer 2007Document10 pagesBeyer 2007DR NOOR AZLIYANA AZIZANNo ratings yet
- Activity Modification and Knee Strengthening For Osgood-Schlatter DiseaseDocument9 pagesActivity Modification and Knee Strengthening For Osgood-Schlatter DiseaseSebastian FandiñoNo ratings yet
- Bioengineering 09 00538 v2Document9 pagesBioengineering 09 00538 v2Nadia KamilahNo ratings yet
- Effectiveness of Klapp Exercise To Treat Angle Currence in Children With Scoliosis: Literature ReviewDocument11 pagesEffectiveness of Klapp Exercise To Treat Angle Currence in Children With Scoliosis: Literature ReviewAlejandra GiraldoNo ratings yet
- Otago Home-Based Strength and Balance Retraining Improves Executive Functioning in Older Fallers - A Randomized Controlled Trial.Document10 pagesOtago Home-Based Strength and Balance Retraining Improves Executive Functioning in Older Fallers - A Randomized Controlled Trial.Ed RibeiroNo ratings yet
- Subcutaneous Thigh Fat Assessment: A Comparison of Skinfold Calipers and Ultrasound ImagingDocument6 pagesSubcutaneous Thigh Fat Assessment: A Comparison of Skinfold Calipers and Ultrasound ImagingNicole NgoNo ratings yet
- Weight Bearing Versus Non-Weight Bearing Ankle DorsiflexionDocument7 pagesWeight Bearing Versus Non-Weight Bearing Ankle Dorsiflexiongisela duarteNo ratings yet
- 2018 Article 2834Document11 pages2018 Article 2834mitroisergiuNo ratings yet
- Water-Versus Land-Based Exercise Effects On Physical Fitness in Older WomenDocument8 pagesWater-Versus Land-Based Exercise Effects On Physical Fitness in Older WomenHONGJY100% (1)
- Research Article: The Influence of The The Sagittal Spinal Curvatures in Children With Generalized Joint HypermobilityDocument7 pagesResearch Article: The Influence of The The Sagittal Spinal Curvatures in Children With Generalized Joint Hypermobilitysaarita lozano piedraNo ratings yet
- PQ Art 47262-10Document6 pagesPQ Art 47262-10tayfunertebelNo ratings yet
- Li-2001-Marcha-3 PuntosDocument7 pagesLi-2001-Marcha-3 PuntosFernando Ortiz CorredorNo ratings yet
- Effects_of_Diaphragmatic_Breathing_PatteDocument7 pagesEffects_of_Diaphragmatic_Breathing_Patteccaneccorso1971 ŻukowskaNo ratings yet
- Effects of Diaphragmatic Breathing Patterns On Balance: A Preliminary Clinical TrialDocument7 pagesEffects of Diaphragmatic Breathing Patterns On Balance: A Preliminary Clinical TrialN onlyNo ratings yet
- Lopes 2017Document7 pagesLopes 2017alonsoNo ratings yet
- (129 136) V9N5PTDocument8 pages(129 136) V9N5PTAqila NurNo ratings yet
- Jurnal Geriatri 9Document6 pagesJurnal Geriatri 9Villia DamayantieNo ratings yet
- Ajustes Posturales Anticipatorios y Compensatorios en PCDocument10 pagesAjustes Posturales Anticipatorios y Compensatorios en PCPamela DíazNo ratings yet
- 2487 9752 2 PBDocument9 pages2487 9752 2 PBAnisNo ratings yet
- Schenkman: Exercise To Improve Spinal Flexibility and Function For People With Parkinson's Disease: A Randomized, Controlled TrialDocument10 pagesSchenkman: Exercise To Improve Spinal Flexibility and Function For People With Parkinson's Disease: A Randomized, Controlled TrialGerman BuyattiNo ratings yet
- The Six-Minute Walk Test in Outpatients With Obesity: Reproducibility and Known Group ValidityDocument10 pagesThe Six-Minute Walk Test in Outpatients With Obesity: Reproducibility and Known Group ValidityErick Andrade IbarraNo ratings yet
- Exercise and Physical Performance in Older Adults With Sarcopenic Obesity: A Systematic ReviewDocument13 pagesExercise and Physical Performance in Older Adults With Sarcopenic Obesity: A Systematic ReviewAgatha GeraldyneNo ratings yet
- BMC NeurologyDocument9 pagesBMC NeurologyBASHArnNo ratings yet
- Land 2017 - Effect of Manual Physiotherapy in Homogeneous Individuals With Subacromial Shoulder Impingement - A Randomized Controlled TrialDocument14 pagesLand 2017 - Effect of Manual Physiotherapy in Homogeneous Individuals With Subacromial Shoulder Impingement - A Randomized Controlled TrialJime PENo ratings yet
- Lumbar Stability PDFDocument9 pagesLumbar Stability PDFPablo EstebanNo ratings yet
- Prediction of Insulin Resistance in Late Adolescent Based On Anthropometric IndexDocument8 pagesPrediction of Insulin Resistance in Late Adolescent Based On Anthropometric IndexDewantari BambangNo ratings yet
- Basic Exercise Physiology: Clinical and Laboratory PerspectivesFrom EverandBasic Exercise Physiology: Clinical and Laboratory PerspectivesNo ratings yet
- The ASMBS Textbook of Bariatric Surgery: Volume 1: Bariatric SurgeryFrom EverandThe ASMBS Textbook of Bariatric Surgery: Volume 1: Bariatric SurgeryNo ratings yet
- RP Draft 1 Eng 1201 Sec 509 8Document13 pagesRP Draft 1 Eng 1201 Sec 509 8api-609285394No ratings yet
- PREFIT MANUAL - Assessing FITness in PREschoolers - 14thsept2017Document34 pagesPREFIT MANUAL - Assessing FITness in PREschoolers - 14thsept2017Natalia GutierrezNo ratings yet
- SL Paper 3: Two Dietary Sources of Vitamin DDocument28 pagesSL Paper 3: Two Dietary Sources of Vitamin DSugey Constante ToalaNo ratings yet
- Inglés Junio 1-5 PDFDocument6 pagesInglés Junio 1-5 PDFJuan DiegoNo ratings yet
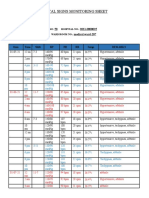
- Vital Signs Monitoring SheetDocument2 pagesVital Signs Monitoring SheetRenea Joy ArruejoNo ratings yet
- Daftar Pustaka: Strokenews/Coronary-Arterydisease - The-Abcs Ofcad - Ucm - 436416 - Article - JSPDocument3 pagesDaftar Pustaka: Strokenews/Coronary-Arterydisease - The-Abcs Ofcad - Ucm - 436416 - Article - JSPmuhamad isafarudinNo ratings yet
- Individual Pace Planner for Personal Fitness CourseDocument5 pagesIndividual Pace Planner for Personal Fitness CourseNolan RiddleNo ratings yet
- (ThichTiengAnh - Com) De-Thi-Thu-Thptqglan-1nam-2017-Truong-Thpt-Nguyen-Binh-Khiemquang-NamDocument23 pages(ThichTiengAnh - Com) De-Thi-Thu-Thptqglan-1nam-2017-Truong-Thpt-Nguyen-Binh-Khiemquang-NamBach Hua HuaNo ratings yet
- IELTS Reading Yes, No, Not Given TipsDocument7 pagesIELTS Reading Yes, No, Not Given Tipsmenta gintingNo ratings yet
- Importance of SleepDocument4 pagesImportance of SleepNabila SalsaNo ratings yet
- Body Image Disorders DebateDocument10 pagesBody Image Disorders DebatePATRICIA MAE CABANANo ratings yet
- Body Fat Monitor HBF-306: Instruction ManualDocument20 pagesBody Fat Monitor HBF-306: Instruction Manual윤여평No ratings yet
- Pathophysiology of Gestational Diabetes Mellitus: AuthorDocument10 pagesPathophysiology of Gestational Diabetes Mellitus: AuthorMayra PereiraNo ratings yet
- MAPEH - (PE8) - Q1 - Mod1 - Ver1.0 TeachersDocument8 pagesMAPEH - (PE8) - Q1 - Mod1 - Ver1.0 TeachersALBERT IAN CASUGANo ratings yet
- Addressing overweight, obesity and NCDs through lifestyle changesDocument33 pagesAddressing overweight, obesity and NCDs through lifestyle changesSiti Ika FitrasyahNo ratings yet
- Obesity: A Health and Social IssueDocument4 pagesObesity: A Health and Social IssueDumb PepeNo ratings yet
- High Intensity Interval Training Is Not Superior To Contin - 2023 - Journal of EDocument10 pagesHigh Intensity Interval Training Is Not Superior To Contin - 2023 - Journal of ESherriNo ratings yet
- PFT FormDocument4 pagesPFT FormBreylyn Guitarte Acopiado RapistaNo ratings yet
- General Physics 1 Activity 1Document2 pagesGeneral Physics 1 Activity 1Margarette Yssabelle VillarNo ratings yet
- 1161 Jphi QCRDDocument6 pages1161 Jphi QCRDamar prasadNo ratings yet
- Final ProgrammeDocument204 pagesFinal ProgrammeimagigatoNo ratings yet
- If Clauses ExerciseDocument6 pagesIf Clauses ExerciseJeff CadetNo ratings yet
- Forms 1Document2 pagesForms 1Diana Rose Jimenez MarasiganNo ratings yet
- 3 2 5 HansDocument4 pages3 2 5 Hansapi-34377161857% (7)
- OMS. IMC Meninas - 5-19 Anos. em Percentil.Document1 pageOMS. IMC Meninas - 5-19 Anos. em Percentil.anaclaraamaralf2002No ratings yet
- Uncontrolled T2DMDocument1 pageUncontrolled T2DMMickinzieNo ratings yet