You might also like
- Autism Spectrum Disorder: Bioregenerative Medicine With Stem Cell TherapyFrom EverandAutism Spectrum Disorder: Bioregenerative Medicine With Stem Cell TherapyNo ratings yet
- The Primary Care of Seizure Disorders: A Practical Guide to the Evaluation and Comprehensive Management of Seizure DisordersFrom EverandThe Primary Care of Seizure Disorders: A Practical Guide to the Evaluation and Comprehensive Management of Seizure DisordersNo ratings yet
- Tau PET and Multimodal Brain Imaging in Patients at Risk F - 2019 - NeuroImageDocument13 pagesTau PET and Multimodal Brain Imaging in Patients at Risk F - 2019 - NeuroImageBruno MañonNo ratings yet
- Advantage of Modified MRI Protocol For HDocument148 pagesAdvantage of Modified MRI Protocol For HasasakopNo ratings yet
- Schizophrenia Stigma in Mental Health Professionals and Associated Factors A Systematic ReviewDocument1 pageSchizophrenia Stigma in Mental Health Professionals and Associated Factors A Systematic ReviewFrida Ximena Perez CaballeroNo ratings yet
- Shin-2011-International Journal of Geriatric PsychiatryDocument3 pagesShin-2011-International Journal of Geriatric PsychiatryImanNo ratings yet
- Cross-national epidemiology of panic disorder and attacksDocument23 pagesCross-national epidemiology of panic disorder and attacksSATRIO BAGAS SURYONEGORONo ratings yet
- Mediterranean Diet and 3year Alzheimer Brain Biomarker Changes in Middle Aged AdultsDocument11 pagesMediterranean Diet and 3year Alzheimer Brain Biomarker Changes in Middle Aged AdultsMariNo ratings yet
- Diabetes Articulo NuevoDocument9 pagesDiabetes Articulo NuevoAn GelNo ratings yet
- Association of Plasma Total Tau Level With Cognitive Decline and Risk of Mild Cognitive Impairment or Dementia in The Mayo Clinic Study On AgingDocument8 pagesAssociation of Plasma Total Tau Level With Cognitive Decline and Risk of Mild Cognitive Impairment or Dementia in The Mayo Clinic Study On AgingeastareaNo ratings yet
- Mind Diet Adherence and Cognitive PerformandeDocument13 pagesMind Diet Adherence and Cognitive PerformandeSaionara FranciscoNo ratings yet
- Mp201672a MolekularDocument9 pagesMp201672a MolekularNadia OktarinaNo ratings yet
- Amico F Et Al (2023) A Resting State EEG Study On Depressed Persons With Suicidal Ideation IBRO Neuroscience ReportsDocument7 pagesAmico F Et Al (2023) A Resting State EEG Study On Depressed Persons With Suicidal Ideation IBRO Neuroscience ReportsAlparslan OnderNo ratings yet
- JOHNSTON Brainstem Abnormalities in Attention Deficit Hyperactivity Disorder Support High Accuracy Individual Diagnostic ClassificationDocument11 pagesJOHNSTON Brainstem Abnormalities in Attention Deficit Hyperactivity Disorder Support High Accuracy Individual Diagnostic Classificationexcelencia5No ratings yet
- Depresión-Alteraciones Subcorticales-Schmaal 2015Document7 pagesDepresión-Alteraciones Subcorticales-Schmaal 2015Kitzia AveiriNo ratings yet
- Antidiabetic Medications in RelationDocument7 pagesAntidiabetic Medications in RelationjayNo ratings yet
- 10.1007@s00408 020 00340 7Document5 pages10.1007@s00408 020 00340 7Sergio Vargas CarrilloNo ratings yet
- Est. Trans C. e Bipo.Document19 pagesEst. Trans C. e Bipo.Luciana OliveiraNo ratings yet
- 31108978Document19 pages31108978kdafloresaNo ratings yet
- Temporal Lobe Epilepsy With Amygdala Enlargement: A Subtype of Temporal Lobe EpilepsyDocument8 pagesTemporal Lobe Epilepsy With Amygdala Enlargement: A Subtype of Temporal Lobe EpilepsyRavi ChandraNo ratings yet
- Alzheimer 5Document14 pagesAlzheimer 5Elena MironNo ratings yet
- Tab VS DFTDocument15 pagesTab VS DFTAntu NandaNo ratings yet
- Frontiers in Neuroendocrinology: A B C D e F G H IDocument14 pagesFrontiers in Neuroendocrinology: A B C D e F G H IIonela BogdanNo ratings yet
- DZNEDocument10 pagesDZNEeastareaNo ratings yet
- Ossenkoppele 2019 PET Tau Pet Amyloid Cortical ThicknessDocument13 pagesOssenkoppele 2019 PET Tau Pet Amyloid Cortical ThicknessAngela SilvaNo ratings yet
- Transcranial Magnetic Stimulation in Alzheimer's Disease - Are We Ready?Document11 pagesTranscranial Magnetic Stimulation in Alzheimer's Disease - Are We Ready?aamchnbNo ratings yet
- Brini2017 PDFDocument16 pagesBrini2017 PDFAde Maghvira PutriNo ratings yet
- Progression of Brain Atrophy and Cognitive Decline in Diabetes MellitusDocument2 pagesProgression of Brain Atrophy and Cognitive Decline in Diabetes MellitusWidi AdnyanaNo ratings yet
- LongtermeffectsDocument9 pagesLongtermeffectsLindenberger BoriszNo ratings yet
- Metabolic Syndrome, Mild Cognitive Impairment, and Dementia: A Meta-Analysis of Longitudinal StudiesDocument13 pagesMetabolic Syndrome, Mild Cognitive Impairment, and Dementia: A Meta-Analysis of Longitudinal StudiesMiguelySusy Ramos-RojasNo ratings yet
- Hallucinations in Dementia Psychosis in Neurodegenerative Disease Differential Patterns of Hallucination and Delusion SymptomsDocument14 pagesHallucinations in Dementia Psychosis in Neurodegenerative Disease Differential Patterns of Hallucination and Delusion SymptomsSultan TarlacıNo ratings yet
- 2014 Delirium in Elderly PeopleDocument12 pages2014 Delirium in Elderly Peoplejuan.pablo.castroNo ratings yet
- Alzheimer S Dementia - 2012 - MielkeDocument9 pagesAlzheimer S Dementia - 2012 - MielkeEccoNo ratings yet
- Wessels Et Al. - 2007 - Cognitive Performance in Type 1 Diabetes Patients Is Associated With Cerebral White Matter VolumeDocument7 pagesWessels Et Al. - 2007 - Cognitive Performance in Type 1 Diabetes Patients Is Associated With Cerebral White Matter VolumeJUAN PABLO PEREZ PEREIRANo ratings yet
- JSL 047Document15 pagesJSL 047Alí Jorkaeff Hernández LópezNo ratings yet
- Riedel - 2011 - Clinical Predictors of Response and Remission in Inpatients With Depressive SyndromesDocument13 pagesRiedel - 2011 - Clinical Predictors of Response and Remission in Inpatients With Depressive SyndromesRicardo DíazNo ratings yet
- 2020 Invasive Electrical Neuromodulation For The Treatment of Painful Diabetic Neuropathy Systematic Review and Meta-AnalysisDocument9 pages2020 Invasive Electrical Neuromodulation For The Treatment of Painful Diabetic Neuropathy Systematic Review and Meta-AnalysisSafitri MuhlisaNo ratings yet
- Remote monitoring strategies for ADHD medicationDocument3 pagesRemote monitoring strategies for ADHD medicationAnti DamayantiNo ratings yet
- Clinicopathological Correlations in BehaviouralDocument17 pagesClinicopathological Correlations in BehaviouralAlexandra CastellanosNo ratings yet
- Alteraciones Adultos MayoresDocument12 pagesAlteraciones Adultos MayoresGabriel Zúñiga MartinezNo ratings yet
- 22Q 11 2-WiscDocument21 pages22Q 11 2-WiscMRHNo ratings yet
- Mediterranean Diet and Brain Structure in A Multiethnic Elderly CohortDocument9 pagesMediterranean Diet and Brain Structure in A Multiethnic Elderly Cohortx92q9rwjmgNo ratings yet
- Clinica Encefalitis Nmda InglesDocument7 pagesClinica Encefalitis Nmda InglesOskr MezaNo ratings yet
- Schizophrenia and Psychiatric Comorbidities Recognition Management (Oxford Psychiatry Library Series) (David J. Castle, Peter F. Buckley Etc.) (Z-Library)Document156 pagesSchizophrenia and Psychiatric Comorbidities Recognition Management (Oxford Psychiatry Library Series) (David J. Castle, Peter F. Buckley Etc.) (Z-Library)Emier Zulhilmi100% (1)
- Birkefeld (2022)Document14 pagesBirkefeld (2022)Nerea AlvarezNo ratings yet
- Dopamine Related Frontostriatal Abnormalities in Obesity and Binge Eating Disorder Emerging Evidence For Developmental PsychopathologyDocument9 pagesDopamine Related Frontostriatal Abnormalities in Obesity and Binge Eating Disorder Emerging Evidence For Developmental PsychopathologyAnna MoveNo ratings yet
- Articulo Sobre Eficacia Ayuno Intermitente en EMDocument18 pagesArticulo Sobre Eficacia Ayuno Intermitente en EMPedro Rodriguez PicazoNo ratings yet
- Psychiatric Comorbidities in EpilepsyDocument6 pagesPsychiatric Comorbidities in EpilepsydhruvaNo ratings yet
- Depression in Neurodegenerative Diseases - Common Mechanisms and Current Treatment OptionsDocument103 pagesDepression in Neurodegenerative Diseases - Common Mechanisms and Current Treatment OptionsAna Paula LopesNo ratings yet
- AlzheimerDocument25 pagesAlzheimerNET-AVÓNo ratings yet
- NeurologiaDocument216 pagesNeurologiaPietro BracagliaNo ratings yet
- Amyloid Pathologies Modulate The Associations of Minimal Depr - 2021 - BiologicaDocument10 pagesAmyloid Pathologies Modulate The Associations of Minimal Depr - 2021 - BiologicaPriscilla ChantalNo ratings yet
- Predictors of Poor Treatment Response ToDocument13 pagesPredictors of Poor Treatment Response ToMaite Novo del valleNo ratings yet
- Detecting HIV-Associated Neurocognitive Disorders in Adolescents: Which Screening Tool Is BestDocument3 pagesDetecting HIV-Associated Neurocognitive Disorders in Adolescents: Which Screening Tool Is BestBruno Fernandes Borginho0% (1)
- Age and Neurodegeneration ImagingDocument9 pagesAge and Neurodegeneration ImagingChouaib OujhainNo ratings yet
- Resting-State EEG Microstates and Power Spectrum IDocument14 pagesResting-State EEG Microstates and Power Spectrum IChu Thị NghiệpNo ratings yet
- No Bidirectional Relationship Between Depression and Periodontitis: A Genetic Correlation and Mendelian Randomization StudyDocument9 pagesNo Bidirectional Relationship Between Depression and Periodontitis: A Genetic Correlation and Mendelian Randomization StudyOaNa GrigorutaNo ratings yet
- The Ketogenic Diet As A Non Pharmacological Treatment For HIV Associated Neurocognitive Disorder A Descriptive AnalysisDocument5 pagesThe Ketogenic Diet As A Non Pharmacological Treatment For HIV Associated Neurocognitive Disorder A Descriptive AnalysisPaul HartingNo ratings yet
- Retrieve 2Document9 pagesRetrieve 2api-664106052No ratings yet
- Jamaneurology Hendriks 2021 Oi 210036 1630683443.28039Document11 pagesJamaneurology Hendriks 2021 Oi 210036 1630683443.28039aymee fernandezNo ratings yet
- Kassam 2009 ADocument6 pagesKassam 2009 Anatsumi18No ratings yet
- Pabst Stress&DecisionMaking&Timing BehavBrainRes (2013)Document8 pagesPabst Stress&DecisionMaking&Timing BehavBrainRes (2013)natsumi18No ratings yet
- Police CortDocument9 pagesPolice Cortnatsumi18No ratings yet
- Yip-Psychological Science-2012-0956797612450031Document8 pagesYip-Psychological Science-2012-0956797612450031natsumi18No ratings yet
- Measuring Misery Around The World, May 2014 - 26DQ PDFDocument4 pagesMeasuring Misery Around The World, May 2014 - 26DQ PDFjorgenittiNo ratings yet
- Journal Pone 0103940Document13 pagesJournal Pone 0103940natsumi18No ratings yet
- Empatia Base NeuronalDocument25 pagesEmpatia Base Neuronalnatsumi18No ratings yet
- EI competences predict cross-cultural adjustmentDocument23 pagesEI competences predict cross-cultural adjustmentnatsumi18No ratings yet
- Neuroimagen y EmocionDocument10 pagesNeuroimagen y Emocionnatsumi18No ratings yet
- The ability to influence others via emotion displaysDocument20 pagesThe ability to influence others via emotion displaysnatsumi18No ratings yet
- Decisiones y Emociones AnticipadasDocument6 pagesDecisiones y Emociones Anticipadasnatsumi18No ratings yet
- InteliEmocion y ResoluProbleDocument17 pagesInteliEmocion y ResoluProblenatsumi18No ratings yet
- Games To Do You GoodDocument2 pagesGames To Do You GoodNeptün KırçiçekNo ratings yet
- Emocion y TomaDecisionDocument10 pagesEmocion y TomaDecisionnatsumi18No ratings yet
- Decisiones Sesgo NeuropshycologiaDocument11 pagesDecisiones Sesgo Neuropshycologianatsumi18No ratings yet
- Psychological General Wellbeing Index: January 2012Document6 pagesPsychological General Wellbeing Index: January 2012natsumi18No ratings yet
- Assessing Global Functioning with CGI ScalesDocument3 pagesAssessing Global Functioning with CGI Scalesnatsumi18No ratings yet
- Cognicion y NegociacionDocument287 pagesCognicion y Negociacionnatsumi18No ratings yet
- Self-Care Strategies for Frontline WorkersDocument45 pagesSelf-Care Strategies for Frontline Workersnatsumi18No ratings yet
- M01 S34 UNDP 2007 Gender Mainstreaming ToolkitDocument259 pagesM01 S34 UNDP 2007 Gender Mainstreaming Toolkitnatsumi18No ratings yet
- Child Neurology CBIT ReviewDocument5 pagesChild Neurology CBIT Reviewnatsumi18No ratings yet
- UMass Amherst Faculty Publishes Research on Adaptive Critics and Basal GangliaDocument20 pagesUMass Amherst Faculty Publishes Research on Adaptive Critics and Basal Ganglianatsumi18No ratings yet
- Evidencia Deprevencion AlzheimerDocument9 pagesEvidencia Deprevencion AlzheimerMarta Elena Díaz SotoNo ratings yet
- DeRuiteretal 2017Document21 pagesDeRuiteretal 2017natsumi18No ratings yet
- Derivation of Definition of Entropy: 1 Derivation of H (X) P P Log PDocument3 pagesDerivation of Definition of Entropy: 1 Derivation of H (X) P P Log Pnatsumi18No ratings yet
- Predicting The Visual WorldDocument2 pagesPredicting The Visual Worldnatsumi18No ratings yet
- EVAC Fund ToC and ME Narrative 20200615040610Document9 pagesEVAC Fund ToC and ME Narrative 20200615040610natsumi18No ratings yet
- An Optimal Estimation Approach To Visual Perception and LearningDocument27 pagesAn Optimal Estimation Approach To Visual Perception and Learningnatsumi18No ratings yet
- Soal Bahasa Inggris Kelas 5Document8 pagesSoal Bahasa Inggris Kelas 5imam hambaliNo ratings yet
- Penile Injection TherapyDocument4 pagesPenile Injection Therapydr NayanBharadwajNo ratings yet
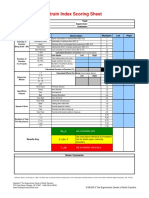
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- Hygiene Rules For Hotel Kitchen and Food Production StaffDocument3 pagesHygiene Rules For Hotel Kitchen and Food Production Staffvishnu nairNo ratings yet
- Young InfantDocument69 pagesYoung InfantAurora Doris BatagaNo ratings yet
- 210 419 1 SMDocument4 pages210 419 1 SMIneMeilaniNo ratings yet
- Hsmi Hudco TrainingDocument20 pagesHsmi Hudco TrainingThomas PeguNo ratings yet
- Kurukshetra University PhD Entrance Exam GuideDocument27 pagesKurukshetra University PhD Entrance Exam GuidemanojrkmNo ratings yet
- Nurs 5019 - Soap Note 41-60 Year OldDocument7 pagesNurs 5019 - Soap Note 41-60 Year Oldapi-308904543100% (1)
- BCS Class of DrugsDocument45 pagesBCS Class of DrugsLionO50% (2)
- 4.schedule Waste Management UTM - SWMP - 22mei2018 PDFDocument54 pages4.schedule Waste Management UTM - SWMP - 22mei2018 PDFfaraNo ratings yet
- Trays PDFDocument18 pagesTrays PDFBilal Hasan100% (1)
- Grizz Phys Tier 2 PDFDocument19 pagesGrizz Phys Tier 2 PDFJ VivianNo ratings yet
- Head To Toe Patient AssessmentDocument2 pagesHead To Toe Patient AssessmentJaypee Nuñez100% (2)
- Atkinson R L - Weight CyclingDocument7 pagesAtkinson R L - Weight CyclingmaddafackerNo ratings yet
- Annexure I: Block / Building Fire Safety Audit-Check List Fire Safety Audit ChecklistDocument5 pagesAnnexure I: Block / Building Fire Safety Audit-Check List Fire Safety Audit ChecklistGaurav Singh67% (3)
- Training Needs Analysis FormDocument4 pagesTraining Needs Analysis FormLizjasmine DimayaNo ratings yet
- CIS ParentDocument2 pagesCIS ParentAbegail (Abby) MirandaNo ratings yet
- VGEC 2024_Thư mời hội nghịDocument8 pagesVGEC 2024_Thư mời hội nghịkhongquantam101010No ratings yet
- Acute Respiratory Distress Syndrome: Jason D. Sciarretta, M.D. Critical Care Conference October 13, 2010Document24 pagesAcute Respiratory Distress Syndrome: Jason D. Sciarretta, M.D. Critical Care Conference October 13, 2010JelenaNo ratings yet
- Preface: Color Profile: Disabled Composite Default ScreenDocument2 pagesPreface: Color Profile: Disabled Composite Default ScreenCláudio CastroNo ratings yet
- Babu Jagjivan RamDocument24 pagesBabu Jagjivan RamAnonymous qFWInco8cNo ratings yet
- Couchiching FN Toll BoothDocument8 pagesCouchiching FN Toll BoothpegspirateNo ratings yet
- Pathological Urine ConstituentsDocument22 pagesPathological Urine Constituentsmanni1001100% (3)
- List of Beed Researchers 2 Semester SY 2020-2021 Beed-ADocument5 pagesList of Beed Researchers 2 Semester SY 2020-2021 Beed-AAndamin MalaNo ratings yet
- UKHO Survey Specification Acoustic V3 Jul18Document102 pagesUKHO Survey Specification Acoustic V3 Jul18Iqbal FauzanNo ratings yet
- Meat Inspection Certificate For Export of Pork/Pork Products To MalaysiaDocument2 pagesMeat Inspection Certificate For Export of Pork/Pork Products To MalaysiaLingSiewyingNo ratings yet
- Appendix7 I-131Document4 pagesAppendix7 I-131Crizzz001No ratings yet
- Pulmonary TB RadiologyDocument45 pagesPulmonary TB RadiologyArina Windri RivartiNo ratings yet
- Pothole Claim Form in PhiladelphiaDocument3 pagesPothole Claim Form in Philadelphiaphilly victorNo ratings yet