You might also like
- Philips Mri Panorama ManualDocument6 pagesPhilips Mri Panorama ManualAbood Ali0% (1)
- Automatic 4D Flow MRI Segmentation Using The Standardized Difference of Means VelocityDocument14 pagesAutomatic 4D Flow MRI Segmentation Using The Standardized Difference of Means VelocityAngkon BiswasNo ratings yet
- A Rare Case of Space Occupying Lesion of Brainstem in An Elderly Male PatientDocument3 pagesA Rare Case of Space Occupying Lesion of Brainstem in An Elderly Male PatientInternational Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- Dacheng Jin 2020Document5 pagesDacheng Jin 2020Nehemias MD GuevaraNo ratings yet
- 1 Neurosurgery Cases and ReviewsDocument5 pages1 Neurosurgery Cases and ReviewsintodoieblissNo ratings yet
- Brain Imaging in Colloid CystDocument5 pagesBrain Imaging in Colloid CystMohamed Farouk El-FaresyNo ratings yet
- Medip, IJRMS-7729 ODocument7 pagesMedip, IJRMS-7729 ORagupathi MNo ratings yet
- Surgical Neurology International: Cordectomy For Intramedullary Spinal Cord Glioblastoma With A 12 Year SurvivalDocument5 pagesSurgical Neurology International: Cordectomy For Intramedullary Spinal Cord Glioblastoma With A 12 Year Survivallucasnegromonte0001No ratings yet
- Surgical Neurology International: Unusual Growth Pattern of A MeningiomaDocument3 pagesSurgical Neurology International: Unusual Growth Pattern of A MeningiomaJamie NicholsNo ratings yet
- International 2Document4 pagesInternational 2daffunkmadansyahNo ratings yet
- A Rare Case of A Giant Tumor of Sebaceous Glands in The Posterior Chest WallDocument7 pagesA Rare Case of A Giant Tumor of Sebaceous Glands in The Posterior Chest WallAthenaeum Scientific PublishersNo ratings yet
- Letters: Kumar S, Nair S, Alexander MDocument2 pagesLetters: Kumar S, Nair S, Alexander MAbubakar BashirNo ratings yet
- Ajns - AJNS 268 19Document4 pagesAjns - AJNS 268 19Elmo KrisnawanNo ratings yet
- Laminectomy Tumor Resection - Case ReportDocument8 pagesLaminectomy Tumor Resection - Case Reportshara rachmawatiNo ratings yet
- Cerebellar Hemangioblastoma-A Rare EntityDocument10 pagesCerebellar Hemangioblastoma-A Rare EntityJay LeheriNo ratings yet
- Tumefactive Demyelinating Lesions: Nine Cases and A Review of The LiteratureDocument9 pagesTumefactive Demyelinating Lesions: Nine Cases and A Review of The LiteraturePS NeuroNo ratings yet
- Hemangiopericytoma 05Document10 pagesHemangiopericytoma 05Tamajyoti GhoshNo ratings yet
- Primary Leiomyosarcoma of The Spine: An Analysis of Imaging Manifestations and Clinicopathological FindingsDocument9 pagesPrimary Leiomyosarcoma of The Spine: An Analysis of Imaging Manifestations and Clinicopathological Findingst7xs5mchfzNo ratings yet
- Magnetic Resonance Spectroscopy A Noninvasive Diagno - 2006 - Magnetic ResonancDocument3 pagesMagnetic Resonance Spectroscopy A Noninvasive Diagno - 2006 - Magnetic Resonanctejas1578No ratings yet
- SSP 1Document5 pagesSSP 1YanNo ratings yet
- Hon 2005Document2 pagesHon 2005Andana TrisaviNo ratings yet
- Idiopathic Cervical Spinal Subdural Haematoma: A Case Report and Literature ReviewDocument10 pagesIdiopathic Cervical Spinal Subdural Haematoma: A Case Report and Literature ReviewSelfa YunitaNo ratings yet
- Mature Cystic Teratoma of The Right Cerebellopontine Angle A Rare Case ReportDocument5 pagesMature Cystic Teratoma of The Right Cerebellopontine Angle A Rare Case ReportHaribabuBabuNo ratings yet
- An Uncommon Presentation of Early Brainstem High Gra 2024 International JourDocument7 pagesAn Uncommon Presentation of Early Brainstem High Gra 2024 International JourRonald QuezadaNo ratings yet
- Management of Orbital Rhabdomyosarcoma: About 2 Cases and Literature ReviewDocument7 pagesManagement of Orbital Rhabdomyosarcoma: About 2 Cases and Literature ReviewIJAR JOURNALNo ratings yet
- 264 2011 Article 1480Document6 pages264 2011 Article 1480Paul Mendez AguilarNo ratings yet
- Medial Orbital Epidermoid Cyst: Case ReportDocument3 pagesMedial Orbital Epidermoid Cyst: Case ReportTeodorNo ratings yet
- Chondrosarcoma of The Cervical Spine: C Ase ReportDocument3 pagesChondrosarcoma of The Cervical Spine: C Ase ReportChoirina Nur AzizaNo ratings yet
- 2021 Case Report Rare Case of Synchronous Neck Metastasis From Metachronous Bilateral Renal Cell CarcinomaDocument7 pages2021 Case Report Rare Case of Synchronous Neck Metastasis From Metachronous Bilateral Renal Cell CarcinomaAlfonsoSánchezNo ratings yet
- Solitary Bone Plasmacytoma of The Axis A Rare 2024 International Journal ofDocument5 pagesSolitary Bone Plasmacytoma of The Axis A Rare 2024 International Journal ofRonald QuezadaNo ratings yet
- Intraventricular GlioblastomaDocument3 pagesIntraventricular GlioblastomaArif Susilo RahadiNo ratings yet
- Pen TingDocument4 pagesPen TingLydia AmaliaNo ratings yet
- Cordom Clivus Case Report Plus Review 2017Document6 pagesCordom Clivus Case Report Plus Review 2017Ionela DumitriuNo ratings yet
- SM Pediatric Balolike 10072 - 2022 - Article - 6396Document3 pagesSM Pediatric Balolike 10072 - 2022 - Article - 6396Tunde CsepanyNo ratings yet
- J Surneu 2007 07 059Document4 pagesJ Surneu 2007 07 059lucasnegromonte0001No ratings yet
- Brain-Sparing Radiotherapy For Neuroblastoma Skull MetastasesDocument6 pagesBrain-Sparing Radiotherapy For Neuroblastoma Skull Metastasesasialoren74No ratings yet
- Cerebral Venous Thrombosis: A Comprehensive Review: Clinical Neurology: Review ArticleDocument11 pagesCerebral Venous Thrombosis: A Comprehensive Review: Clinical Neurology: Review Articledanby danbyNo ratings yet
- Unusual Brain StoneDocument5 pagesUnusual Brain StonekucingNo ratings yet
- Spinal Cord EnhancementDocument3 pagesSpinal Cord EnhancementGabriel PinillaNo ratings yet
- Jurnal Radiologi 1Document9 pagesJurnal Radiologi 1Nia RwNo ratings yet
- Diffusion-Weighted Imaging in The Follow-Up of Treated High-Grade Gliomas: Tumor Recurrence Versus Radiation InjuryDocument9 pagesDiffusion-Weighted Imaging in The Follow-Up of Treated High-Grade Gliomas: Tumor Recurrence Versus Radiation InjuryJheny LopezNo ratings yet
- JAMA - A Child With A White Pupil (Retinoblastoma)Document2 pagesJAMA - A Child With A White Pupil (Retinoblastoma)Rafael Carrillo-BaylonNo ratings yet
- Point: How Do I Manage A Suspected Oral Vascular Malformation?Document3 pagesPoint: How Do I Manage A Suspected Oral Vascular Malformation?Luis Mesicano QuipeNo ratings yet
- A Case Report of Chest Wall Desmoplastic Sma - 2024 - International Journal of SDocument4 pagesA Case Report of Chest Wall Desmoplastic Sma - 2024 - International Journal of SRonald QuezadaNo ratings yet
- Jurnal Bedah AnakDocument3 pagesJurnal Bedah AnakAstari ArumNo ratings yet
- Medi 98 E18430Document2 pagesMedi 98 E18430Anonymous tG35SYROzENo ratings yet
- Follow UpDocument6 pagesFollow UpWinda HaeriyokoNo ratings yet
- Ctoij MS Id 555925Document8 pagesCtoij MS Id 555925lucasnegromonte0001No ratings yet
- Imaging Patterns of Cardiac MRI in The Diagnosis of MyocarditisDocument10 pagesImaging Patterns of Cardiac MRI in The Diagnosis of MyocarditisvijuNo ratings yet
- Brainstem CysticercoseDocument4 pagesBrainstem CysticercoseDr. R. SANKAR CITNo ratings yet
- CE (Ra1) F (GH) PF1 (ANAK) PFA (AK) PF2 (PAG)Document2 pagesCE (Ra1) F (GH) PF1 (ANAK) PFA (AK) PF2 (PAG)Diana CantúNo ratings yet
- Follicular Carcinoma of Thyroid Presenting As Brain MetastasisDocument3 pagesFollicular Carcinoma of Thyroid Presenting As Brain MetastasisArif Susilo RahadiNo ratings yet
- Laryngeal Plasmacytoma in Kahlers Disease: A Case ReportDocument6 pagesLaryngeal Plasmacytoma in Kahlers Disease: A Case ReportIJAR JOURNALNo ratings yet
- Central Giant Cell Granuloma of The Head & Neck: A Case Report and Systematic ReviewDocument8 pagesCentral Giant Cell Granuloma of The Head & Neck: A Case Report and Systematic ReviewKarol Y. Wilson LondoñoNo ratings yet
- Imaging Findings of Intraventricular and Ependymal LesionsDocument16 pagesImaging Findings of Intraventricular and Ependymal Lesionsanggi abNo ratings yet
- Cpho 29 2 97Document5 pagesCpho 29 2 97Kyung-Nam KohNo ratings yet
- Kbbi 18 5 326 329Document4 pagesKbbi 18 5 326 329nursengNo ratings yet
- Tonsil TumorDocument4 pagesTonsil TumorafrisiammyNo ratings yet
- Late Recurrence of A Brain Tumor: Michael N. Needle,, Lucy B. Rorke,, and Peter WinklerDocument5 pagesLate Recurrence of A Brain Tumor: Michael N. Needle,, Lucy B. Rorke,, and Peter WinklerantonioopNo ratings yet
- A Child With Acute Eyelid Edema and Proptosis: JAMA Ophthalmology Clinical ChallengeDocument2 pagesA Child With Acute Eyelid Edema and Proptosis: JAMA Ophthalmology Clinical ChallengePatriciaNo ratings yet
- Imaging in Brain TumorDocument142 pagesImaging in Brain TumorMagrinov AzaniaNo ratings yet
- Fast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseFrom EverandFast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseNo ratings yet
- Kumbhar 2016Document13 pagesKumbhar 2016S Francisco MotNo ratings yet
- Yale Observation Scale For Prediction of BacteremiaDocument7 pagesYale Observation Scale For Prediction of BacteremiaS Francisco MotNo ratings yet
- JNM 19 251Document6 pagesJNM 19 251S Francisco MotNo ratings yet
- Natural Language Processing To Identify Pulmonary Nodules and Extract Nodule Characteristics From Radiology ReportsDocument13 pagesNatural Language Processing To Identify Pulmonary Nodules and Extract Nodule Characteristics From Radiology ReportsS Francisco MotNo ratings yet
- Adedapo 2020Document12 pagesAdedapo 2020S Francisco MotNo ratings yet
- Anxiety Disorders and Mood Disorders in Hospital Doctors: A Literature ReviewDocument9 pagesAnxiety Disorders and Mood Disorders in Hospital Doctors: A Literature ReviewS Francisco MotNo ratings yet
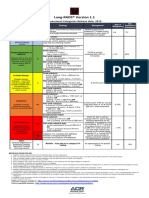
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Document1 pageLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNo ratings yet
- The Highest Field Strength Open MriDocument10 pagesThe Highest Field Strength Open MriOmarNo ratings yet
- Anaesthesia Outside The Operating Theatre Update 2010Document5 pagesAnaesthesia Outside The Operating Theatre Update 2010Marcella AmadeaNo ratings yet
- Guia Marco TeoricoDocument16 pagesGuia Marco Teoricoarlin AiraNo ratings yet
- Wiley Journal APCs Open AccessDocument216 pagesWiley Journal APCs Open AccessLupi YudhaningrumNo ratings yet
- Evaluating Cardiomegaly by Radiological Cardiothoracic Ratio As Compared To Conventional EchocardiographyDocument3 pagesEvaluating Cardiomegaly by Radiological Cardiothoracic Ratio As Compared To Conventional EchocardiographyputriNo ratings yet
- Va Mri Design Plan Drawings and LayoutDocument19 pagesVa Mri Design Plan Drawings and Layoutkusnanto erinNo ratings yet
- To Reduce The Waiting Time at Radiology Department (CT, MRI, X-RAY)Document12 pagesTo Reduce The Waiting Time at Radiology Department (CT, MRI, X-RAY)kaashvi dubeyNo ratings yet
- Properties of Ferromagnetic Materials PDFDocument9 pagesProperties of Ferromagnetic Materials PDFSäjidëë KisÅnNo ratings yet
- Tumor Celulas GigantesDocument7 pagesTumor Celulas GigantesGabyNo ratings yet
- PAPIMI SPORTS ReportDocument61 pagesPAPIMI SPORTS ReportLaurent SchidlerNo ratings yet
- X Ray L InterpretationDocument33 pagesX Ray L InterpretationBajwala ViralNo ratings yet
- An Approach For Three-Dimensional Visualization Using High-Resolution MRI of The Temporomandibular JointDocument7 pagesAn Approach For Three-Dimensional Visualization Using High-Resolution MRI of The Temporomandibular JointПавло БурлаковNo ratings yet
- The Amazing BrainDocument13 pagesThe Amazing BrainhaveanicedayNo ratings yet
- Tuberculous Meningitis: Neurological Aspects of Tropical DiseaseDocument11 pagesTuberculous Meningitis: Neurological Aspects of Tropical DiseaseSanti IsmatulNo ratings yet
- Hemorragia SubaracnoideaDocument18 pagesHemorragia SubaracnoideaResidencia NeurologíaNo ratings yet
- Mri XyzDocument26 pagesMri Xyzwisesoar100% (1)
- AXA PPP HandbookDocument40 pagesAXA PPP Handbookcamsy83No ratings yet
- The Essential Guide To Brain Tumors PDFDocument43 pagesThe Essential Guide To Brain Tumors PDFA Farid WajdyNo ratings yet
- SternMed Marcom 0.35T LeafletDocument8 pagesSternMed Marcom 0.35T LeafletQCNo ratings yet
- Carcinoma Rectum - Janak - NEWDocument74 pagesCarcinoma Rectum - Janak - NEWTowhidulIslamNo ratings yet
- Prostate Biopsy - UpToDateDocument47 pagesProstate Biopsy - UpToDateCésar Aguirre RomeroNo ratings yet
- Salter Harris Classification of Growth Plate FracturesDocument13 pagesSalter Harris Classification of Growth Plate FracturesAarón E. CaríasNo ratings yet
- Ece Thesis NG Kuya KoDocument61 pagesEce Thesis NG Kuya KoRouel LeonenNo ratings yet
- Abbreviations For O&G IndustryDocument38 pagesAbbreviations For O&G IndustryMike George MeyerNo ratings yet
- EstudioDocument30 pagesEstudioSonia QuicenoNo ratings yet
- MR Obstetric PelvimetryDocument5 pagesMR Obstetric PelvimetrySreekanth RaveendranNo ratings yet
- Fusion of The Lumbar Spine. A Consideration of The IndicationsDocument12 pagesFusion of The Lumbar Spine. A Consideration of The IndicationsCristina Galvez PerezNo ratings yet
- AGLLSS - Day1 - Preoperative Preparation For Gynecologic Surgery - DR GatotDocument15 pagesAGLLSS - Day1 - Preoperative Preparation For Gynecologic Surgery - DR GatotherryNo ratings yet