Professional Documents
Culture Documents
Using Rasch Analysis To Revisit The Vali
Uploaded by
pallavi patilOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Using Rasch Analysis To Revisit The Vali
Uploaded by
pallavi patilCopyright:
Available Formats
ARTICLE
Using Rasch analysis to revisit the validity
of the Cataract TyPE Spec instrument
for measuring cataract surgery outcomes
Vijaya K. Gothwal, PhD, Thomas A. Wright, Ecosse L. Lamoureux, PhD, Konrad Pesudovs, PhD
PURPOSE: To assess the psychometric properties of the Cataract TyPE Specification (Spec)
questionnaire using the Rasch model.
SETTING: Flinders Medical Centre, Adelaide, Australia.
METHODS: The 12-item Cataract TyPE Spec questionnaire was self-administered to patients drawn
from the cataract surgery waiting list. The questionnaire and its 5 subscales were assessed for fit to
the Rasch model. Response category performance, item-fit targeting, unidimensionality (using
principal components analysis), and differential item functioning were assessed. A shortened ver-
sion (11 items) was tested for criterion validity by determining correlation with a global rating of
vision question.
RESULTS: Two hundred ninety-four patients responded to the questionnaire. The response
categories for each question functioned as intended. Person-separation reliability was high
(0.90). Deletion of 1 misfitting item (nighttime driving) improved overall model fit. The principal
components analysis of the residuals demonstrated unidimensionality for the 11-item Cataract
TyPE Spec and 2 subscales. However, items were targeted to a less able population. Only 2
subscales (near vision and glare) were valid. There was a good statistically significant correlation
between the Likert-scored global rating of vision and the Rasch-scaled Cataract TyPE Spec score
(r Z 0.66, P<.0001), suggesting good criterion validity.
CONCLUSIONS: With minor modifications, the Cataract TyPE Spec questionnaire and its glare and
near-vision subscales were good measures of visual functioning in the cataract patient. Additional
items to suit the more able, including patients having second-eye surgery, could improve the mea-
surement properties.
J Cataract Refract Surg 2009; 35:1509–1517 Q 2009 ASCRS and ESCRS
Cataract is the leading cause of treatable blindness in the scales are equal over the full range of the scale
the world, and cataract surgery is expected to increase and the scale is erroneously treated as an interval scale
with the aging population.1 It is the most commonly based on the ordinal level of scoring.12,13 More re-
performed procedure in Australia.2,3 cently, modern psychometric approaches have been
The need to include patient-reported outcomes (or adopted such as the Rasch measurement models.14–16
questionnaires) in the assessment of cataract surgery Rasch analysis provides unparalleled insight into con-
is now widely appreciated.4–6 Several questionnaires tent validity and targeting of item difficulty to patient
developed for this purpose, such as the Activities of ability, not possible with classical test theory.17,18 Al-
Daily Vision Scale (ADVS),7,8 Visual Disability Assess- though none of the aforementioned questionnaires
ment (VDA),9 Visual Function 14 (VF-14),10 Cat- (ADVS, VDA, VF-14, Catquest) have been developed
quest,11 and Cataract TyPE Specification (TyPE using Rasch Analysis, they have been tested and reva-
Spec),12,13 have used the traditional psychometric ap- lidated using Rasch analysis (Pesudovs K, et al. IOVS
proach; that is the classical test theory. However there 2005; 46:ARVO E-Abstract 3844. Available at: http://
are 2 important limitations of classical test theory: the abstracts.iovs.org/cgi/content/abstract/46/5/3844.
validity of the scoring method and the validity of the Accessed May 24, 2009).19–21
items included. The scoring problem of classical test The Cataract TyPE Spec is a reliable and valid scale, by
theory arises from the assumption that distances on classical test theory, for measuring vision-related
Q 2009 ASCRS and ESCRS 0886-3350/09/$dsee front matter 1509
Published by Elsevier Inc. doi:10.1016/j.jcrs.2009.03.056
1510 RASCH ANALYSIS: VALIDITY OF THE CATARACT TYPE SPEC INSTRUMENT
function and outcomes of cataract extraction.12,13 In There are also questions about other characteristics, such
view of the limitations of the classic test theory, we as recent illness, injury, or emotional upset, and the help re-
quired (if any) to fill out the questionnaire. These latter ques-
sought to use Rasch analysis to revalidate the Cataract
tions were meant to be used as demographic variables, not to
TyPE Spec instrument in an Australian cataract popula- evaluate the benefits of cataract surgery. Therefore, these
tion waiting to have cataract extraction. This included, if questions were not included in the analysis.
necessary, making revisions to the content of the instru-
ment to improve its validity. However, the main aim Patients
was to use Rasch analysis to estimate linear interval mea- Patients with cataract were drawn from the surgical
sures from ordinal raw scores. This improves the accu- waiting list (average waiting period 3 to 4 months) of the
racy of scoring and removes measurement noise,22–24 Ophthalmology Department, Flinders Medical Centre,
thus improving sensitivity to intervention-related Adelaide, South Australia. All patients had previously had
changes.22–25 Linear scoring also enables parametric sta- a comprehensive ocular examination and were diagnosed
to have cataract as the principal cause of visual disability
tistics to be validly applied to questionnaire scores. The and who required surgical intervention. Consecutive pa-
final aim was to make Rasch scoring available to all in- tients on the list were invited to participate. This included pa-
vestigators using the Cataract TyPE Spec questionnaire tients awaiting first- or second-eye surgery and those with
through a simple spreadsheet-based scoring conversion. ocular comorbidity (eg, glaucoma, diabetic retinopathy). It
is important to include these comorbidities as it is unlikely
to find a sample of an elderly cataract population without co-
PATIENTS AND METHODS existing ocular conditions. Other inclusion criteria were age
18 years or older, no severe cognitive impairment, and ability
Questionnaire to converse in English without the need for an interpreter.
The Cataract TyPE Spec questionnaire assesses visual Ethical approval was obtained, and all patients who agreed
functioning in 5 dimensions: distance vision, near vision, to participate signed a consent form. This research adhered
daytime driving, nighttime driving, and glare (Table 1). to the tenets of the Declaration of Helsinki.
There are 5 response options for the perceived difficulty
levels for both vision-related and glare-related questions Clinical Assessment
(summary scoring): totally disabled 5, quite a lot 4, some
difficulty 3, a little bit of difficulty 2, and not at all 1. An Visual acuity assessments were performed for each eye
additional option is provided if the subject does not do separately and binocularly using a computerized presenta-
an activity for other reasons, which is scored as zero, and tion of letters following logMAR principals with a screen
is considered as missing data for Rasch analysis. One ques- luminance of 150 candelas/m2 and letter-by-letter scoring.
tion relates to the global rating of vision. This question was Only binocular visual acuity measurements were used for
used to assess criterion validity. analysis because these are more closely related to disability
than better-eye or worse-eye measurements.26,27
Rasch Analysis
Submitted: January 27, 2009.
Final revision submitted: none. The Cataract TyPE Spec data were fitted to the Rasch rat-
Accepted: March 30, 2009. ing scale model28 using the Winsteps Rasch measurement
software29,30 (version 3.66, Winsteps). The item response the-
From the NH&MRC Centre for Clinical Eye Research (Gothwal, ory, specifically Rasch models, has been described in detail.31
Wright, Pesudovs), Department of Ophthalmology, Flinders Medi- Rasch models are probabilistic mathematical models that
cal Centre and Flinders University of South Australia, Bedford have been used in the validation of a series of vision-specific
Park, South Australia, the Centre for Eye Research Australia questionnaires.19,32–34 In brief, Rasch models attempt to esti-
mate the values of latent variables on an interval scale from
(Lamoureux), Department of Ophthalmology, University of Mel-
item scores that form an ordinal scale. In the Rasch model of
bourne, Victoria, and Vision CRC (Lamoureux), Sydney, Australia; visual disability, disability can be considered to lie on a ruler,
Meera and LB Deshpande Centre for Sight Enhancement (Gothwal), similar to an ordinary ruler, where ‘‘no disability’’ is an-
Vision Rehabilitation Centres, L.V. Prasad Eye Institute, Hyderabad, chored at one end and ‘‘maximum disability’’ at the other
India; Singapore Eye Research Institute (Lamoureux), Singapore end. The range of disability is expressed in log-odds proba-
National Eye Centre, Singapore. bility units (logits). The longer the scale length, the better it
is at representing the visual disability. An item (question)
No author has a financial or proprietary interest in any material or difficulty represents the position in logits that the item oc-
method mentioned. cupies on the linear disability scale; the center of the scale
is set at zero (ie, mean item difficulty). Similarly, person (par-
Supported in part by National Health and Medical Research Council, ticipant) ability represents the location of the person on the
Centre of Clinical Research Excellence Grant 264620, Canberra, same scale in logits. For the Cataract TyPE Spec instrument,
Australia. a positive logit score indicates a less difficult item and less
able participant (ie, the participant has lower ability than
Corresponding author: Konrad Pesudovs, NH&MRC Centre for that required to endorse the item).
Clinical Eye Research, Department of Ophthalmology, Flinders First, the participant’s use of the rating scale was exam-
Medical Centre, Bedford Park, South Australia, 5042, Australia. ined using the category probability curves. For a well-fitting
E-mail: konrad.pesudovs@flinders.edu.au. item, one would expect that across the whole range of the
J CATARACT REFRACT SURG - VOL 35, SEPTEMBER 2009
RASCH ANALYSIS: VALIDITY OF THE CATARACT TYPE SPEC INSTRUMENT 1511
Table 1. Items included in the original version of the Cataract TyPE Spec questionnaire.
Item Description Subscale
2 Vision hinders usual activity Distance vision
3 Vision hinders recognising people Distance vision
4 Vision hinders reading price labels Near vision
5 Vision hinders reading magazine Near vision
6 Vision hinders knitting Near vision
7 Vision hinders watching television Distance vision
8 Vision hinders daytime driving Daytime driving
9 Vision hinders nighttime driving Nighttime driving, glare
10 Glare hinders usual activities Glare
11 Glare hinders reading shiny paper Glare, near vision
12 Glare hinders driving toward the sun or oncoming Glare, daytime driving,
headlights nighttime driving
13 Glare hinders walking outside on a sunny day Glare
d Global rating question* d
*The original version included a global rating question: ‘‘How do you rate your vision?’’ This was not included in the score.
trait being measured (visual disability in this case), the high- If items do not fit the model’s expectations, unidimensional-
er response option (eg, quite a lot or totally disabled) would ity is not preserved.
show higher probability of endorsement than the lower Further examination of unidimensionality (a primary
response options (eg, a little bit of difficulty or not at all). requirement for measurement) was assessed using a principal
One of the most common source of items that do not fit is component analysis of the residuals.30,40 Unidimensionality
the participant’s inconsistent use of these response options, refers to the capacity of the instrument to measure the specific
which causes disordered thresholds. The threshold repre- attributes or underlying trait. Two criteria to were used to
sents the equal probability point between any 2 adjacent cat- confirm unidimensionality. First, the proportion of variance
egories. If disordering occurs, combining adjacent categories explained by the Rasch measure should be comparable for
can often, although not always, solve the problem and im- empirical calculation as well as that explained by the model.41
prove overall model fit. However, the newly formed cate- The second criterion is an eigenvalue less than 2.0 of the
gories remain theoretical and must be tested before being unexplained variance explained by the first contrast.42
recommended.35,36 Differential item functioning (DIF) concerns the expecta-
Second, the overall reliability of the Cataract TyPE Spec in- tion that participants who are in different groups but have
strument was estimated by examining the person-separation equal levels of visual disability would have the same proba-
statistics and person-separation reliability. Person separa- bility of selecting a particular response.43,44 Differential item
tion is a measure of spread in the test sample, and reliability functioning analyses were used to identify items potentially
is a measure of the true variance to the observed measure biased by age (!75 years versus R75 years), sex, systemic
variance. In general, reliability ranges from 0.0 to 1.0, with and ocular comorbidity, and first versus second eye surgery.
values higher than 0.8 (or person separation O2.0) consid- The definition of DIF was based on magnitude as follows: in-
ered the minimum acceptable level that indicates the ability significant DIF, !0.50 logits; mild (but probably inconse-
of the instrument to distinguish 3 strata of participants (high, quential), between 0.50 and 1.00 logits; and notable, O1.00
average, low) and that represents a useful range of task dif- logits.45,46 These DIF variables were selected a priori in the
ficulty.28,37 Model fit must be viewed in conjunction with re- present study. Age was included because cataract surgery
sponse scale functioning and item fit because problems in is performed over a wide age range. Sex was included be-
these 2 measurement properties can decrease overall model cause some of the items may be easier to perform for women
fit. than for men. Participants with comorbidities (systemic or
Third, compliance of the fit of the observed data to the ocular) may find some items more difficult than the rest. Par-
model expectations was assessed. Because the Rasch model ticipants who were awaiting cataract surgery in the second
is probabilistic and not deterministic, some failure of the eye may find some items easier to perform than those await-
model to predict the observed values is expected. Two statis- ing surgery in the first eye.
tics are used to represent these deviations: infit mean square In addition to the measurement properties described
(information-weighted fit statistic) and outfit mean square above, the Winsteps program enables item difficulty and per-
(outlier-sensitive fit statistic). Items that fit perfectly to the son ability to be visualized along a linear scale (like a ruler),
unidimensional scale have an expected infit and outfit which is known as a person–item map. Such a map can be
mean square of 1.0. Although acceptable levels of these fit used 3 ways; that is, to determine (1) the extent to which
statistics vary,38 values of 0.7 to 1.3 (30% less or more vari- item positions match person positions (targeting) (if posi-
ance than expected) were considered acceptable in the pres- tions do not line up, items are likely inappropriate [eg, too
ent study. Items with poorer fit statistics (ie, misfitting items) easy or too hard] for the persons); (2) whether there are
usually reflect a problem with coherence of the item with the gaps in the measure, which if present indicate the need for
underlying trait, and they are considered ‘‘noisy.’’39 Testing more items; (3) an item hierarchy, which provides informa-
for item fit forms 1 of the assessments of unidimensionality. tion about the most and least difficult items and more and
J CATARACT REFRACT SURG - VOL 35, SEPTEMBER 2009
1512 RASCH ANALYSIS: VALIDITY OF THE CATARACT TYPE SPEC INSTRUMENT
less able persons. For a valid measurement, a well-targeted 5-category response scale; therefore, the originally
scale must have adequate spread along the dimensions of proposed response scale was retained.
measurement with negligible floor and ceiling effects.47
The overall fit of the data to the model was good, in-
The proposed subscales of the Cataract TyPE Spec instru-
ment were analyzed separately using a rigorous approach dicating that overall, the 12-item scale formed a valid
similar that used for the entire instrument because subscales measure. The real person separation was 2.95 and
have the same requirements as whole scales for sufficiency of the reliability, 0.90.
psychometric properties.
Criterion validity was assessed by determining the rela-
Item Fit
tionship between the Likert score from the question on
global rating of vision and the Rasch-scaled score for the One item (‘‘How much does your vision hinder,
overall Rasch-scaled Cataract TyPE Spec score as well as limit, or disable you in nighttime driving?’’) showed
for the subscales. The relationship between visual acuity significant misfit (infit mean square 1.36). After the
and the Rasch-scaled score was also assessed.
Summarystatistics and correlations for criterion validity item was deleted, the infit mean square was within
were generated with SPSS statistical analysis software (ver- the acceptable range for the remaining 11 items, with
sion 16, SPSS, Inc.). A P value less than 0.05 was considered little loss of person separation (2.88).
statistically significant.
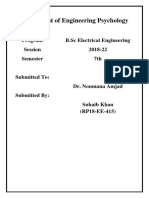
Targeting
RESULTS Figure 2 shows the person–item map for the revised
Two hundred ninety-four patients responded to the 11-item Cataract TyPE Spec questionnaire. The mean
visual disability scale. The 12 items were initially fitted person ability was 1.47 logits G 1.95 (SD). The range
to the Rasch model. Table 2 shows the patients’ of person ability (5.34 to 6.22 logits) was not signifi-
characteristics. cantly different from a normal distribution (Kolmo-
gorov-Smirnov Z test score 0.88, P Z .41). There was
Assessment of the Rating Scale and Reliability an uneven spread of items along the visual disability
continuum. On the whole, the items were too easy
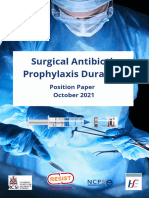
Figure 1 shows the category probability curves for
for the abilities of the patients. Further inadequacies
an item of the Cataract TyPE Spec questionnaire. There
in the measurement were reflected by redundancy of
was no evidence of disordered thresholds with the
the items; that is, pairs of items (eg, ‘‘reading price la-
bels in shops and supermarkets’’ and ‘‘reading shiny
Table 2. Participant characteristics (N Z 294). paper’’) were located at the same difficulty level, indi-
Characteristic Result
cating that they were addressing a similar activity.
Redundancy is acceptable only if the aim of the instru-
Mean age (y) GSD 74.6 G 9.5 ment is high precision rather than brevity. The
Sex, n (%)
Male 123 (41.8)
Female 171 (58.2)
Binocular visual acuity
Mean G SD
LogMAR 0.27 G 0.20
Snellen 6/12C
Range
LogMAR -0.14 to 1.00
Snellen 6/4.8C2 to 6/60
Awaiting second-eye surgery, n (%) 118 (41.9)
Ocular comorbidity,* n (%)
Present 136 (47.9)
Absent 148 (52.1)
Duration of cataract (y)
Median 1
Range 0 to 80
Systemic comorbidity,† n (%)
Present 258 (93.1)
Absent 19 (6.9)
Figure 1. Category probability curves for the 11-item Cataract TyPE
*Includes, for example, glaucoma, diabetic retinopathy, and age-related Spec questionnaire showing the range over which each of the 5 cat-
macular degeneration as well as data missing for 10 cases
† egories is most likely to be chosen. Boundaries occur at points along
Includes, for example, diabetes, hypertension, and angina as well as data
missing for 17 cases the scale where the category most likely to be chosen changes from
one to the next.
J CATARACT REFRACT SURG - VOL 35, SEPTEMBER 2009
RASCH ANALYSIS: VALIDITY OF THE CATARACT TYPE SPEC INSTRUMENT 1513
the unidimensionality of the Cataract TyPE Spec
instrument.
Differential Item Functioning
The Cataract TyPE Spec questionnaire was largely
free of DIF. However, 3 items showed a minimal
level of DIF by sex, with male participants rating 1
item as easier relative to other items: ‘‘vision hinders,
limits, or disables you in your usual activities’’ (0.58
logits). Female participants, on the other hand, rated
the following 2 items as easier than the male partic-
ipants: ‘‘knitting or sewing’’ (0.54 logits) and ‘‘walk-
ing outside on a sunny day’’ (0.71 logits).
Participants who did not have ocular comorbidity
rated the item ‘‘driving toward the sun’’ as 0.53 logits
easier than those who had ocular comorbidity.
Performance of Subscales Within the Rasch Model
Table 4 shows the results of subscale analyses. Of
the 5 proposed subscales, only glare and near vision
fit the Rasch model. Given the low level of discrimina-
tion of the remaining subscales, they did not form
valid scales. Furthermore, no amount of modifications
could improve the overall functioning of these sub-
scales to a satisfactory level.
Glare
Figure 2. Person–item map for 11-item Cataract TyPE Spec question- The person separation and reliability for glare fell
naire. The subjects are on the left of the dashed line, and more able within the recommend range (Table 4). One item
subjects are located at the bottom of the map. Items are located on (nighttime driving) misfit (infit mean square 1.45). Af-
the right of the dashed line and more difficult items are located at ter its deletion, the remaining 4 items fit and the person
the bottom of the map. Each ‘‘#’’ represents 2 subjects (M Z mean;
S Z 1 standard deviation from the mean; T Z 2 standard deviations
separation (2.11) remained largely unaffected. How-
from the mean). ever, the targeting worsened ( 1.34 logits). The princi-
pal components analysis of the residuals showed
unidimensionality. There was minimal DIF by sex
addition of items representing more difficult activities for 3 items. Male participants rated the following
would improve targeting of the instrument. 2 items as relatively easier compared with female par-
The 3 most difficult items were ‘‘driving toward ticipants: ‘‘glare hinders, limits, or disables your usual
the sun or oncoming headlights,’’ ‘‘knitting or sew- daily activities’’ (0.61 logits) and ‘‘read shiny paper’’
ing,’’ and ‘‘reading a magazine, newspaper, or (0.53 logits). Females, on the other hand, rated the
books.’’ Conversely, the 3 least difficult items were item ‘‘walking outside on a sunny day’’ 0.87 logits eas-
‘‘daytime driving,’’ ‘‘your usual daily activities (vi- ier compared with the male participants. This subscale
sion related),’’ and ‘‘your usual daily activities (glare formed a valid measure. However, similar to the full
related)’’ (Table 3). version of the Cataract TyPE Spec instrument, this sub-
scale was also targeted toward the less able end of the
population, with more able subjects having little or no
Unidimensionality difficulty with more difficult items.
The principal components analysis of the residuals
indicated that the variance explained by the measures Near Vision
was comparable for the empirical calculation (64.2%) The person separation and reliability for near vision
and by the model (65.0%). The unexplained variance were within the acceptable range (Table 4). There were
explained by the first contrast was 2.0 eigenvalue no misfitting items. In contrast to the glare subscale,
units, which is close to the magnitude seen with ran- the items in this subscale were better targeted to the
dom data. Taken together, these findings confirmed participants’ abilities. The principal components
J CATARACT REFRACT SURG - VOL 35, SEPTEMBER 2009
1514 RASCH ANALYSIS: VALIDITY OF THE CATARACT TYPE SPEC INSTRUMENT
Table 3. Item-fit statistics from the 11-item Cataract TyPE Spec questionnaire fitted to Rasch model.
TyPE Item Description Item Calibration Standard Error Infit Mean Square Outfit Mean Square
8 Day time driving 1.04 0.13 1.17 0.88
2 Usual daily activities (vision related) 0.88 0.09 0.92 0.87
10 Usual daily activities (glare related) 0.71 0.09 0.96 0.90
7 Watching television 0.49 0.09 1.01 1.07
3 Recognize people 0.40 0.09 1.27 1.22
13 Walking on sunny day 0.15 0.09 1.06 1.05
4 Reading price labels 0.45 0.09 0.87 0.82
11 Reading shiny paper 0.47 0.08 0.91 0.94
5 Reading a magazine 0.66 0.08 0.78 0.75
6 Knitting or sewing 0.69 0.10 1.17 1.14
12 Driving toward sun 1.41 0.10 1.17 1.16
analysis of the residuals confirmed unidimensionality. between 4 strata of participant ability. Our findings
No items showed DIF. This subscale also formed of high precision are in line with those reported for
a valid measure. Similar to the full version of the Cat- Catquest-9SF,21 another Rasch-revalidated question-
aract TyPE Spec instrument and the glare subscale, naire for a cataract population. There was no need to
this subscale was targeted toward the less able end collapse categories, supporting the originally pro-
of the population, with more able subjects having little posed 5-category response scale for the Cataract
or no difficulty with more difficult items. TyPE Spec questionnaire. Our finding of ordered
thresholds for a 5-category response scale in a cataract
Criterion Validity population is consistent with the 10-item Vision Core
Measure 1 scale.48 Although, other visual functioning
The Spearman rank correlation of visual acuity with
questionnaires used in cataract patients required fewer
the 11-item Rasch scaled Cataract TyPE Spec instru-
response categories,19 this difference probably reflects
ment was 0.25. There was a good statistically signifi-
the appropriateness of category labels for the Cataract
cant correlation (r Z 0.66, P!.0001) between the
TyPE Spec questionnaire. One reason for the optimum
global rating of vision and the 11-item Rasch scaled
use of the categories in this study could be because the
Cataract TyPE Spec instrument. The Spearman rank
categories (‘‘not at all,’’ ‘‘a little bit’’) are biased toward
correlation between the global rating of vision and
more able patients (ie, the less affected end of scale).
the glare subscale was 0.41 and between the global
However, despite ordered thresholds, there was
rating of vision and the near-vision subscale, 0.57
underuse of the extreme response category (ie, totally
(both P!.0001).
disabled, 4%); this reflects the finding of suboptimum
targeting in our study population.
DISCUSSION There was a significant floor effect in that the items
The Cataract TyPE Spec questionnaire performed well did not target participants with low levels of visual
in our population. It was highly discriminating, as evi- disability (ie, at bottom of the map). Although there
denced by the person separation for the 12-item Cata- were participants with low levels of visual disability
ract TyPE Spec and the revised 11-item version, (logits O 1.0), no items had difficulty estimates in
indicating that the instrument can discriminate that area. However, this may not entirely be the case
Table 4. Results of testing of fit of TyPE Spec subscales to the Rasch model.
Subscale
Parameter Glare Near Vision Daytime Driving Nighttime Driving Distance Vision
Items (n) 5 4 2 2 3
Misfitting items (n) 1 0 0 0 0
Person separation 2.10 2.02 1.21 1.40 1.41
Person separation reliability 0.81 0.80 0.59 0.66 0.67
Mean item location 0 0 0 0 0
Mean person location 0.87 0.88 2.79 0.56 1.69
Principal components analysis (eigenvalue) 1.6 1.5 d d 1.7
J CATARACT REFRACT SURG - VOL 35, SEPTEMBER 2009
RASCH ANALYSIS: VALIDITY OF THE CATARACT TYPE SPEC INSTRUMENT 1515
because items use multiple response categories and congruent to the overall trait, resulting in as much
each item is represented not just by its mean value noise as signal, because the removal of a good-fitting
by but levels of endorsement as well. Such intricate de- item would cause a loss of person separation.47
tails remain obscure in the person–item map. Never- The reduced 11-item version of Cataract TyPE Spec
theless, the restricted range of item difficulty questionnaire represents a unidimensional construct
(thresholds) indicates the Cataract TyPE Spec scale’s of visual disability in cataract patients. Because the
representation of the visual disability construct is Rasch model is sample-independent, the principal
skewed, suggesting less than optimum targeting of components analysis of the residuals provides a robust
the cataract patients to the questionnaire’s items and demonstration of its dimensionality. This important
thresholds. The participants were mistargeted by measurement characteristic reinforces that all the
1.47 logits. A little more than half the patients items on the 11-item Cataract TyPE Spec questionnaire
(59.9%) were awaiting surgery in their first eye, and hang together as a single construct of visual disability.
our findings of poor targeting are consistent with an- However, similar unidimensionality was apparent
other Rasch-validated questionnaire for use in cataract only in 2 subscales: glare and near vision. These sub-
patients; that is, the ADVS.19 The changing indications scales can reasonably discriminate between 3 strata
for cataract surgery are well documented,49 and cata- of the participant’s visual ability. Therefore, investiga-
ract surgery is now offered at a lower level of impair- tors can make use of the 2 valid subscales in addition to
ment in this part of the world than when these the overall score or simply implement them individu-
instruments were developed, which may explain the ally. Unfortunately, the other subscales of the Cataract
unsuitability of the items for the present cataract pop- TyPE Spec questionnaire did not perform well, as evi-
ulation. Targeting is sample-dependent21; therefore, denced by their poor person separation. This indicates
the Cataract TyPE Spec questionnaire may show opti- that these subscales do not meaningfully stratify par-
mum targeting in a more severely visually impaired ticipants; therefore, we do not endorse their reporting.
population in regions such as China and Africa.50 Dysfunctional subscales have been found in another
With the exception of the Catquest-9SF,21 poor target- Rasch revalidated questionnaire too, the original Cat-
ing has been common to all the Rasch-analyzed visual quest, and these were removed from the Rasch-scaled
function questionnaires in cataract patients.19,34,51 The revision, the Catquest-9SF.21
reason for good targeting using the Catquest-9SF The Cataract TyPE Spec was free of large DIF in our
questionnaire was related to optimum targeting of its population, indicating that it is consistent across sub-
long form in the same population. populations. It showed criterion validity when com-
In addition to evenly spacing item difficulties, it is de- pared with the self-rating of vision.
sirable that a questionnaire measures a long span of dif- We recommend the users of the Cataract TyPE Spec
ficulties. It is relatively easy to capture the functional perform Rasch analysis on their own data as popula-
level of persons who are severely disabled (eg, unable tions may vary. However, there may be clinicians
to read a magazine or unable to do usual daily activi- and researchers who wish to use the benefits of the
ties); however, it is much more difficult to measure Rasch-scaled scores without performing Rasch analy-
items at the other end of the spectrum. That is perhaps sis. Therefore, as stated in our aims, we developed
the reason that floor or ceiling effects are commonly a ready-to-use Microsoft Excel spreadsheet for conver-
seen in the visual function questionnaires. The only so- sion of raw to Rasch-scaled scores for the 11-item Cat-
lution to this problem is to add more difficult items to aract TyPE Spec instrument (see Supplementary
suit less impaired patients awaiting cataract surgery, Material which can be downloaded from the journal’s
particularly those waiting for second-eye surgery. web site or obtained by contacting the corresponding
Only 1 item (nighttime driving) consistently did not author). This spreadsheet converts ordinal category re-
fit the model for the full version and the glare subscale, sponses into 55 item–category calibrations to create
indicating that the response to this item was influ- Rasch measurement estimates. We caution that these
enced by attributes other than patient ability. This mis- conversions can be applied only if the sample it is be-
fit was predictable and is in line with findings in other ing applied to is similar to that in the present study.
studies, which report that driving items misfit with In conclusion, this study confirms the validity and
other items, such as reading.52,53 In the present study, reliability of the Cataract TyPE Spec within a Rasch
the misfit was probably because only little more than model. The important limitations of the instrument
half the patients (52.4%) drove and most reported are that only 2 of the 5 subscales are valid and the in-
greater difficulty with this activity. Deletion of this strument poorly targets the population. Poor targeting
item confirmed the remaining 11 items fit the Rasch limits the prospect for measuring the outcome of cata-
model; however, it did not significantly reduce person ract surgery; thus, other instruments, such as the Cat-
separation. This suggests that the item was not quest-9SF, may be a better choice. Better still would be
J CATARACT REFRACT SURG - VOL 35, SEPTEMBER 2009
1516 RASCH ANALYSIS: VALIDITY OF THE CATARACT TYPE SPEC INSTRUMENT
to develop item banking and computer adaptive test- 15. Massof RW. The measurement of vision disability. Optom Vis Sci
ing that can tailor item difficulty to suit the abilities 2002; 79:516–552. Available at: http://www.optvissci.com/pt/re/
ovs/pdfhandler.00006324-200208000-00015.pdf%3Bjsessio
of a given patient. Similar approaches have been nidZKZYSBB5kbwjgJ6YYXzpgLywwBK16QcpSb8q3bQGC3
used for other areas of health care54,55 but have yet 1s8vY3cdGzj!-701738752!181195629!8091!-1. Accessed May
to be developed for ophthalmology. 24, 2009
16. Rasch G. Probabilistic Models for Some Intelligence and
Attainment Tests. Copenhagen, Denmark, Institute of Educa-
REFERENCES tional Research, 1960
1. McCarty CA, Mukesh BN, Fu CL, Taylor HR. The epidemiology 17. Pesudovs K, Burr JM, Harley C, Elliott DB. The development,
of cataract in Australia. Am J Ophthalmol 1999; 128:446–465 assessment, and selection of questionnaires. Optom Vis Sci
2. Keeffe JE, Taylor HR. Cataract surgery in Australia. Aust N Z J 2007; 84:664–675. Available at: http://www.optvissci.com/pt/re/
Ophthalmol 1996; 24:313–317 ovs/pdfhandler.00006324-200708000-00005.pdf;jsessionidZ
3. Taylor HR. Cataract: how much surgery do we have to do? KZcJrBxMKHzzcx4VGhCDgGwV2vDSD5HknjcG729LKxDlX1
[editorial] Br J Ophthalmol 2000; 84:1–2. Available at: http:// XPvfm1!-701738752!181195629!8091!-1. Accessed May 24,
www.pubmedcentral.nih.gov/picrender.fcgi?artidZ1723236& 2009
blobtypeZpdf. Accessed May 24, 2009 18. Mallinson T. Why measurement matters for measuring patient vi-
4. Desai P, Reidy A, Minassian DC, Vafidis G, Bolger J. Gains from sion outcomes. Optom Vis Sci 2007; 84. Available at: http://
cataract surgery: visual function and quality of life. Br J Ophthalmol www.optvissci.com/pt/re/ovs/pdfhandler.00006324-200708000-
1996; 80:868–873. Available at: http://www.pubmedcentral.nih. 00006.pdf;jsessionidZKZcW21QvZ9vvSbXT2Y5S7dNchsSTl
gov/picrender.fcgi?artidZ505640&blobtypeZpdf. Accessed wjP2TbTJFyJJYG2tgLLc2LR!-701738752!181195629!8091!-1.
May 24, 2009 Accessed May 24, 2009
5. Mönestam E, Wachtmeister L. Dissatisfaction with cataract sur- 19. Pesudovs K, Garamendi E, Keeves JP, Elliott DB. The Activities
gery in relation to visual results in a population-based study in of Daily Vision Scale for cataract surgery outcomes: re-evaluat-
Sweden. J Cataract Refract Surg 1999; 25:1127–1134 ing validity with Rasch analysis. Invest Ophthalmol Vis Sci 2003;
6. Brenner MH, Curbow B, Javitt JC, Legro MW, Sommer A. Vision 44:2892–2899. Available at: http://www.iovs.org/cgi/reprint/44/
change and quality of life in the elderly; response to cataract 7/2892. Accessed May 24, 2009
surgery and treatment of other chronic ocular conditions. Arch 20. Velozo CA, Lai J-S, Mallinson T, Hauselman E. Maintaining
Ophthalmol 1993; 111:680–685. Available at: http://archopht. instrument quality while reducing items: application of Rasch
ama-assn.org/cgi/reprint/111/5/680. Accessed May 24, 2009 analysis to a self-report of visual function. J Outcome Meas
7. Mangione CM, Phillips R, Seddon JM, Lawrence MG, Cook EF, 2000–2001; 4:667–680
Dailey R, Goldman L. Development of the ‘Activities of Daily 21. Lundström M, Pesudovs K. Catquest-9SF patient outcomes
Vision Scale.’ A measure of visual functional status. Med Care questionnaire; nine-item short-form Rasch-scaled revision of
1992; 30:1111–1126 the Catquest questionnaire. J Cataract Refract Surg 2009;
8. Mangione CM, Orav EJ, Lawrence MG, Phillips RS, Seddon JM, 35:504–513
Goldman L. Prediction of visual function after cataract surgery; 22. Garamendi E, Pesudovs K, Stevens MJ, Elliott DB. The Refrac-
a prospectively validated model. Arch Ophthalmol 1995; tive Status and Vision Profile: evaluation of psychometric prop-
113:1305–1311. Available at: http://archopht.ama-assn.org/ erties and comparison of Rasch and summated Likert-scaling.
cgi/reprint/113/10/1305. Accessed May 24, 2009 Vision Res 2006; 46:1375–1383
9. Pesudovs K, Coster DJ. An instrument for assessment of sub- 23. Pesudovs K. Patient-centred measurement in ophthalmology –
jective visual disability in cataract patients. Br J Ophthalmol a paradigm shift [commentary]. BMC Ophthalmol 2006; 6:25.
1998; 82:617–624. Available at: http://www.pubmedcentral.nih. Available at: http://www.biomedcentral.com/content/pdf/1471-
gov/picrender.fcgi?artidZ1722619&blobtypeZpdf. Accessed 2415-6-25.pdf. Accessed May 24, 2009
May 24, 2009 24. Norquist JM, Fitzpatrick R, Dawson J, Jenkinson C. Comparing
10. Steinberg EP, Tielsch JM, Schein OD, Javitt JC, Sharkey P, alternative Rasch-based methods vs raw scores in measuring
Cassard SD, Legro MW, Diener-West M, Bass EB, change in health. Med Care 2004; 42(suppl 1):I25–I36
Damiano AM, Steinwachs DM, Sommer A. The VF-14; an index 25. Pesudovs K, Garamendi E, Elliott DB. The Quality of Life Impact
of functional impairment in patients with cataract. Arch Ophthal- of Refractive Correction (QIRC) Questionnaire: development
mol 1994; 112:630–638. Available at: http://archopht.ama-assn. and validation. Optom Vis Sci 2004; 81:769–777. Available at:
org/cgi/reprint/112/5/630. Accessed May 24, 2009 http://www.optvissci.com/pt/re/ovs/pdfhandler.00006324-2004
11. Lundström M, Roos P, Jensen S, Fregell G. Catquest 10000-00009.pdf;jsessionidZKZlQrwyhmlzpQ0JgPykLn0wJq
questionnaire for use in cataract surgery care: description, 9FlTyYqrNBBQCG2kTPPcB41qvh1!-1775402713!18119562
validity, and reliability. J Cataract Refract Surg 1997; 23: 8!8091!-1. Accessed May 24, 2009
1226–1236 26. Elliott DB, Hurst MA, Weatherill J. Comparing clinical tests of
12. Javitt JC, Jacobson G, Schiffman RM. Validity and reliability of visual function in cataract with the patient’s perceived visual dis-
the Cataract TyPE Spec: an instrument for measuring outcomes ability. Eye 1990; 4:712–717
of cataract extraction. Am J Ophthalmol 2003; 136:285–290 27. Rubin GS, Muñoz B, Bandeen-Roche K, West SK. Monocular ver-
13. Lawrence DJ, Brogan C, Benjamin L, Pickard D, Stewart- sus binocular visual acuity as measures of vision impairment and
Brown S. Measuring the effectiveness of cataract surgery: the predictors of visual disability; for the SEE Project Team. Invest
reliability and validity of a visual function outcomes instrument. Ophthalmol Vis Sci 2000; 41:3327–3334. Available at: http://
Br J Ophthalmol 1999; 83:66–70; Available: http://www.pub www.iovs.org/cgi/reprint/41/11/3327. Accessed May 24, 2009
medcentral.nih.gov/picrender.fcgi?artidZ1722791&blobtypeZ 28. Wright BD, Masters GN. Rating Scale Analysis (Rasch Mea-
pdf. Accessed May 24, 2009 surement Book). Chicago, IL, MESA Press, 1982
14. Massof RW, Rubin GS. Visual function assessment question- 29. Linacre JM, Wright BD. A User’s Guide to WINSTEPS: Rasch
naires. Surv Ophthalmol 2001; 45:531–548 model computer program. Chicago, IL, MESA Press, 2000
J CATARACT REFRACT SURG - VOL 35, SEPTEMBER 2009
RASCH ANALYSIS: VALIDITY OF THE CATARACT TYPE SPEC INSTRUMENT 1517
30. Linacre JM. A User’s Guide to WINSTEPS/MINISTEPS; 44. Holland PW, Wainer H, eds, Differential Item Functioning. Hill-
Rasch-Model Computer Programs. Chicago, IL, MESA Press, sdale, NJ, Lawrence Erlbaum Associates, 1993
2009;. Available at: http://www.winsteps.com/winman/index.- 45. Wright BD, Douglas GA. Best Test Design and Self-Tailored
htm?copyright.htm. Accessed May 24, 2009 Testing. MESA Research Memorandum No. 19. Statistical
31. Andrich D. A rating formulation for ordered response categories. Laboratory, Department of Education. Chicago, IL, University
Psychometrika 1978; 43:561–573 of Chicago, 1975
32. Lamoureux EL, Pallant JF, Pesudovs K, Hassell JB, Keeffe JE. 46. Wright BD, Douglas GA. Rasch Item Analysis by Hand MESA
The impact of vision impairment questionnaire: an evaluation of Research Memorandum Number 21. Statistical Laboratory, De-
its measurement properties using Rasch analysis. Invest Oph- partment of Education. Chicago, IL, University of Chicago, 1976
thalmol Vis Sci 2006; 47:4732–4741. Available at: http:// 47. Mallinson T, Stelmack J, Velozo C. A comparison of the separa-
www.iovs.org/cgi/reprint/47/11/4732. Accessed May 24, 2009 tion ratio and coefficient a in the creation of minimum item sets.
33. Massof RW, Fletcher DC. Evaluation of the NEI visual function- Med Care 2004; 42(suppl 1):I17–I24
ing questionnaire as an interval measure of visual ability in low 48. Lamoureux EL, Pesudovs K, Pallant JF, Rees G, Hassell JB,
vision. Vision Res 2001; 41:397–413 Caudle LE, Keeffe JE. An evaluation of the 10-item vision core
34. Velozo CA, Lai J-S, Mallinson T, Hauselman E. Maintaining measure 1 (VCM1) scale (the Core Module of the Vision-Related
instrument quality while reducing items: application of Rasch Quality of Life scale) using Rasch analysis. Ophthalmic Epide-
analysis to a self-report of visual function. J Outcome Meas miol 2008; 15:224–233
2000–2001; 4:667–680 49. Leinonen J, Laatikainen L. Changes in visual acuity of patients
35. Comins J, Brodersen J, Krogsgaard M, Beyer N. Rasch analysis undergoing cataract surgery during the last two decades. Acta
of the Knee Injury and Osteoarthritis Outcome Score (KOOS): Ophthalmol Scand 2002; 80:506–511
a statistical re-evaluation. Scand J Med Sci Sports 2008; 50. Foster A. Vision 2020: the cataract challenge [editorial]. J Comm
18:336–345 Eye Health 2000; 13(34):17–19. Available at: http://www.
36. Wolfe F, Michaud K, Pincus T. Development and validation of the cehjournal.org/download/ceh_13_34_017.pdf. Accessed May
Health Assessment Questionnaire II; a revised version of the 24, 2009
Health Assessment Questionnaire. Arthritis Rheum 2004; 51. Pesudovs K, Caudle LE, Rees G, Lamoureux EL. Validity of a vi-
50:3296–3305. Available at: http://www3.interscience.wiley. sual impairment questionnaire in measuring cataract surgery
com/cgi-bin/fulltext/109677229/PDFSTART. Accessed May 24, outcomes. J Cataract Refract Surg 2008; 34:925–933
2009 52. Globe D, Varma R, Azen SP, Paz S, Yu E, Preston-Martin SLos
37. Smith EV Jr. Evidence for the reliability of measures and validity Angeles Latino Eye Study Group. Psychometric performance of
of measure interpretation: a Rasch measurement perspective. the NEI VFQ-25 in visually normal Latinos: the Los Angeles La-
J Appl Meas 2001; 2:281–311 tino eye study. Invest Ophthalmol Vis Sci 2003; 44:1470–1478.
38. Wright BD, Linacre JM. Reasonable mean-square fit values. Available at: http://www.iovs.org/cgi/reprint/44/4/1470. Ac-
Rasch Measurement Transactions 1994; 8:370. Available at: cessed May 24, 2009
http://www.rasch.org/rmt/rmt83b.htm. Accessed May 24, 2009 53. Massof RW, Hsu CT, Baker FH, Barnett GD, Park WL,
39. Smith RM. Person fit in the Rasch model. Educ Psychol Mea- Deremeik JT, Rainey C, Epstein C. Visual disability variables.
surement 1986; 46:359–372 II: The difficulty of tasks for a sample of low-vision patients.
40. Smith EV Jr. Detecting and evaluating the impact of multidimen- Arch Phys Med Rehabil 2005; 86:954–967. Available at: http://
sionality using item fit statistics and principal component analy- download.journals.elsevierhealth.com/pdfs/journals/0003-
sis of residuals. J Appl Meas 2002; 3:205–231 9993/PIIS0003999304013978.pdf. Accessed May 24, 2009
41. Bond TG, Fox CM. Applying the Rasch Model: Fundamental 54. Lai J-S, Cella D, Dineen K, Bode R, Von Roenn J, Gershon RC,
Measurement in the Human Sciences. London, UK, Lawrence Shevrin D. An item bank was created to improve the measure-
Erlbaum Associates, 2001 ment of cancer-related fatigue. J Clin Epidemiol 2005; 58:
42. Linacre JM. A User’s Guide to WINSTEPS. Chicago, IL, MESA 190–197
Press, 2009 55. Walter OB, Becker J, Bjorner JB, Fliege H, Klapp BF, Rose M.
43. Teresi JA. Different approaches to differential item functioning in Development and evaluation of a computer adaptive test for
health applications. advantages, disadvantages and some ne- ‘Anxiety’ (Anxiety-CAT). Qual Life Res 2007; 16(suppl 1):
glected topics. Med Care 2006; 44:S152–S170 143–155
J CATARACT REFRACT SURG - VOL 35, SEPTEMBER 2009
You might also like
- Ebook Biomarker GuideDocument40 pagesEbook Biomarker Guidepallavi patil100% (1)
- Patient Information: Reteval ™Document4 pagesPatient Information: Reteval ™pallavi patilNo ratings yet
- Status of Pediatric Eye Care in India.7Document8 pagesStatus of Pediatric Eye Care in India.7pallavi patilNo ratings yet
- IN2015 Chapter5Document15 pagesIN2015 Chapter5pallavi patilNo ratings yet
- Cost Effectiveness Analysis Should Continually.7Document5 pagesCost Effectiveness Analysis Should Continually.7pallavi patilNo ratings yet
- Oculoplasty Basics: Clinical Work Up Proformas: September 2020Document20 pagesOculoplasty Basics: Clinical Work Up Proformas: September 2020pallavi patilNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- WASHINGTON, DC - JANUARY 04: U.S. House Majority Leader Rep. Eric Cantor (R-VA) (C) Walks Towards The HouseDocument6 pagesWASHINGTON, DC - JANUARY 04: U.S. House Majority Leader Rep. Eric Cantor (R-VA) (C) Walks Towards The HouseShie La Santillan MedezNo ratings yet
- Surgical Antibiotic Prophylaxis Duration Position Statement October 2021 v1Document3 pagesSurgical Antibiotic Prophylaxis Duration Position Statement October 2021 v1debby twonabilaNo ratings yet
- Guidelines For Diagnostic Imaging During Pregnancy and Lactation PDFDocument7 pagesGuidelines For Diagnostic Imaging During Pregnancy and Lactation PDFMuhammad nafisNo ratings yet
- Developmental Profile PrekDocument7 pagesDevelopmental Profile Prekapi-3171385680% (2)
- Jean Monnet Teaching ActivityDocument1 pageJean Monnet Teaching ActivityBoban StojanovicNo ratings yet
- Hajiron, Rose Ann S. BSN-4B - Cognitive Behavioral Therapy (Rot6) FinalDocument21 pagesHajiron, Rose Ann S. BSN-4B - Cognitive Behavioral Therapy (Rot6) FinalROSE ANN SABIRAN. HAJIRONNo ratings yet
- Badger Airbrush Model 175 CrescendoDocument12 pagesBadger Airbrush Model 175 CrescendoKristel ClearyNo ratings yet
- Sika Form Oil PDFDocument2 pagesSika Form Oil PDFmilanbrasinaNo ratings yet
- Food AdditivesDocument1 pageFood AdditivesChristine100% (1)
- Ethical Business - Salsabila LuvaridianDocument20 pagesEthical Business - Salsabila LuvaridianSalsabila SalsaNo ratings yet
- Milton Lappin, Detroit, MichDocument10 pagesMilton Lappin, Detroit, MichMarcos CastroNo ratings yet
- Inc Affiliated List of Colleges 2020-21Document61 pagesInc Affiliated List of Colleges 2020-21Babita KumariNo ratings yet
- Final Year Presentation of BS CS 179 (Haider Ali Talha Saleem Humza Huassin)Document21 pagesFinal Year Presentation of BS CS 179 (Haider Ali Talha Saleem Humza Huassin)rao talha100% (1)
- Kenya Registration - Food & Dietary SupplementsDocument21 pagesKenya Registration - Food & Dietary SupplementsDRIVECURENo ratings yet
- Restaurant Report Card - December 2, 2021Document3 pagesRestaurant Report Card - December 2, 2021KBTXNo ratings yet
- 台 灣 漢 族 酒 癮 者 以 ALDH2對 偶 基 因 型 分 組 後 於 酒 精 效 果 預 期 、 酒 癮 渴 求 與 飲 酒 量 之 差 異 The Differences in Alcohol Outcome Expectancy, Alcohol Craving and Alcohol Consumption betweenDocument80 pages台 灣 漢 族 酒 癮 者 以 ALDH2對 偶 基 因 型 分 組 後 於 酒 精 效 果 預 期 、 酒 癮 渴 求 與 飲 酒 量 之 差 異 The Differences in Alcohol Outcome Expectancy, Alcohol Craving and Alcohol Consumption betweenjennyNo ratings yet
- CarbohydratesDocument4 pagesCarbohydratesKuhu MakadiaNo ratings yet
- EP Assignment RP18 EE 415Document6 pagesEP Assignment RP18 EE 415Ijaz AhmadNo ratings yet
- CPP Mini Cex Form v1.0Document2 pagesCPP Mini Cex Form v1.0bobfooNo ratings yet
- Jacob Levy Morenos Psychodrama As A Work TechniquDocument12 pagesJacob Levy Morenos Psychodrama As A Work TechniquAdriana EneNo ratings yet
- Bijcrid 20221103Document5 pagesBijcrid 20221103BOHR International Journal of Current research in Dentistry (BIJCRID)No ratings yet
- New Book AnnotationsDocument1 pageNew Book Annotationslee tohNo ratings yet
- Agresivnost Kod Djece I AdolescenataDocument12 pagesAgresivnost Kod Djece I Adolescenatamatea tijaNo ratings yet
- TSBDocument9 pagesTSBrovimosh100% (2)
- Rufina M. Cruz - Salvador RN, MAN Lecturer NCM 120Document224 pagesRufina M. Cruz - Salvador RN, MAN Lecturer NCM 120Alexander Blanche PajelaNo ratings yet
- Aspiration Pneumonia Recommendations 2023Document19 pagesAspiration Pneumonia Recommendations 2023ctsakalakisNo ratings yet
- Seven Secrets of The Killer Resume: AuthorDocument3 pagesSeven Secrets of The Killer Resume: AuthorjayNo ratings yet
- Thomas J. Butler PH.D RRT RPFT - Laboratory Exercises For Competency in Respiratory Care-F.a. Davis Company (201Document865 pagesThomas J. Butler PH.D RRT RPFT - Laboratory Exercises For Competency in Respiratory Care-F.a. Davis Company (201Celia Seneh GwandiNo ratings yet
- Flexible Working PolicyDocument7 pagesFlexible Working PolicySophie-Louise MercedesNo ratings yet
- White Brown Professional Cover Letter - 20231125 - 072415 - 0000Document1 pageWhite Brown Professional Cover Letter - 20231125 - 072415 - 0000leackyotieno4No ratings yet