You might also like
- Robert WillnerAids DenialistDocument40 pagesRobert WillnerAids Denialistsibby11No ratings yet
- Cancer Cures Cancer Treatments That Work - Top 10 Natural Cancer TreatmentsDocument8 pagesCancer Cures Cancer Treatments That Work - Top 10 Natural Cancer TreatmentsDr. Dennis Clark100% (1)
- 9 Factors Cancer Miracle Survivors Have in CommonDocument1 page9 Factors Cancer Miracle Survivors Have in CommonSusan100% (1)
- Anaesthesia For Pancreatic SurgeryDocument11 pagesAnaesthesia For Pancreatic SurgeryDianita P Ñáñez VaronaNo ratings yet
- Biores CourseDocument43 pagesBiores CoursehldrmoneyNo ratings yet
- The FRCPath Exam - Paul BennettDocument130 pagesThe FRCPath Exam - Paul BennettVictor ChanNo ratings yet
- The Live Food FactorDocument903 pagesThe Live Food FactorCláudio Matos100% (1)
- Mms-Diseases and ProtocolDocument8 pagesMms-Diseases and ProtocolWeb Any100% (1)
- Health Benefits of Lavender Essential OilDocument6 pagesHealth Benefits of Lavender Essential OilNada PetrovićNo ratings yet
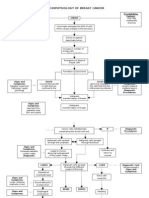
- Pathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsDocument3 pagesPathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsKevin Ercia100% (1)
- Neoadjuvant Chemoradiotherapy Followed by Surgery VersusDocument15 pagesNeoadjuvant Chemoradiotherapy Followed by Surgery VersusRaul Matute MartinNo ratings yet
- Liver Tumor Markers GuidelinesDocument64 pagesLiver Tumor Markers GuidelinesEyad KatrangiNo ratings yet
- 2017 Article 584Document6 pages2017 Article 584Victoria ViurcosNo ratings yet
- Kemoterapi THT 5Document8 pagesKemoterapi THT 5Niko Nofian NugrohoNo ratings yet
- Debiri 1Document12 pagesDebiri 1paquidermo85No ratings yet
- Gastric Ca With Peritoneal CarcinomatosisDocument11 pagesGastric Ca With Peritoneal Carcinomatosispaolo gasconNo ratings yet
- Postoperative - Adjuvant - Radiotherapy - HCCDocument11 pagesPostoperative - Adjuvant - Radiotherapy - HCCDinoop Korol PonnambathNo ratings yet
- Surgery For Early Stage Hepatocellular CarcinomaDocument9 pagesSurgery For Early Stage Hepatocellular CarcinomaAnthie FitriNo ratings yet
- Chemotherapy Plus Percutaneous Radiofrequency Ablation in Patients With Inoperable Colorectal Liver MetastasesDocument7 pagesChemotherapy Plus Percutaneous Radiofrequency Ablation in Patients With Inoperable Colorectal Liver MetastasesHaya RihanNo ratings yet
- Hepatocellular Carcinoma: The Need For Progress: Ournal of Linical NcologyDocument8 pagesHepatocellular Carcinoma: The Need For Progress: Ournal of Linical NcologyGetty InasNo ratings yet
- Simultaneous Versus Delayed Resection For Initially Resectable Synchronous Colorectal Cancer Liver MetastasesDocument8 pagesSimultaneous Versus Delayed Resection For Initially Resectable Synchronous Colorectal Cancer Liver MetastasesDr Shiv ChopraNo ratings yet
- الرسالة (Recovered)Document6 pagesالرسالة (Recovered)sonpolahmedNo ratings yet
- 19#prognostic HCC 2021Document7 pages19#prognostic HCC 2021hitashiNo ratings yet
- Children 06 00001 v2Document11 pagesChildren 06 00001 v2Nicolás Mosso F.No ratings yet
- Neoadjuvant Chemotherapy Vs Upfront Surgery For Gastric Signet Ring Cell Carcinoma A Retrospective, Propensity Score-Matched StudyDocument11 pagesNeoadjuvant Chemotherapy Vs Upfront Surgery For Gastric Signet Ring Cell Carcinoma A Retrospective, Propensity Score-Matched StudyLITTLESWEETKILLERNo ratings yet
- Criteria HCC 2011Document11 pagesCriteria HCC 2011commiekapurNo ratings yet
- Open Radiofrequency Ablation Combined With Splenectomy and Pericardial Devascularization Vs Liver Transplantation For Hepatocellular Carcinoma PDFDocument8 pagesOpen Radiofrequency Ablation Combined With Splenectomy and Pericardial Devascularization Vs Liver Transplantation For Hepatocellular Carcinoma PDFQotrunnada S SNo ratings yet
- Posthepatectomy Liver Failure: A Definition and Grading by The International Study Group of Liver Surgery (ISGLS)Document12 pagesPosthepatectomy Liver Failure: A Definition and Grading by The International Study Group of Liver Surgery (ISGLS)drsubramanianNo ratings yet
- Meta 6 - Khizar - 2023Document11 pagesMeta 6 - Khizar - 2023matheus.verasNo ratings yet
- Hepatic Arterial Anatomy Variations Evaluated by The Computedtomography Angiography in The Patients With Hepatocellular Carcinomaa 2167 7964 1000242Document6 pagesHepatic Arterial Anatomy Variations Evaluated by The Computedtomography Angiography in The Patients With Hepatocellular Carcinomaa 2167 7964 1000242Valir HusleNo ratings yet
- Cancers 13 01971Document19 pagesCancers 13 01971core6406No ratings yet
- HIFU For Palliative Treatment of Pancreatic CancerDocument11 pagesHIFU For Palliative Treatment of Pancreatic CancerpuchioNo ratings yet
- Jurnal Prognosis 2Document8 pagesJurnal Prognosis 2Chlarissa WahabNo ratings yet
- HPCDocument6 pagesHPCPrathita AmandaNo ratings yet
- Art Cancer Gastrico PDFDocument8 pagesArt Cancer Gastrico PDFvane_vane_tatyNo ratings yet
- Hepatectomy Versus Stereotactic Body Radiotherapy For Primary Early Hepatocellular Carcinoma A Propensity-Matched Analysis in A Single InstitutionDocument8 pagesHepatectomy Versus Stereotactic Body Radiotherapy For Primary Early Hepatocellular Carcinoma A Propensity-Matched Analysis in A Single Institutiondongjun daiNo ratings yet
- Multimodal Treatment of HCCDocument8 pagesMultimodal Treatment of HCCgrigmihNo ratings yet
- CD006039 AbstractDocument3 pagesCD006039 AbstractHeppyMeiNo ratings yet
- Role For Locoregional Therapies For Non-Colorectal Gastrointestinal MalignanciesDocument18 pagesRole For Locoregional Therapies For Non-Colorectal Gastrointestinal MalignanciesDR. SUMANTRA RAYNo ratings yet
- Shindoh 2013Document8 pagesShindoh 2013Nikos SerifisNo ratings yet
- Techniques of TIPS in The Treatment of Liver Cirrhosis Combined With Incompletely Occlusive Main Portal Vein ThrombosisDocument9 pagesTechniques of TIPS in The Treatment of Liver Cirrhosis Combined With Incompletely Occlusive Main Portal Vein ThrombosisLeon L GayaNo ratings yet
- Cholangiocarcinoma - A Review of The Literature and Future Directions in Therapy - HB SurgicalDocument12 pagesCholangiocarcinoma - A Review of The Literature and Future Directions in Therapy - HB SurgicalAnna MariaNo ratings yet
- Prognostic Factors and Survival in Patients With Gastric Stump CancerDocument8 pagesPrognostic Factors and Survival in Patients With Gastric Stump Cancerd33aNo ratings yet
- HPB 09 S2 071Document120 pagesHPB 09 S2 071Widya Dahlia JuwitaNo ratings yet
- Clinical Characteristics of Epithelioid Hemangioendothelioma: A Single-Center Retrospective StudyDocument8 pagesClinical Characteristics of Epithelioid Hemangioendothelioma: A Single-Center Retrospective StudyJose Huaman CamposNo ratings yet
- Locoregional Treatments Obsolete For Patients With Cancer With Liver MetastasesDocument18 pagesLocoregional Treatments Obsolete For Patients With Cancer With Liver MetastasesDR. SUMANTRA RAYNo ratings yet
- Medicine: Spontaneous Rupture of Solid Pseudopapillary Tumor of PancreasDocument8 pagesMedicine: Spontaneous Rupture of Solid Pseudopapillary Tumor of PancreasPatricia BezneaNo ratings yet
- 2017 Article 3322Document7 pages2017 Article 3322Kevin MandakNo ratings yet
- WBCprognosis Fujiwara2010Document6 pagesWBCprognosis Fujiwara2010Christofel JomanNo ratings yet
- Sub-Adventitial Divestment Technique For Resecting Artery-Involved Pancreatic Cancer: A Retrospective Cohort StudyDocument11 pagesSub-Adventitial Divestment Technique For Resecting Artery-Involved Pancreatic Cancer: A Retrospective Cohort StudyMatias Jurado ChaconNo ratings yet
- 2 PDFDocument10 pages2 PDFIka Kurniawan FaizinNo ratings yet
- Huang2020 Article ComparisonOfEmergencyCholecystDocument14 pagesHuang2020 Article ComparisonOfEmergencyCholecystLerdsin PlasticNo ratings yet
- SD Article 3Document6 pagesSD Article 3bogdanotiNo ratings yet
- Survival After Transarterial Embolization For Spontaneous Ruptured Hepatocellular CarcinomaDocument5 pagesSurvival After Transarterial Embolization For Spontaneous Ruptured Hepatocellular CarcinomaRollin SidaurukNo ratings yet
- FLOT 3 QuimioterapiaDocument8 pagesFLOT 3 Quimioterapiaerica corral corralNo ratings yet
- Tumor SeedingDocument10 pagesTumor SeedingQeis RamadhanNo ratings yet
- s13014 015 0495 4Document6 pagess13014 015 0495 4produxing 101No ratings yet
- BCAA Cancer MetaanalysisDocument11 pagesBCAA Cancer MetaanalysisSUFIAH MAIWIRMANo ratings yet
- Non-Hodgkin's Lymphoma of The Stomach: Treatment Outcomes For 57 Patients Over A 20-Year PeriodDocument5 pagesNon-Hodgkin's Lymphoma of The Stomach: Treatment Outcomes For 57 Patients Over A 20-Year PeriodpataraauliaNo ratings yet
- Atelektasis ParuDocument9 pagesAtelektasis ParuGigih PrakosoNo ratings yet
- 01 HepatogastroDocument3 pages01 Hepatogastroyacine26No ratings yet
- Hepatocellular Carcinoma 2009Document58 pagesHepatocellular Carcinoma 2009ctsakalakisNo ratings yet
- Long-Term Outcomes of Hepatitis B Virus-Related Cirrhosis Treated With Nucleos (T) Ide AnalogsDocument10 pagesLong-Term Outcomes of Hepatitis B Virus-Related Cirrhosis Treated With Nucleos (T) Ide AnalogsZulfiana NabilaNo ratings yet
- Neoadjuvant Chemoradiotherapy Plus Surgery Versus Surgery Alone For Oesophageal or Junctional Cancer (CROSS) Long-Term Results of A Randomised Controlled TrialDocument9 pagesNeoadjuvant Chemoradiotherapy Plus Surgery Versus Surgery Alone For Oesophageal or Junctional Cancer (CROSS) Long-Term Results of A Randomised Controlled TrialSergioNo ratings yet
- PB4 5920 R3Document22 pagesPB4 5920 R3Nicolás Mosso F.No ratings yet
- Prognostic Value and Adverse Events of Cytoreductive Surgery With Hyperthermic Intraperitoneal Chemotherapy in Primary Advanced and PlatinumDocument14 pagesPrognostic Value and Adverse Events of Cytoreductive Surgery With Hyperthermic Intraperitoneal Chemotherapy in Primary Advanced and PlatinumChris El HadiNo ratings yet
- Penatalaksanaan Medis CA Colon Stadium IIIDocument46 pagesPenatalaksanaan Medis CA Colon Stadium IIINadia Iriana DewiNo ratings yet
- Pone 0166157Document12 pagesPone 0166157cindydmjktNo ratings yet
- The Liver Graft Before Transplantation: Defining Outcome After Liver TransplantationFrom EverandThe Liver Graft Before Transplantation: Defining Outcome After Liver TransplantationXavier VerhelstNo ratings yet
- Hep 30Document4 pagesHep 30Andreea NicoletaNo ratings yet
- Hep 1Document6 pagesHep 1Andreea NicoletaNo ratings yet
- Case Presentation PediatricsDocument17 pagesCase Presentation PediatricsAndreea NicoletaNo ratings yet
- FullDocument13 pagesFullAndreea NicoletaNo ratings yet
- What Is A Lung CancerDocument3 pagesWhat Is A Lung CancerAdrian BsaerrdoeylaoMsaNo ratings yet
- Anti-Angiogenic Potential of Theobroma Cacao L. (Cacao) Seed Extract On Anas Platyrhynchos (Mallard Duck) EmbryoDocument41 pagesAnti-Angiogenic Potential of Theobroma Cacao L. (Cacao) Seed Extract On Anas Platyrhynchos (Mallard Duck) EmbryoJulienne Baldonado50% (2)
- 100 20210811 ICOPH 2021 Abstract BookDocument186 pages100 20210811 ICOPH 2021 Abstract Bookwafiq alibabaNo ratings yet
- Common Illnesses or DiseasesDocument17 pagesCommon Illnesses or Diseasesrosalyn gaboniNo ratings yet
- Diet and Physical Activity For Men With Prostate Cancer-IfmDocument20 pagesDiet and Physical Activity For Men With Prostate Cancer-Ifmapi-675909478No ratings yet
- A Review of The Ethnopharmacology, Phytochemistry and Pharmacology of Rauwolfia TetraphyllaDocument8 pagesA Review of The Ethnopharmacology, Phytochemistry and Pharmacology of Rauwolfia TetraphyllaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Poster Paper Foo Kota Bengkulu NewDocument1 pagePoster Paper Foo Kota Bengkulu NewPoppy WulandariNo ratings yet
- TP53 GeneDocument7 pagesTP53 GeneAlisson SantanaNo ratings yet
- Malignant Findings: Ductal Carcinoma in SituDocument12 pagesMalignant Findings: Ductal Carcinoma in SituNimeniNo ratings yet
- Abdomen & Pelvis Pathology - CT-scanDocument53 pagesAbdomen & Pelvis Pathology - CT-scanKeithKam100% (1)
- CDC: What You Need To Know About SmokingDocument2 pagesCDC: What You Need To Know About SmokingBen CulpepperNo ratings yet
- Cervical and Breast Cancer ScreeningDocument12 pagesCervical and Breast Cancer ScreeningIndonesian Journal of CancerNo ratings yet
- Care Oncology Clinic: Patient Information PackDocument4 pagesCare Oncology Clinic: Patient Information Packdave_scribedNo ratings yet
- September 15, Maple Ridge-Pitt Meadows NewsDocument33 pagesSeptember 15, Maple Ridge-Pitt Meadows NewsmapleridgenewsNo ratings yet
- 289-Article Text-1320-1-10-20070404Document4 pages289-Article Text-1320-1-10-20070404MisiingloveNo ratings yet
- A Case of Giant Pleomorphic Adenoma of The Parotid GlandDocument3 pagesA Case of Giant Pleomorphic Adenoma of The Parotid GlandmitaNo ratings yet
- Clitoral Carcinoma in 30 Yr Lady: A Case ReportDocument3 pagesClitoral Carcinoma in 30 Yr Lady: A Case ReportInternational Organization of Scientific Research (IOSR)No ratings yet
- Myths of U.S. HealthcareDocument3 pagesMyths of U.S. HealthcarecherylsealatlargeNo ratings yet
- Transcript of Medical Malpractice Delay in Diagnosis of Breast CancerDocument101 pagesTranscript of Medical Malpractice Delay in Diagnosis of Breast CancerAnthony T. DiPietroNo ratings yet
- Vitality Resource GuideDocument34 pagesVitality Resource GuideJason SmallNo ratings yet
- Hartalega Extreme Gloves - Sell Sheet - Colloidal Oatmeal Coated Nitrile Powder Free 2.5 MilDocument1 pageHartalega Extreme Gloves - Sell Sheet - Colloidal Oatmeal Coated Nitrile Powder Free 2.5 Milmfidae_210808925No ratings yet