You might also like
- The Black Emperor's Grand Grimoire - by Frank GenghisDocument144 pagesThe Black Emperor's Grand Grimoire - by Frank GenghisFrank Genghis0% (2)
- Strategic Planning Assignment - TescoDocument16 pagesStrategic Planning Assignment - TescoKayode Trinity Omosebi100% (1)
- Spine Oncology, An Issue of Orthopedic Clinics PDFDocument168 pagesSpine Oncology, An Issue of Orthopedic Clinics PDFThanh Le DangNo ratings yet
- PR & PublicityDocument16 pagesPR & PublicityVipul Partap100% (2)
- ACR Thyroid Imaging, Reporting and Data 2018 TesslerDocument9 pagesACR Thyroid Imaging, Reporting and Data 2018 TesslerdianaveebaeNo ratings yet
- Expert Consensus Contouring Guidelines For Intensity Modulated Radiation Therapy in Esophageal and Gastroesophageal Junction CancerDocument10 pagesExpert Consensus Contouring Guidelines For Intensity Modulated Radiation Therapy in Esophageal and Gastroesophageal Junction CancermarrajoanaNo ratings yet
- The Science and Art of DSGE ModellingDocument9 pagesThe Science and Art of DSGE ModellingkeyyongparkNo ratings yet
- GCMS-QP2010 User'sGuide (Ver2.5) PDFDocument402 pagesGCMS-QP2010 User'sGuide (Ver2.5) PDFnguyenvietanhbtNo ratings yet
- Interrogating Texts: Six Reading Habits To Develop in Your First Year at HarvardDocument2 pagesInterrogating Texts: Six Reading Habits To Develop in Your First Year at HarvardS I ZahidNo ratings yet
- YLE - Top Tips and Common MistakesDocument15 pagesYLE - Top Tips and Common Mistakeskuvan alievNo ratings yet
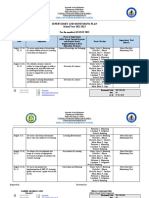
- Supervisory Plan 2022 2023Document4 pagesSupervisory Plan 2022 2023Jesieca Bulauan100% (12)
- RG Radiologists' Role in Breast Cancer StagingDocument14 pagesRG Radiologists' Role in Breast Cancer StagingAzucena BCNo ratings yet
- 10 1148@rg 2019180114Document21 pages10 1148@rg 2019180114alexandragherman92No ratings yet
- Thyroidcancer: Ultrasound Imaging and Fine-Needle Aspiration BiopsyDocument21 pagesThyroidcancer: Ultrasound Imaging and Fine-Needle Aspiration BiopsyPedro Gómez RNo ratings yet
- Tirads NuevoDocument13 pagesTirads NuevoLuisMamaniTercerosNo ratings yet
- 10 1053@j Semnuclmed 2020 07 005Document10 pages10 1053@j Semnuclmed 2020 07 005anon_813722240No ratings yet
- Clinical Practice Guidelines: Penile Cancer: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpDocument10 pagesClinical Practice Guidelines: Penile Cancer: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-Uphypebeast dopeNo ratings yet
- DTH 34 E14981Document9 pagesDTH 34 E14981Henry WijayaNo ratings yet
- P. Wang Et Al.2019Document6 pagesP. Wang Et Al.2019Mai M. AlshalNo ratings yet
- Jurnal CNFDocument36 pagesJurnal CNFAndrianorMuhammadNo ratings yet
- TIRADS2017Document9 pagesTIRADS2017Eliana RuizNo ratings yet
- LI-RADS Lesiones HepáticasDocument24 pagesLI-RADS Lesiones HepáticasvictoriaNo ratings yet
- Consensus Guidelines For Delineation of Clinical Target Volume For Intensity-Modulated Pelvic Radiotherapy in Postoperative Treatment of Endometrial and Cervical CancerDocument17 pagesConsensus Guidelines For Delineation of Clinical Target Volume For Intensity-Modulated Pelvic Radiotherapy in Postoperative Treatment of Endometrial and Cervical CancerJaime H. Soto LugoNo ratings yet
- Radiotherapy and OncologyDocument14 pagesRadiotherapy and OncologyJavier RodríguezNo ratings yet
- 2012 Renal Cell Carcinoma Metastasizing To Larynx A Case ReportDocument5 pages2012 Renal Cell Carcinoma Metastasizing To Larynx A Case ReportAlfonsoSánchezNo ratings yet
- MainDocument8 pagesMainIoana CucuNo ratings yet
- Imaging characteristics predict NPC metastasisDocument7 pagesImaging characteristics predict NPC metastasisJose JulianNo ratings yet
- 390 398MRIinRectalCA PDFDocument10 pages390 398MRIinRectalCA PDFHerve-narcisse N'goranNo ratings yet
- Australia - Asian AtlasDocument8 pagesAustralia - Asian AtlaszanNo ratings yet
- 10 1002@jmri 27182 PDFDocument10 pages10 1002@jmri 27182 PDFMădălina MoldovanuNo ratings yet
- Imaging Updates To Breast Cancer Lymph Node ManagementDocument17 pagesImaging Updates To Breast Cancer Lymph Node ManagementMinh Thư DươngNo ratings yet
- Elsholtz2021 NodeReportingDocument9 pagesElsholtz2021 NodeReportingDjabhi SpinzzNo ratings yet
- Palpable Lumps After MastectomyDocument23 pagesPalpable Lumps After MastectomyMinh Thư DươngNo ratings yet
- Cystic Lesions of The Pancreas - RadiologicEndosonographic CorrelationDocument20 pagesCystic Lesions of The Pancreas - RadiologicEndosonographic CorrelationVictor Kenzo IvanoNo ratings yet
- Imaging of Oncologic Emergencies What Every RadiolDocument23 pagesImaging of Oncologic Emergencies What Every RadiolJean Brando Torres GuerreroNo ratings yet
- 10 1111@codi 15424Document22 pages10 1111@codi 15424yongky sugandaNo ratings yet
- Jurnal Radiologi 2Document21 pagesJurnal Radiologi 2Adelya Dwi AsyifaNo ratings yet
- Staged Surgery For Advanced Thyroid Cancers: Safety and Oncologic Outcomes of Neural Monitored SurgeryDocument6 pagesStaged Surgery For Advanced Thyroid Cancers: Safety and Oncologic Outcomes of Neural Monitored SurgeryAprilihardini LaksmiNo ratings yet
- 1 s2.0 S105342962200056X MainDocument9 pages1 s2.0 S105342962200056X MainFatimah AssagafNo ratings yet
- Baek 2017Document10 pagesBaek 2017witaNo ratings yet
- Dem 2Document15 pagesDem 2paskisallaberryNo ratings yet
- Elective Neck Irradiation N0 Neck Jia KouDocument13 pagesElective Neck Irradiation N0 Neck Jia KouSanjog SinghNo ratings yet
- Surgery For Locally Advanced T4 Rectal CancerDocument8 pagesSurgery For Locally Advanced T4 Rectal CancerAnitei GabrielaNo ratings yet
- Rectal Cancer NLR and Lymphopenia Predict SurvivalDocument4 pagesRectal Cancer NLR and Lymphopenia Predict SurvivalRaul Matute MartinNo ratings yet
- CA MammaeDocument6 pagesCA MammaeRiaNo ratings yet
- 11 Preoperative - High - Neutrophil-Lymphocyte - Ratio - MayDocument8 pages11 Preoperative - High - Neutrophil-Lymphocyte - Ratio - MayBridia BogarNo ratings yet
- TNM+No+CA+de+Tireoide+ +2007Document9 pagesTNM+No+CA+de+Tireoide+ +2007aLineLanNo ratings yet
- Esophageal Cancer Recurrence Patterns and Implicati 2013 Journal of ThoracicDocument5 pagesEsophageal Cancer Recurrence Patterns and Implicati 2013 Journal of ThoracicFlorin AchimNo ratings yet
- Protocolo de Rayos en Esclerosis MultipleDocument8 pagesProtocolo de Rayos en Esclerosis MultipleFernando Dueñas MoralesNo ratings yet
- Diagnosis and Management of Squamous Cell Carcinoma of Unknown Primary in The Head and Neck - ASCO GuidelineDocument29 pagesDiagnosis and Management of Squamous Cell Carcinoma of Unknown Primary in The Head and Neck - ASCO GuidelineFabian Camelo OtorrinoNo ratings yet
- Lymph Nodes Normal and MalignantDocument12 pagesLymph Nodes Normal and MalignantMagzNo ratings yet
- Radiofrequency ablation efficacy for thyroid cancer typesDocument7 pagesRadiofrequency ablation efficacy for thyroid cancer typesivan dario hernandez erazoNo ratings yet
- 10 1093@icvts@ivz140Document8 pages10 1093@icvts@ivz140PEDRO JESuS GUERRA CANCHARINo ratings yet
- Prostate MRI and Image Quality The Radiologist'sDocument4 pagesProstate MRI and Image Quality The Radiologist'sdeaNo ratings yet
- Austin Journal of Nuclear Medicine and RadiotherapyDocument5 pagesAustin Journal of Nuclear Medicine and RadiotherapyAustin Publishing GroupNo ratings yet
- Thyroid Ultrasound, State of The ArtDocument15 pagesThyroid Ultrasound, State of The ArtDe DawnNo ratings yet
- Outcomes After Stereotactic Body Radiotherapy or Radiofrequency Ablation For Hepatocellular CarcinomaDocument10 pagesOutcomes After Stereotactic Body Radiotherapy or Radiofrequency Ablation For Hepatocellular CarcinomaRaul Matute MartinNo ratings yet
- Temporal Bone Carcinoma Classical Prognostic Vari - 2016 - Reports of PracticalDocument5 pagesTemporal Bone Carcinoma Classical Prognostic Vari - 2016 - Reports of PracticalOana VarvariNo ratings yet
- Testicular Cancer NCCN2015Document28 pagesTesticular Cancer NCCN2015palomazul007No ratings yet
- Writing Radiology Reports in ChiropracticDocument6 pagesWriting Radiology Reports in ChiropracticRohit SagarNo ratings yet
- Review Article Esophageal CancerDocument9 pagesReview Article Esophageal CancerMuhadis AhmadNo ratings yet
- 21 - Mark e Berry Guidelines Staging and TreatmentDocument9 pages21 - Mark e Berry Guidelines Staging and TreatmentNatalindah Jokiem Woecandra T. D.No ratings yet
- Glimelius 2013Document8 pagesGlimelius 2013Sofia SimpertigueNo ratings yet
- Baumann 2016 IJROBP Development Validation of Bladder Contouring AtlasDocument9 pagesBaumann 2016 IJROBP Development Validation of Bladder Contouring AtlaszanNo ratings yet
- A Pictorial Review of Postpartum ComplicationsDocument25 pagesA Pictorial Review of Postpartum ComplicationsGabriela Serra del CarpioNo ratings yet
- Actualizacion de Reporte de CA Colorectal 2019Document14 pagesActualizacion de Reporte de CA Colorectal 2019Jairo Lino BNo ratings yet
- The Solitary Pulmonary NoduleDocument11 pagesThe Solitary Pulmonary NoduleShahid HussainNo ratings yet
- Yale Observation Scale For Prediction of BacteremiaDocument7 pagesYale Observation Scale For Prediction of BacteremiaS Francisco MotNo ratings yet
- Medi 101 E28665Document5 pagesMedi 101 E28665S Francisco MotNo ratings yet
- JNM 19 251Document6 pagesJNM 19 251S Francisco MotNo ratings yet
- Natural Language Processing To Identify Pulmonary Nodules and Extract Nodule Characteristics From Radiology ReportsDocument13 pagesNatural Language Processing To Identify Pulmonary Nodules and Extract Nodule Characteristics From Radiology ReportsS Francisco MotNo ratings yet
- Adedapo 2020Document12 pagesAdedapo 2020S Francisco MotNo ratings yet
- Anxiety Disorders and Mood Disorders in Hospital Doctors: A Literature ReviewDocument9 pagesAnxiety Disorders and Mood Disorders in Hospital Doctors: A Literature ReviewS Francisco MotNo ratings yet
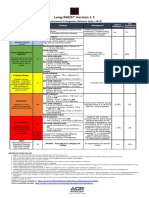
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Document1 pageLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNo ratings yet
- FaucifilesDocument302 pagesFaucifilesLady WellingtonNo ratings yet
- Clinical Practice Guidelines On Postmenopausal Osteoporosis: An Executive Summary and Recommendations - Update 2019-2020Document17 pagesClinical Practice Guidelines On Postmenopausal Osteoporosis: An Executive Summary and Recommendations - Update 2019-2020Marwa YassinNo ratings yet
- Studi Kasus Pada PT Damar Bandha Jaya Corp. BogorDocument10 pagesStudi Kasus Pada PT Damar Bandha Jaya Corp. BogorMayHan13No ratings yet
- Vivekananda's Role as Revivalist Reformer and His Ideas of Equality and Spiritual RevolutionDocument2 pagesVivekananda's Role as Revivalist Reformer and His Ideas of Equality and Spiritual RevolutionMartin VanlalhlimpuiaNo ratings yet
- Intersecting Lines Intersecting Lines Parallel Lines Same LineDocument7 pagesIntersecting Lines Intersecting Lines Parallel Lines Same Lineapi-438357152No ratings yet
- On The Art of Fighting - A Humanist Translation of Fiore Dei Liberi's Flower of Battle Owned by Leonello D'EsteDocument37 pagesOn The Art of Fighting - A Humanist Translation of Fiore Dei Liberi's Flower of Battle Owned by Leonello D'EsteHunterSJNo ratings yet
- 14 Ways To Acquire KnowledgeDocument4 pages14 Ways To Acquire KnowledgeRenato MiguelNo ratings yet
- EMAG W01 RodHeatingDocument16 pagesEMAG W01 RodHeatingMiguel Ángel ArizaNo ratings yet
- Dual Domain Image Encryption Using Bit Plane Scrambling and Sub - Band ScramblingDocument16 pagesDual Domain Image Encryption Using Bit Plane Scrambling and Sub - Band Scramblingraja rishyantNo ratings yet
- Presentation - On SVAMITVADocument18 pagesPresentation - On SVAMITVAPraveen PrajapatiNo ratings yet
- SEO-Optimized Title for Document on English Exam QuestionsDocument4 pagesSEO-Optimized Title for Document on English Exam Questionsminh buiNo ratings yet
- Google Wakeword Detection 1 PDFDocument5 pagesGoogle Wakeword Detection 1 PDFÖzgür Bora GevrekNo ratings yet
- 5.1 Advanced Pattern Making - IDocument9 pages5.1 Advanced Pattern Making - IRisul Islam EmonNo ratings yet
- Legal Documents Evidence in Safety Related Proceedings 1663086621Document9 pagesLegal Documents Evidence in Safety Related Proceedings 1663086621richardNo ratings yet
- English Team Agenda 2023-2024Document4 pagesEnglish Team Agenda 2023-2024api-604869051No ratings yet
- Gabriel MarcelDocument6 pagesGabriel MarcelCeciBohoNo ratings yet
- Review Relative Clauses, Articles, and ConditionalsDocument10 pagesReview Relative Clauses, Articles, and ConditionalsNgoc AnhNo ratings yet
- Consumers Guide To The ExpertsDocument406 pagesConsumers Guide To The ExpertsHassan Younhous Traore KonéNo ratings yet
- Class Xii Appendix-Iii: Colligative PropertiesDocument3 pagesClass Xii Appendix-Iii: Colligative PropertiesSrijan JaiswalNo ratings yet
- Kwame Ture InterviewDocument8 pagesKwame Ture InterviewSumayya K AliNo ratings yet
- Neurodegenerative Disorders of ChildhoodDocument51 pagesNeurodegenerative Disorders of ChildhoodPRONTO DIAGNOSTICNo ratings yet
- WRBS Quarter 1 Modules WEEK-1-8Document32 pagesWRBS Quarter 1 Modules WEEK-1-8Sir Kindred VillaruzNo ratings yet