You might also like
- A Project Management System Based On The PMBOK Guide For Student-Centered LearningDocument6 pagesA Project Management System Based On The PMBOK Guide For Student-Centered LearningdyasrennyNo ratings yet
- Benchmarking Engineering Curricula With The CDIO SyllabusDocument13 pagesBenchmarking Engineering Curricula With The CDIO SyllabussatishNo ratings yet
- 3140707_COA_Lab Manual_Even-2024.docx (1)Document59 pages3140707_COA_Lab Manual_Even-2024.docx (1)kunalkhairanar007No ratings yet
- Boden WorkshopHandbook 012508Document51 pagesBoden WorkshopHandbook 012508dinhcauduong12No ratings yet
- Lynch Seery Gordon - ISEE07 PDFDocument9 pagesLynch Seery Gordon - ISEE07 PDFTani RicafrenteNo ratings yet
- Project Based Learning in Wireless Communications Utilizing Deployed Wireless NetworksDocument6 pagesProject Based Learning in Wireless Communications Utilizing Deployed Wireless NetworksAnkit ShahNo ratings yet
- Project Portfolio Selection Using Interactive Approach: Maciej NowakDocument9 pagesProject Portfolio Selection Using Interactive Approach: Maciej Nowaknormand67No ratings yet
- Teaching Interior Design Methodology - A Case Study Shopping Mall Design Studio ProjectDocument9 pagesTeaching Interior Design Methodology - A Case Study Shopping Mall Design Studio ProjectAbrat RagulNo ratings yet
- Industrial Projects in A Project-Based Learning Environment: AbstractDocument6 pagesIndustrial Projects in A Project-Based Learning Environment: AbstractAnand BhiseNo ratings yet
- Conf DictapDocument6 pagesConf DictapImran Hossain TuhinNo ratings yet
- Students Perception of Capstone ProjectsDocument9 pagesStudents Perception of Capstone ProjectsRajani Gupta KamlapuriNo ratings yet
- Problem Based Learning in Engineering DesignDocument11 pagesProblem Based Learning in Engineering Designaugur886No ratings yet
- Case Study To Analyze The Impact of Multi-CourseDocument21 pagesCase Study To Analyze The Impact of Multi-CourseMiriam CollegeNo ratings yet
- Week 2 - A Sample of A Short Research ProposalDocument4 pagesWeek 2 - A Sample of A Short Research ProposalIsrael PopeNo ratings yet
- Practical Teaching and Its Importance in Teaching Civil EngineeringDocument4 pagesPractical Teaching and Its Importance in Teaching Civil EngineeringP.PENCHALA REDDY Structures HeadNo ratings yet
- Program Curriculum and Teaching-Learning ProcessesDocument5 pagesProgram Curriculum and Teaching-Learning ProcessesAshok DaraNo ratings yet
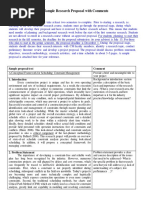
- A Sample Proposal With CommentDocument6 pagesA Sample Proposal With CommentgalNo ratings yet
- Teaching Plant Design Material Handling by Project Based ApproachDocument10 pagesTeaching Plant Design Material Handling by Project Based ApproachMohamed MustefaNo ratings yet
- Project Based Learning Benefits Engineering StudentsDocument8 pagesProject Based Learning Benefits Engineering StudentsagushattaNo ratings yet
- Ds NarjjisDocument98 pagesDs Narjjisghasadiyakrisha211No ratings yet
- Environment Lab ManDocument105 pagesEnvironment Lab ManIshwar ChandraNo ratings yet
- Establishing Fair Objectives and Grading Criteria ForDocument18 pagesEstablishing Fair Objectives and Grading Criteria ForPraful KakdeNo ratings yet
- Changing An Engineering Curriculum Through A Co-Construction Process: A Case StudyDocument12 pagesChanging An Engineering Curriculum Through A Co-Construction Process: A Case StudyasparagusNo ratings yet
- Research Proposal Imrad Format With CommentsDocument6 pagesResearch Proposal Imrad Format With CommentsJoshua AndayaNo ratings yet
- Artigo Trainning Interior Designers To Project Feasibility StudiesDocument12 pagesArtigo Trainning Interior Designers To Project Feasibility StudiesCarol LimaNo ratings yet
- Approaches To The Teaching of Design: Engineering Subject Centre Guide by Andrew MclarenDocument24 pagesApproaches To The Teaching of Design: Engineering Subject Centre Guide by Andrew MclarenAnonymous i3HHYO8No ratings yet
- Research Paper 3.3Document19 pagesResearch Paper 3.3Sailee RedkarNo ratings yet
- Value Engineering As An Effective Tool For Improving The Performance of Students at The College of Engineering - King Saud UniversityDocument9 pagesValue Engineering As An Effective Tool For Improving The Performance of Students at The College of Engineering - King Saud UniversityM Ahmed LatifNo ratings yet
- Reverse Engineering Courses to Incrementally Teach DesignDocument12 pagesReverse Engineering Courses to Incrementally Teach DesignYatin NgadiyonoNo ratings yet
- ds62 078Document6 pagesds62 078Lihardo RanjalibaNo ratings yet
- OOP Lab Manual for Core Java ConceptsDocument91 pagesOOP Lab Manual for Core Java ConceptsKavish Panchal0% (1)
- Final Year Projects - A Means of Adding Value To Graduate AttributesDocument6 pagesFinal Year Projects - A Means of Adding Value To Graduate Attributesrajesh jamesNo ratings yet
- JEET261Document10 pagesJEET261acehabiniNo ratings yet
- Research Paper Latest TemplateDocument4 pagesResearch Paper Latest TemplateDaniel JohnsNo ratings yet
- Lab Manual SurveyDocument84 pagesLab Manual SurveyTamil Selvi CIVILNo ratings yet
- Power 2Document21 pagesPower 2Fabiola CruzNo ratings yet
- Concurrent Software Engineering Project: Executive SummaryDocument22 pagesConcurrent Software Engineering Project: Executive SummaryRajesh PawarNo ratings yet
- ارشادات عمل مشروع تخرجDocument19 pagesارشادات عمل مشروع تخرجelsayedyasser29No ratings yet
- Implementation of A PBL - CDIO Methodology at Systems Engineering CourseDocument8 pagesImplementation of A PBL - CDIO Methodology at Systems Engineering CourseGenaro MagiNo ratings yet
- The Praxis of Product Design in Collaboration with EngineeringFrom EverandThe Praxis of Product Design in Collaboration with EngineeringNo ratings yet
- An Enquiry-Based Chemical Engineering Design ProjectDocument8 pagesAn Enquiry-Based Chemical Engineering Design ProjectMuhammad SaeedNo ratings yet
- A Project-Based Learning Design For Teaching and Learning of Mechatronics EngineeringDocument6 pagesA Project-Based Learning Design For Teaching and Learning of Mechatronics Engineeringalejandro perdomoNo ratings yet
- Assessment - Engineering Materials - 3Document10 pagesAssessment - Engineering Materials - 3md.naimul HaqueNo ratings yet
- Teaching and Assessing Engineering Design Thinking With Virtual InternshipDocument14 pagesTeaching and Assessing Engineering Design Thinking With Virtual InternshipEngr. Ronnie SantelicesNo ratings yet
- ASEE 2015 Final PDFDocument10 pagesASEE 2015 Final PDFothmaneNo ratings yet
- Best Practices in Managing, Supervising, and Assessing Architectural Graduation Projects A Quantitative StudyDocument16 pagesBest Practices in Managing, Supervising, and Assessing Architectural Graduation Projects A Quantitative Studyarchi33No ratings yet
- 2018 JSS AgileEducationDocument18 pages2018 JSS AgileEducationWassila BENSAHELNo ratings yet
- Guidelines For FYPDocument12 pagesGuidelines For FYPHaiderAliNo ratings yet
- An Educational and Commercial Product Design Symbiosis: A Case StudyDocument6 pagesAn Educational and Commercial Product Design Symbiosis: A Case StudyShweta KulkarniNo ratings yet
- Problem Based Learning in Engineering DesignDocument12 pagesProblem Based Learning in Engineering DesignBrujoca BrujocaNo ratings yet
- Sample Proposal With CommentDocument3 pagesSample Proposal With CommentarulgasparNo ratings yet
- Challenge Driven Education in The Context of Internet of ThingsDocument6 pagesChallenge Driven Education in The Context of Internet of Thingspantzos.stockholm.suNo ratings yet
- Outcome Based Education: Vinaychandna@Yahoo - Co.InDocument17 pagesOutcome Based Education: Vinaychandna@Yahoo - Co.InTovindra Kumar SahuNo ratings yet
- Pedagogical Praxis in Architecture Design StudioDocument13 pagesPedagogical Praxis in Architecture Design StudioemadeldinhamdyNo ratings yet
- A Sample Proposal With CommentDocument3 pagesA Sample Proposal With CommentCarlo SanchezNo ratings yet
- A Sample Proposal With CommentDocument3 pagesA Sample Proposal With CommentTasnia MebinNo ratings yet
- The Importance of Prototyping For Education in Product Innovation EngineeringDocument9 pagesThe Importance of Prototyping For Education in Product Innovation EngineeringJ.C.VNo ratings yet
- Developing a Conceptual Framework for Construction Constraint ManagementDocument3 pagesDeveloping a Conceptual Framework for Construction Constraint ManagementramszlaiNo ratings yet
- Exploring the Complexity of Projects: Implications of Complexity Theory for Project Management PracticeFrom EverandExploring the Complexity of Projects: Implications of Complexity Theory for Project Management PracticeNo ratings yet
- ICT Project Management: Framework for ICT-based Pedagogy System: Development, Operation, and ManagementFrom EverandICT Project Management: Framework for ICT-based Pedagogy System: Development, Operation, and ManagementNo ratings yet
- Clinical Cardiology - April 1978 - Reichert - A History of The Development of Cardiology As A Medical Specialty PDFDocument11 pagesClinical Cardiology - April 1978 - Reichert - A History of The Development of Cardiology As A Medical Specialty PDFSakshi RangnekarNo ratings yet
- JDTP (North) Plan Details 2010-11Document15 pagesJDTP (North) Plan Details 2010-11Sakshi RangnekarNo ratings yet
- English 8TH PaperDocument8 pagesEnglish 8TH PaperSakshi RangnekarNo ratings yet
- Types of FlooringDocument11 pagesTypes of FlooringSakshi RangnekarNo ratings yet
- Working Drawing PageDocument1 pageWorking Drawing PageSakshi RangnekarNo ratings yet
- English 8TH PaperDocument8 pagesEnglish 8TH PaperSakshi RangnekarNo ratings yet
- The Impact of Economic News On Financial Markets - John ParkerDocument61 pagesThe Impact of Economic News On Financial Markets - John ParkerSakshi RangnekarNo ratings yet
- 1AA17AT009 - Trauma Centre by Ananya KulkarniDocument43 pages1AA17AT009 - Trauma Centre by Ananya KulkarniSakshi RangnekarNo ratings yet
- Fabric Types and Uses for Interior DesignDocument16 pagesFabric Types and Uses for Interior DesignSakshi RangnekarNo ratings yet
- Cardiology Hospital Synopsis by Sakshi RangnekarDocument1 pageCardiology Hospital Synopsis by Sakshi RangnekarSakshi RangnekarNo ratings yet
- Types of EcosystemsDocument10 pagesTypes of EcosystemsSakshi RangnekarNo ratings yet
- Test PDFDocument1 pageTest PDFSakshi RangnekarNo ratings yet
- Wall Cladding - 13 MM X 173 MMDocument1 pageWall Cladding - 13 MM X 173 MMSakshi RangnekarNo ratings yet
- Learning Transcript for Sakshi RangnekarDocument1 pageLearning Transcript for Sakshi RangnekarSakshi RangnekarNo ratings yet
- Fabric Types and Uses for UpholsteryDocument17 pagesFabric Types and Uses for UpholsterySakshi RangnekarNo ratings yet
- Printable Lawyer CV by SlidesgoDocument24 pagesPrintable Lawyer CV by SlidesgoOkto Wisnu NugrohoNo ratings yet
- 31 02 08 BrambillaDocument17 pages31 02 08 BrambillaArooj AnjumNo ratings yet
- 1 Parking FloorDocument1 page1 Parking FloorSakshi RangnekarNo ratings yet
- Xal Acoustic Lighting enDocument80 pagesXal Acoustic Lighting enSakshi RangnekarNo ratings yet
- CertificateDocument1 pageCertificateSakshi RangnekarNo ratings yet
- Assignment On PrincipalDocument10 pagesAssignment On PrincipalmacmohitNo ratings yet
- Caitlin Mariscal - Career Exploration WorksheetDocument2 pagesCaitlin Mariscal - Career Exploration Worksheetapi-389735946No ratings yet
- BPH treatment options and assessmentDocument7 pagesBPH treatment options and assessmentVon BellosilloNo ratings yet
- G1604056 CRC UnDocument19 pagesG1604056 CRC UnsofiabloemNo ratings yet
- Teks Percakapan Bahasa InggrisDocument2 pagesTeks Percakapan Bahasa Inggrisnaufal456No ratings yet
- Knowledge and Practices of Mothers On Nigeria PDFDocument11 pagesKnowledge and Practices of Mothers On Nigeria PDFalfinNo ratings yet
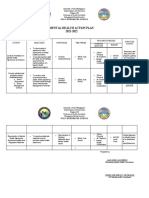
- Mental Health Action PlanDocument2 pagesMental Health Action PlanKenny Ann Grace Batiancila100% (9)
- Total Penectomy Urooncology 12thDocument10 pagesTotal Penectomy Urooncology 12thdr. Joko WibowoNo ratings yet
- Managing waste through technology and regulationDocument3 pagesManaging waste through technology and regulationNita ArviyaniNo ratings yet
- Nephrolithiasis - Drug StudyDocument5 pagesNephrolithiasis - Drug StudyAia JavierNo ratings yet
- 22 CR Protean NeurologicalDocument2 pages22 CR Protean NeurologicalCamii CvNo ratings yet
- Obsessive Compulsive DisorderDocument2 pagesObsessive Compulsive DisorderThomas ScottNo ratings yet
- Journal of Nutrition College,: Sensitivity C-Reactive Protein (HS-CRP) Pada RemajaDocument6 pagesJournal of Nutrition College,: Sensitivity C-Reactive Protein (HS-CRP) Pada RemajaDevi OktariaNo ratings yet
- Nurse Midwife PractionersDocument8 pagesNurse Midwife PractionersVineeta JoseNo ratings yet
- Lecture - Mental and Emotional HealthDocument5 pagesLecture - Mental and Emotional HealthRogerson PenaNo ratings yet
- Alt - Cancer (1) BookDocument419 pagesAlt - Cancer (1) Bookniceia matos100% (3)
- Case 1-2 Business Case Data Chaos Creates RiskDocument5 pagesCase 1-2 Business Case Data Chaos Creates RiskfauziahezzyNo ratings yet
- Implementasi SPM Kesehatan Bayi Baru Lahir di Puskesmas DukuhsetiDocument10 pagesImplementasi SPM Kesehatan Bayi Baru Lahir di Puskesmas DukuhsetiFidia sariNo ratings yet
- Assign No. 1 Module 6Document3 pagesAssign No. 1 Module 6Cindy Mae de la TorreNo ratings yet
- Glander DiseaseDocument1 pageGlander DiseaseAdams10No ratings yet
- Atos CFSDocument22 pagesAtos CFSPaul SmithNo ratings yet
- Hazardous Material Management ProcedureDocument9 pagesHazardous Material Management ProcedureozerNo ratings yet
- Mefenamic Acid Drug StudyDocument1 pageMefenamic Acid Drug StudyAj GoNo ratings yet
- Nursing Interventions for Fracture CareDocument2 pagesNursing Interventions for Fracture CareShekinah DomingoNo ratings yet
- Mental Health Weekly - May 16, 2016Document8 pagesMental Health Weekly - May 16, 2016Sharon A StockerNo ratings yet
- Sun Valley International School: COVID-19 Acknowledgement of Risk and Consent Form For StudentsDocument2 pagesSun Valley International School: COVID-19 Acknowledgement of Risk and Consent Form For StudentsAditya PariharNo ratings yet
- Population Trends in INDIADocument8 pagesPopulation Trends in INDIAcheedikrishnaNo ratings yet
- Nutrition Care Process Note-IcuDocument2 pagesNutrition Care Process Note-Icuapi-1032325430% (1)
- Barangay Nutrition Scholar ProgramDocument4 pagesBarangay Nutrition Scholar ProgramLenz BautistaNo ratings yet
- AWWA M3 Safety Mangement For Utilities 7th Ed 2014Document164 pagesAWWA M3 Safety Mangement For Utilities 7th Ed 2014Harold Fernando Guavita ReyesNo ratings yet