You might also like
- Radiotherapy of Liver CancerFrom EverandRadiotherapy of Liver CancerJinsil SeongNo ratings yet
- Mehta Et Al-2018-American Journal of TransplantationDocument8 pagesMehta Et Al-2018-American Journal of Transplantationpaul00040No ratings yet
- Total Marrow Irradiation: A Comprehensive ReviewFrom EverandTotal Marrow Irradiation: A Comprehensive ReviewJeffrey Y. C. WongNo ratings yet
- Hepatectomy Versus Stereotactic Body Radiotherapy For Primary Early Hepatocellular Carcinoma A Propensity-Matched Analysis in A Single InstitutionDocument8 pagesHepatectomy Versus Stereotactic Body Radiotherapy For Primary Early Hepatocellular Carcinoma A Propensity-Matched Analysis in A Single Institutiondongjun daiNo ratings yet
- Rectal Cancer: International Perspectives on Multimodality ManagementFrom EverandRectal Cancer: International Perspectives on Multimodality ManagementBrian G. CzitoNo ratings yet
- Clinical Impact of External Radiotherapy in Non-Metastatic Esophageal Cancer According To Histopathological SubtypeDocument12 pagesClinical Impact of External Radiotherapy in Non-Metastatic Esophageal Cancer According To Histopathological SubtypesilviailieNo ratings yet
- Therapy Response Imaging in OncologyFrom EverandTherapy Response Imaging in OncologyMizuki NishinoNo ratings yet
- An Overview of Liver Directed Locoregional TherapiesDocument21 pagesAn Overview of Liver Directed Locoregional TherapiesDR. SUMANTRA RAYNo ratings yet
- AsdasdDocument10 pagesAsdasdAdhi PratamaNo ratings yet
- Dhondt Et Al 2022 90y Radioembolization Versus Drug Eluting Bead Chemoembolization For Unresectable HepatocellularDocument12 pagesDhondt Et Al 2022 90y Radioembolization Versus Drug Eluting Bead Chemoembolization For Unresectable HepatocellularNachchakorn DellNo ratings yet
- Debiri 1Document12 pagesDebiri 1paquidermo85No ratings yet
- Articulo de RevisiónDocument8 pagesArticulo de RevisiónDranmvmNo ratings yet
- EBRT in DTCDocument7 pagesEBRT in DTCElena FlorentinaNo ratings yet
- Surgery For Early Stage Hepatocellular CarcinomaDocument9 pagesSurgery For Early Stage Hepatocellular CarcinomaAnthie FitriNo ratings yet
- Vera2020 Article MultidisciplinaryManagementOfLDocument16 pagesVera2020 Article MultidisciplinaryManagementOfLDiego Andres VasquezNo ratings yet
- J HPB 2016 02 489Document2 pagesJ HPB 2016 02 489hud6427No ratings yet
- Improved Outcome by Adding Concurrent Chemotherapy ToDocument9 pagesImproved Outcome by Adding Concurrent Chemotherapy ToRaul Matute MartinNo ratings yet
- 2017 Article 584Document6 pages2017 Article 584Victoria ViurcosNo ratings yet
- 8424365Document8 pages8424365Melody CyyNo ratings yet
- Comparison of Radical Cystectomy With Conservative Treatment in Geriatric ( 80) Patients With Muscle-Invasive Bladder CancerDocument9 pagesComparison of Radical Cystectomy With Conservative Treatment in Geriatric ( 80) Patients With Muscle-Invasive Bladder CancerjustforuroNo ratings yet
- TouijerDocument7 pagesTouijerVinko GrubišićNo ratings yet
- FLOT 3 QuimioterapiaDocument8 pagesFLOT 3 Quimioterapiaerica corral corralNo ratings yet
- Cover Refleksi KasusDocument10 pagesCover Refleksi Kasusnadiabella_No ratings yet
- 6 Postoperative Radiation Therapy in The Management of Head and Neck Cancer - UpToDateDocument16 pages6 Postoperative Radiation Therapy in The Management of Head and Neck Cancer - UpToDateMarco GornattiNo ratings yet
- Criteria HCC 2011Document11 pagesCriteria HCC 2011commiekapurNo ratings yet
- BladderDocument36 pagesBladderdrsumitavaNo ratings yet
- Clinical Efficacy of Stereotactic Ablative RadiothDocument8 pagesClinical Efficacy of Stereotactic Ablative RadiothuswahsnddinNo ratings yet
- Acs 06 02 152Document7 pagesAcs 06 02 152crsscribdNo ratings yet
- 2018 Article 6554Document8 pages2018 Article 6554Raíla SoaresNo ratings yet
- Neoadjuvant Chemoradiotherapy Followed by Surgery VersusDocument15 pagesNeoadjuvant Chemoradiotherapy Followed by Surgery VersusRaul Matute MartinNo ratings yet
- Kemoterapi THT 5Document8 pagesKemoterapi THT 5Niko Nofian NugrohoNo ratings yet
- Heymach-2022-Design and Rationale For A Phase1Document5 pagesHeymach-2022-Design and Rationale For A Phase1Luca BertolacciniNo ratings yet
- A Risk-Adapted Approach To The Use of Radioactive Iodine and External Beam Radiation in The Treatment of Well-Differentiated Thyroid CancerDocument7 pagesA Risk-Adapted Approach To The Use of Radioactive Iodine and External Beam Radiation in The Treatment of Well-Differentiated Thyroid Cancerdalton95198285No ratings yet
- Shindoh 2013Document8 pagesShindoh 2013Nikos SerifisNo ratings yet
- Essentials of Thoracic ImagingDocument158 pagesEssentials of Thoracic ImagingMohammed NoemanNo ratings yet
- Transarterial Chemoembolization: Modalities, Indication, and Patient SelectionDocument9 pagesTransarterial Chemoembolization: Modalities, Indication, and Patient SelectionJosseph EscobarNo ratings yet
- Targeted Percutaneous Microwave Ablation at The Pulmonary Lesion Combined With Mediastinal Radiotherapy With or Without Concurrent Chemotherapy inDocument8 pagesTargeted Percutaneous Microwave Ablation at The Pulmonary Lesion Combined With Mediastinal Radiotherapy With or Without Concurrent Chemotherapy inMalekseuofi مالك السيوفيNo ratings yet
- 10 1111@codi 15424Document22 pages10 1111@codi 15424yongky sugandaNo ratings yet
- Liver Transplantation - 2016 - Dioguardi Burgio - Correlation of Tumor Response On Computed Tomography With PathologicalDocument10 pagesLiver Transplantation - 2016 - Dioguardi Burgio - Correlation of Tumor Response On Computed Tomography With Pathologicaldahiheg756No ratings yet
- Hep 49Document5 pagesHep 49Andreea NicoletaNo ratings yet
- CA GastricDocument9 pagesCA GastricmonikNo ratings yet
- The OncologistDocument7 pagesThe OncologistManunart FeungpeanNo ratings yet
- Rectal CancerDocument4 pagesRectal CancerAlice AugustinNo ratings yet
- Kanker Ovarium 2 PDFDocument6 pagesKanker Ovarium 2 PDFhestiNo ratings yet
- 2016 Article 826Document6 pages2016 Article 826tomniucNo ratings yet
- HPCDocument6 pagesHPCPrathita AmandaNo ratings yet
- Watanabe2020 Article RecentProgressInMultidisciplinDocument9 pagesWatanabe2020 Article RecentProgressInMultidisciplinJose Huaman CamposNo ratings yet
- Kanker ParuDocument10 pagesKanker Parunovi hidayahNo ratings yet
- Accreditation Statement: Target Audience: This Activity Is Designed To Meet The Educational Needs of Physicians, NursesDocument13 pagesAccreditation Statement: Target Audience: This Activity Is Designed To Meet The Educational Needs of Physicians, NursesLaras FariadiNo ratings yet
- Patient Selection Criteria For Selective InternalDocument5 pagesPatient Selection Criteria For Selective InternalLuthienFreyNo ratings yet
- Impact of Time To Surgery After Neoadjuvant Chemotherapy in Operable Breast Cancer PatientsDocument6 pagesImpact of Time To Surgery After Neoadjuvant Chemotherapy in Operable Breast Cancer PatientsPani lookyeeNo ratings yet
- Secondary Cytoreduction Surgery Improves Prognosis in Platinum-Sensitive Recurrent Ovarian CancerDocument6 pagesSecondary Cytoreduction Surgery Improves Prognosis in Platinum-Sensitive Recurrent Ovarian CancerMay SirinanNo ratings yet
- The Optimal Neoadjuvant Treatment of Locally Advanced Esophageal CancerDocument11 pagesThe Optimal Neoadjuvant Treatment of Locally Advanced Esophageal CancerdjonesthoracicNo ratings yet
- s13014 015 0495 4Document6 pagess13014 015 0495 4produxing 101No ratings yet
- 1 s2.0 S0748798324003974 MainDocument1 page1 s2.0 S0748798324003974 MainShahnaz AhmedNo ratings yet
- Wo2019 PosterDocument1 pageWo2019 PosterCx Tx HRTNo ratings yet
- Concurrent Radiotherapy and Weekly Paclitaxel For Locally Advanced Squmous Cell Carcinoma of Uterine Cervix-Treated Patients at Rural Centre in IndiaDocument5 pagesConcurrent Radiotherapy and Weekly Paclitaxel For Locally Advanced Squmous Cell Carcinoma of Uterine Cervix-Treated Patients at Rural Centre in IndiaIjsrnet EditorialNo ratings yet
- Effect of Visceral Adipose Tissue On The AccuracyDocument8 pagesEffect of Visceral Adipose Tissue On The AccuracyMaria GoretiNo ratings yet
- Updates in Management of Ampullary Carcinomas: Highlight ArticleDocument4 pagesUpdates in Management of Ampullary Carcinomas: Highlight Articlecorinna291No ratings yet
- Esmo Guidline: Presentasi Oleh: Dr.I Nyoman Dwija Putra SP.BDocument45 pagesEsmo Guidline: Presentasi Oleh: Dr.I Nyoman Dwija Putra SP.BIrbah NabilaNo ratings yet
- Rectal CancerDocument6 pagesRectal CancerIqra FatemahNo ratings yet
- Signs and Symptoms: Colorectal Cancer, Also Called Colon Cancer or Large Bowel Cancer, IncludesDocument18 pagesSigns and Symptoms: Colorectal Cancer, Also Called Colon Cancer or Large Bowel Cancer, Includesphvega06No ratings yet
- Sinonasal Undifferentiated Carcinoma (SNUC)Document13 pagesSinonasal Undifferentiated Carcinoma (SNUC)Anonymous VTZ0bL5Od7No ratings yet
- Ovarian Cancer Treatment Regimens - Print Article - Cancer Therapy AdvisorDocument5 pagesOvarian Cancer Treatment Regimens - Print Article - Cancer Therapy AdvisorAnonymous g1hIPZNo ratings yet
- Powerpoint: Breast CancerDocument89 pagesPowerpoint: Breast Cancerj.doe.hex_8780% (5)
- Augmenting Effect of Hyperthermia in Neoadjuvant Chemotherapy For Advanced Breast Cancer - A Case ReportDocument3 pagesAugmenting Effect of Hyperthermia in Neoadjuvant Chemotherapy For Advanced Breast Cancer - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Woman With Postmenopausal Bleeding: Gynaecological MalignanciesDocument5 pagesThe Woman With Postmenopausal Bleeding: Gynaecological MalignanciesWahyu AriyawatiNo ratings yet
- Colon CancerDocument25 pagesColon Cancerchori2008No ratings yet
- Advanced Cancer. Pain and Quality of LifeDocument356 pagesAdvanced Cancer. Pain and Quality of Lifestrahiltodorov100% (1)
- 2004 PublicationsDocument89 pages2004 PublicationsMochamad Hasim AsariNo ratings yet
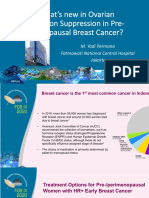
- 2.3.a DR Yadi Permana Whats New in Ovarian Function Suppression in Pre-MenopausalDocument36 pages2.3.a DR Yadi Permana Whats New in Ovarian Function Suppression in Pre-Menopausaltepat rshsNo ratings yet
- Phesgo Patient Quick HitDocument32 pagesPhesgo Patient Quick HitTarun ChakrabortyNo ratings yet
- Current Cancer Treatment - Novel Beyond Conventional ApproachesDocument826 pagesCurrent Cancer Treatment - Novel Beyond Conventional Approacheselenac67100% (1)
- 50 Big Debates in Gynecologic Oncology (2023) - Dennis S. ChiDocument351 pages50 Big Debates in Gynecologic Oncology (2023) - Dennis S. ChiGardener Ayu100% (2)
- Temozolomide Adjuvant NHSDocument5 pagesTemozolomide Adjuvant NHSSyed Touseef AhmedNo ratings yet
- Ghaith Heilat, MD, MS, FEBS, FACS Breast, Endocrine and General Surgeon Faculty of Medicine/ Yarmouk UniversityDocument76 pagesGhaith Heilat, MD, MS, FEBS, FACS Breast, Endocrine and General Surgeon Faculty of Medicine/ Yarmouk UniversityBalqees abusahuonNo ratings yet
- Gynecol. 2009 113:1417-1418.: National Cancer Institute "Metastatic Cancer: Questions and Answers"Document5 pagesGynecol. 2009 113:1417-1418.: National Cancer Institute "Metastatic Cancer: Questions and Answers"Vanshika SharmaNo ratings yet
- Pancreatic Cancer Oxford SurgeryDocument10 pagesPancreatic Cancer Oxford SurgeryJose Tomás MooreNo ratings yet
- ChemotherapyDocument102 pagesChemotherapyJoseph John K Pothanikat100% (1)
- Updates On The Treatment of Pterygium: Serbian Journal of Experimental and Clinical Research September 2016Document7 pagesUpdates On The Treatment of Pterygium: Serbian Journal of Experimental and Clinical Research September 2016Arfadin YusufNo ratings yet
- Ismail Benson John Sbitany Hani Jatoi - Atlas of Breast Surgery.-Springer Nature (2020)Document137 pagesIsmail Benson John Sbitany Hani Jatoi - Atlas of Breast Surgery.-Springer Nature (2020)Zain AlmajaliNo ratings yet
- Clinical Practice Guidelines For The Diagnosis and Treatment of Patients With Soft Tissue Sarcoma by The Spanish Group For Research in Sarcomas (GEIS)Document14 pagesClinical Practice Guidelines For The Diagnosis and Treatment of Patients With Soft Tissue Sarcoma by The Spanish Group For Research in Sarcomas (GEIS)carolinapolotorresNo ratings yet
- Breast Cancer Screening: Screening Management:: A. DciDocument1 pageBreast Cancer Screening: Screening Management:: A. DciCharlie65129No ratings yet
- ChemotherapyDocument35 pagesChemotherapynikhl saulNo ratings yet
- Sarcomas Glandula MamariaDocument6 pagesSarcomas Glandula MamariaNelly ChacónNo ratings yet
- Brain Tumor Imaging - 2016Document166 pagesBrain Tumor Imaging - 2016Vĩ Đặng100% (2)
- Redondo Drug Study PaclitaxelDocument4 pagesRedondo Drug Study PaclitaxelPaul Audrey RedondoNo ratings yet
- Vulvar Cancer: (Squamous Cell Carcinoma)Document60 pagesVulvar Cancer: (Squamous Cell Carcinoma)nuvitaNo ratings yet
- Adjuvant ChemotheraphyDocument10 pagesAdjuvant ChemotheraphyFatona AgungNo ratings yet
- Sgop 2012Document108 pagesSgop 2012PhoebeKatezPiedraCampasasNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (79)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)