You might also like
- Serologic Responses To Sars-Cov-2 Infection Among Hospital Staff With Mild Disease in Eastern FranceDocument21 pagesSerologic Responses To Sars-Cov-2 Infection Among Hospital Staff With Mild Disease in Eastern FranceAssia AouachriaNo ratings yet
- 2020 04 18 20071134v1 FullDocument22 pages2020 04 18 20071134v1 Fulld.amouzou1965No ratings yet
- Diagnosis of SARS-CoV-2 in Children - Accuracy of Nasopharyngeal Swab Compared To Nasopharyngeal AspirateDocument15 pagesDiagnosis of SARS-CoV-2 in Children - Accuracy of Nasopharyngeal Swab Compared To Nasopharyngeal Aspiraterivia ginaNo ratings yet
- s13063 021 05329 yDocument2 pagess13063 021 05329 ymeth holaNo ratings yet
- Use of Antivirals and Antibiotics For COVID-19 in Mexico City: A Real-World Multicenter Cohort StudyDocument38 pagesUse of Antivirals and Antibiotics For COVID-19 in Mexico City: A Real-World Multicenter Cohort StudyutariNo ratings yet
- Artic - Covid 19Document19 pagesArtic - Covid 19cristinaNo ratings yet
- High Transmissibility of COVID-19 Near Symptom Onset: Hsienho@ntu - Edu.twDocument19 pagesHigh Transmissibility of COVID-19 Near Symptom Onset: Hsienho@ntu - Edu.twGABYNo ratings yet
- Impaired Type I Interferon Activity and Exacerbated Inflammatory Responses in Severe Covid-19 PatientsDocument31 pagesImpaired Type I Interferon Activity and Exacerbated Inflammatory Responses in Severe Covid-19 PatientsSusana PaçoNo ratings yet
- Factors Associated With Severe Sars-Cov-2 Infection: BackgroundDocument14 pagesFactors Associated With Severe Sars-Cov-2 Infection: BackgroundmikoNo ratings yet
- 2020 02 11 20021493v2 FullDocument17 pages2020 02 11 20021493v2 FullRogelio MoscosoNo ratings yet
- D1 PDFDocument26 pagesD1 PDFpopov357No ratings yet
- Pre-Symptomatic Transmission of Sars-Cov-2 Infection: A Secondary Analysis Using Published DataDocument34 pagesPre-Symptomatic Transmission of Sars-Cov-2 Infection: A Secondary Analysis Using Published DataFatrina Maha DewiNo ratings yet
- Systematic Review of The Association Between Rotavirus Infection, or Rotavirus Vaccination and Coeliac DiseaseDocument18 pagesSystematic Review of The Association Between Rotavirus Infection, or Rotavirus Vaccination and Coeliac Diseasepopov357No ratings yet
- Novel Coronavirus COVID-19 Knowledge and PerceptioDocument16 pagesNovel Coronavirus COVID-19 Knowledge and Perceptiotiglu nanoNo ratings yet
- Journal Pre-Proof: International Journal of Infectious DiseasesDocument27 pagesJournal Pre-Proof: International Journal of Infectious DiseasesMohammed Shuaib AhmedNo ratings yet
- Ferritin Procalcitonin Ratio in Covid and Bacterial PneumoniaDocument20 pagesFerritin Procalcitonin Ratio in Covid and Bacterial PneumoniaYoutube MaliaNo ratings yet
- Epidemiology and Transmission of COVID-19 in Shenzhen China: Analysis of 391 Cases and 1,286 of Their Close ContactsDocument22 pagesEpidemiology and Transmission of COVID-19 in Shenzhen China: Analysis of 391 Cases and 1,286 of Their Close ContactsVictor Ricardo Ruiz LlamasNo ratings yet
- Title: Seroprevalence of Anti-Sars-Cov-2 Antibodies in Iquitos, Loreto, PeruDocument20 pagesTitle: Seroprevalence of Anti-Sars-Cov-2 Antibodies in Iquitos, Loreto, PeruCésar LópezNo ratings yet
- 11) Jurnal LR Full (Bhagavathula)Document15 pages11) Jurnal LR Full (Bhagavathula)Mastifa HanasitaNo ratings yet
- Abdomen AgudoDocument30 pagesAbdomen AgudoJuan HernandezNo ratings yet
- COVID-19 Testing: A Reflection On Test Accuracy in The Real WorldDocument34 pagesCOVID-19 Testing: A Reflection On Test Accuracy in The Real Worldjoeboots78No ratings yet
- 2020 12 21 20248640v1 FullDocument19 pages2020 12 21 20248640v1 Fulla sangNo ratings yet
- Analytical Performance of COVID-19 Detection Methods (RT-PCR) : Scientific and Societal ConcernsDocument16 pagesAnalytical Performance of COVID-19 Detection Methods (RT-PCR) : Scientific and Societal ConcernsFre mobileNo ratings yet
- The Impact of High Frequency Rapid Viral Antigen Screening On COVID-19 Spread and Outcomes: A Validation and Modeling StudyDocument41 pagesThe Impact of High Frequency Rapid Viral Antigen Screening On COVID-19 Spread and Outcomes: A Validation and Modeling StudyJuensNo ratings yet
- Trends in Social Exposure To SARS-Cov-2 in FranceDocument16 pagesTrends in Social Exposure To SARS-Cov-2 in FrancevicqyoanNo ratings yet
- Ijma 9 408Document3 pagesIjma 9 408agil ferdiansyahNo ratings yet
- Current Understanding of COVID-19 Clinical Course and Investigational TreatmentsDocument26 pagesCurrent Understanding of COVID-19 Clinical Course and Investigational TreatmentsCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- A Deep Learning Algorithm Using CT Images To Screen For Corona Virus Disease (COVID-19)Document19 pagesA Deep Learning Algorithm Using CT Images To Screen For Corona Virus Disease (COVID-19)Hesbon MomanyiNo ratings yet
- Asselah 2020Document42 pagesAsselah 2020ENRICO 102011216No ratings yet
- COVID 19 en UCIP Paises de Recursos Limitados. DR Carcillo. Pediatric Research 2020 Muy BuenaDocument12 pagesCOVID 19 en UCIP Paises de Recursos Limitados. DR Carcillo. Pediatric Research 2020 Muy BuenaDark LouNo ratings yet
- Viable SARS-CoV-2 in The Air of A Hospital Room With COVID-19 Patients - J A Lednicky Et Al - 2020Document20 pagesViable SARS-CoV-2 in The Air of A Hospital Room With COVID-19 Patients - J A Lednicky Et Al - 2020Guto ClipesNo ratings yet
- Research Paper On Dengue VirusDocument6 pagesResearch Paper On Dengue Virusfvgy6fn3100% (1)
- Vaccines For Corona Virus Project-1Document28 pagesVaccines For Corona Virus Project-1Ananya PuhanNo ratings yet
- D3 PDFDocument24 pagesD3 PDFpopov357No ratings yet
- Estudio 2 PDFDocument28 pagesEstudio 2 PDFCr A AleydaNo ratings yet
- 2020 04 24 20078782v1 FullDocument41 pages2020 04 24 20078782v1 FullAbay SisayNo ratings yet
- Incidence and Severity of COVID-19 With The Use of The MMRDocument27 pagesIncidence and Severity of COVID-19 With The Use of The MMRGaspar PonceNo ratings yet
- 8d9c PDFDocument11 pages8d9c PDFJulian AshbourneNo ratings yet
- LeptospirosisDocument8 pagesLeptospirosisSanda Puspa RiniNo ratings yet
- Assessment of COVID-19 Vaccine Acceptance Among Healthcare Workers in Los AngelesDocument23 pagesAssessment of COVID-19 Vaccine Acceptance Among Healthcare Workers in Los AngelesSnega KaranNo ratings yet
- Is There A Connection Between Coronavirus, Wuhan-China, Marseille, Lyon-France and P4 LaboratoriesDocument69 pagesIs There A Connection Between Coronavirus, Wuhan-China, Marseille, Lyon-France and P4 LaboratoriesCucu Catalin100% (2)
- Title: Early Transmission Dynamics, Spread, and Genomic Characterization of Sars-Cov-2 in PanamaDocument14 pagesTitle: Early Transmission Dynamics, Spread, and Genomic Characterization of Sars-Cov-2 in PanamaCarlos de ObladiaNo ratings yet
- Knowledge, Attitudes, and Practices (KAP) of Healthcare Workers On Viral Hepatitis B and Its Vaccination in 12 Health Establishments in The Centre Region of CameroonDocument8 pagesKnowledge, Attitudes, and Practices (KAP) of Healthcare Workers On Viral Hepatitis B and Its Vaccination in 12 Health Establishments in The Centre Region of CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Antibody Tests in Detecting SARS-CoV-2 MetanalisisDocument18 pagesAntibody Tests in Detecting SARS-CoV-2 MetanalisisRenato DesideriNo ratings yet
- Challenges in Laboratory Diagnosis of The NovelDocument27 pagesChallenges in Laboratory Diagnosis of The NovelRidho Al Fiqri100% (1)
- False-Negative Results of Initial RT-PCR Assays For COVID-19: A Systematic ReviewDocument19 pagesFalse-Negative Results of Initial RT-PCR Assays For COVID-19: A Systematic ReviewFre mobileNo ratings yet
- Artigo Cientifico EpidemiologiaDocument10 pagesArtigo Cientifico Epidemiologiaroooberta3No ratings yet
- Deal The PandemicDocument55 pagesDeal The PandemicDebabrata SahaNo ratings yet
- PESQUISA FIOCRUZ COVID - 2020.04.04.020925v2.fullDocument28 pagesPESQUISA FIOCRUZ COVID - 2020.04.04.020925v2.fullMaressa OmenaNo ratings yet
- Effective Contact Tracing For COVID-19: A Systematic Review: Carl-Etienne - Juneau@umontreal - CaDocument25 pagesEffective Contact Tracing For COVID-19: A Systematic Review: Carl-Etienne - Juneau@umontreal - Capopov357No ratings yet
- Knowledge and Perceptions of COVID-19 Among Government Employees in EthiopiaDocument31 pagesKnowledge and Perceptions of COVID-19 Among Government Employees in EthiopiaRedaksi RelawanNo ratings yet
- Title: Coronavirus Disease 2019 (COVID-19) During Pregnancy: A Case SeriesDocument28 pagesTitle: Coronavirus Disease 2019 (COVID-19) During Pregnancy: A Case Seriesbrenda elielNo ratings yet
- Lancet 2023Document17 pagesLancet 2023Julia Urquiza LandaluceNo ratings yet
- English ProjectDocument18 pagesEnglish ProjectSHADOW BOYNo ratings yet
- 2020 11 09 20228098v1 FullDocument35 pages2020 11 09 20228098v1 FullmisdeismoNo ratings yet
- Jurnal Kampen 2020Document29 pagesJurnal Kampen 2020Crosco BDLNo ratings yet
- Recent Advances in The Development and Evaluation of Molecular Diagnostics For Evola Virus DiseaseDocument30 pagesRecent Advances in The Development and Evaluation of Molecular Diagnostics For Evola Virus DiseaseWendi IochNo ratings yet
- Laboratory Abnormalities in Patients With COVID-2019 InfectionDocument5 pagesLaboratory Abnormalities in Patients With COVID-2019 InfectionIsrael Parra-OrtegaNo ratings yet
- Laboratory Abnormalities in Patients With COVID-2019 InfectionDocument5 pagesLaboratory Abnormalities in Patients With COVID-2019 InfectionIsrael Parra-OrtegaNo ratings yet
- Skin and Arthropod VectorsFrom EverandSkin and Arthropod VectorsNathalie BoulangerNo ratings yet
- School Based Information and Education Campaign ProgramDocument13 pagesSchool Based Information and Education Campaign ProgramBarangay MotibotNo ratings yet
- Risk Communication For Public Health EmergenciesDocument25 pagesRisk Communication For Public Health EmergenciesBarangay MotibotNo ratings yet
- Household Transmission of SARS-CoV-2 in The United StatesDocument25 pagesHousehold Transmission of SARS-CoV-2 in The United StatesBarangay MotibotNo ratings yet
- Resurgence of SARS-CoV-2 Detection by Community Viral SurveillanceDocument6 pagesResurgence of SARS-CoV-2 Detection by Community Viral SurveillanceBarangay MotibotNo ratings yet
- Measuring Indonesia HN Pandemic Preparedness Through Stakeholder Analysis - hccr.1000119Document6 pagesMeasuring Indonesia HN Pandemic Preparedness Through Stakeholder Analysis - hccr.1000119Barangay MotibotNo ratings yet
- Reaching Out To The Millions-A 5 Key MessagesDocument5 pagesReaching Out To The Millions-A 5 Key MessagesBarangay MotibotNo ratings yet
- Perceived Sufficiency and Usefulness of IEC Materials and Methods Related To HIVAIDS Among High School Youth in Addis Ababa, EthiopiaDocument13 pagesPerceived Sufficiency and Usefulness of IEC Materials and Methods Related To HIVAIDS Among High School Youth in Addis Ababa, EthiopiaBarangay MotibotNo ratings yet
- Knowledge and Hand Hygiene Practice of Healthcare Workers inDocument11 pagesKnowledge and Hand Hygiene Practice of Healthcare Workers inBarangay MotibotNo ratings yet
- Instructional Interventions For Improving COVID-19 Knowledge, AttitudesDocument6 pagesInstructional Interventions For Improving COVID-19 Knowledge, AttitudesBarangay MotibotNo ratings yet
- Prospects and Challenges For Traditional Leaders in Combating COVID-19 Pandemic in Rural ZimbabweDocument16 pagesProspects and Challenges For Traditional Leaders in Combating COVID-19 Pandemic in Rural ZimbabweBarangay MotibotNo ratings yet
- Impact of A Playful Booklet About Diabetes and Obesity On High School Students in Campinas, BrazilDocument4 pagesImpact of A Playful Booklet About Diabetes and Obesity On High School Students in Campinas, BrazilBarangay MotibotNo ratings yet
- Seroprevalence of SARS-CoV-2 Antibodies in Children and Adults in St. Louis, Missouri, USADocument7 pagesSeroprevalence of SARS-CoV-2 Antibodies in Children and Adults in St. Louis, Missouri, USABarangay MotibotNo ratings yet
- On The Effect of Age On The Transmission of SARS-CoV-2 in Households, Schools and The CommunitDocument16 pagesOn The Effect of Age On The Transmission of SARS-CoV-2 in Households, Schools and The CommunitBarangay MotibotNo ratings yet
- Estimated Incidence of COVID-19 Illness and Hospitalization United States, February-Sep 2020Document32 pagesEstimated Incidence of COVID-19 Illness and Hospitalization United States, February-Sep 2020Barangay MotibotNo ratings yet
- Social Determinants of Health The Role of Effective Communication in The COVID-19 Pandemic in Developing CountriesDocument5 pagesSocial Determinants of Health The Role of Effective Communication in The COVID-19 Pandemic in Developing CountriesBarangay MotibotNo ratings yet
- Use of Information, Education and CommunicationDocument6 pagesUse of Information, Education and CommunicationBarangay MotibotNo ratings yet
- The Role of Children in The Dynamics of Intra Family Coronavirus 2019 Spread in Densely Populated AreaDocument3 pagesThe Role of Children in The Dynamics of Intra Family Coronavirus 2019 Spread in Densely Populated AreaBarangay MotibotNo ratings yet
- Effectiveness of Patient Education in Acute Stroke A Comparison Between A Customised Computer System and A Pictorial Information BookletDocument7 pagesEffectiveness of Patient Education in Acute Stroke A Comparison Between A Customised Computer System and A Pictorial Information BookletBarangay MotibotNo ratings yet
- Transmission of SARS-COV-2 Infections in Households Tennessee and Wisconsin, April-Sep 2020Document4 pagesTransmission of SARS-COV-2 Infections in Households Tennessee and Wisconsin, April-Sep 2020Barangay MotibotNo ratings yet
- A Meta-Analysis On The Role of Children in SARS-CoV-2 in Household TransmissionDocument25 pagesA Meta-Analysis On The Role of Children in SARS-CoV-2 in Household TransmissionBarangay MotibotNo ratings yet
- The Information-Seeking Behavior and Levels of Knowledge, Precaution, and Fear of College Students in Iloilo, Philippines Amidst The COVID-19 PandemicDocument15 pagesThe Information-Seeking Behavior and Levels of Knowledge, Precaution, and Fear of College Students in Iloilo, Philippines Amidst The COVID-19 PandemicBarangay MotibotNo ratings yet
- FEQ3R212QLFGNKA4HODocument9 pagesFEQ3R212QLFGNKA4HOBarangay MotibotNo ratings yet
- 2965 CONSORT+2010+ChecklistDocument2 pages2965 CONSORT+2010+ChecklistsongsiriNo ratings yet
- Excitation of Skeletal Muscle: Neuromuscular Transmission and Excitation-Contraction CouplingDocument14 pagesExcitation of Skeletal Muscle: Neuromuscular Transmission and Excitation-Contraction CouplingBarangay MotibotNo ratings yet
- Book ReportDocument69 pagesBook ReportBarangay MotibotNo ratings yet
- Discordant GrowthDocument20 pagesDiscordant GrowthBarangay MotibotNo ratings yet
- Del Um PinesDocument1 pageDel Um PinesBarangay MotibotNo ratings yet
- Book ReportDocument20 pagesBook ReportBarangay MotibotNo ratings yet
- Herpes Zoster Diagnostic Therapeutic and Preventive ApproachesDocument15 pagesHerpes Zoster Diagnostic Therapeutic and Preventive ApproacheswulanNo ratings yet
- Common ColdDocument8 pagesCommon Coldvaschuk_8No ratings yet
- An Analysis of Taiwan's Vaccination Services and Applications For Vaccine Injury CompensationsDocument15 pagesAn Analysis of Taiwan's Vaccination Services and Applications For Vaccine Injury CompensationsAnonymous FNZ3uR2AHsNo ratings yet
- Acne VulgarisDocument58 pagesAcne VulgarisNargisNo ratings yet
- Management of Stevens-Johnson Syndrome and Toxic Epidermal NecrolysisDocument3 pagesManagement of Stevens-Johnson Syndrome and Toxic Epidermal NecrolysisWinda AlpiniawatiNo ratings yet
- Lap Pelayanan SeptemberDocument12 pagesLap Pelayanan SeptemberJosepb SimarmataNo ratings yet
- EPALS DKA Flowchart Jan 23 V4Document1 pageEPALS DKA Flowchart Jan 23 V4Miguel BaiaNo ratings yet
- Taking A History NotesDocument3 pagesTaking A History NotesMarkNo ratings yet
- Acute Necrotizing Ulcerative GingivitisDocument5 pagesAcute Necrotizing Ulcerative GingivitisVictor GiraldezNo ratings yet
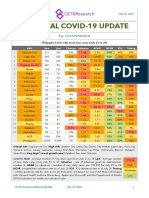
- National COVID-19 Update by Octa Research On July 30, 2021Document2 pagesNational COVID-19 Update by Octa Research On July 30, 2021RapplerNo ratings yet
- Typhoid Fever Final 2Document28 pagesTyphoid Fever Final 2gAARaNo ratings yet
- Clinical Reasoning, Assessment, and RecordingDocument19 pagesClinical Reasoning, Assessment, and RecordingChristyl JoNo ratings yet
- Tdap VaccinationDocument3 pagesTdap VaccinationDark AghanimNo ratings yet
- Major Case StudyDocument29 pagesMajor Case Studyapi-490093193No ratings yet
- Medical History Report Medical Prescreen Questionnaire: Philippine National Police Health ServiceDocument4 pagesMedical History Report Medical Prescreen Questionnaire: Philippine National Police Health ServicejovelonderizaNo ratings yet
- Methodology Series Module 1 Cohort StudiesDocument5 pagesMethodology Series Module 1 Cohort StudiesRaa ShaviraaNo ratings yet
- Approach To PCM CasesDocument310 pagesApproach To PCM CasesgjdbfiuvaNo ratings yet
- Treatment of Minor AilmentsDocument43 pagesTreatment of Minor AilmentsVidhya RaniNo ratings yet
- Basics of Scientific Writing, Scientific Research, and Elementary Data AnalysisDocument12 pagesBasics of Scientific Writing, Scientific Research, and Elementary Data Analysisburhan sabirNo ratings yet
- Formula of Vital Health IndicatorsDocument3 pagesFormula of Vital Health IndicatorsZyntrx Villas100% (1)
- Epidemiology of Alzheimer DiseaseDocument17 pagesEpidemiology of Alzheimer DiseaseAndi SulvanNo ratings yet
- Immune Tolerance and Slow-Virus Disease: Skeletons in The Closet of Western Science & Public Health, by A. W. FinneganDocument38 pagesImmune Tolerance and Slow-Virus Disease: Skeletons in The Closet of Western Science & Public Health, by A. W. FinneganOperation OpenscriptNo ratings yet
- Oxfordshire ADULT Antimicrobial Prescribing Guidelines For Primary CareDocument21 pagesOxfordshire ADULT Antimicrobial Prescribing Guidelines For Primary CareDan IonescuNo ratings yet
- Class IX Science Why Do We Fall Ill PPT Module 1 - 3Document16 pagesClass IX Science Why Do We Fall Ill PPT Module 1 - 3Shailaja Mestry50% (2)
- Disaster Triage Forgotten Lessons in Pandemic Covid-19 Management - Dr. Yogi Prabowo, SpOT (K)Document23 pagesDisaster Triage Forgotten Lessons in Pandemic Covid-19 Management - Dr. Yogi Prabowo, SpOT (K)Clara EverlastNo ratings yet
- Hepatites A, B, CDocument22 pagesHepatites A, B, CsanthiagoschneiderNo ratings yet
- The Health Benefits of Exercise in Overweight and Obese PatientsDocument5 pagesThe Health Benefits of Exercise in Overweight and Obese Patientspb.nakulaNo ratings yet
- Multiple Organ Dysfunction SyndromeDocument2 pagesMultiple Organ Dysfunction SyndromeMaryjoy Gabriellee De La CruzNo ratings yet
- Complicated MeaslesDocument13 pagesComplicated MeaslesFarica Armane AquinoNo ratings yet
- Speci C Protein Analysis System: DiagnosticsDocument2 pagesSpeci C Protein Analysis System: DiagnosticsAniket dubeyNo ratings yet