You might also like
- Computerised Payroll Practice Set Using MYOB AccountRight: Australian EditionFrom EverandComputerised Payroll Practice Set Using MYOB AccountRight: Australian EditionNo ratings yet
- Agara Mallegowda MalleshDocument4 pagesAgara Mallegowda MalleshRamesh BabuNo ratings yet
- Policy DocumentDocument4 pagesPolicy Documentnizamsagar tsgencoNo ratings yet
- Policy ScheduleDocument4 pagesPolicy ScheduleacrajeshNo ratings yet
- Policy DocDocument4 pagesPolicy Dochiteshmohakar15No ratings yet
- PVS Lakshmiprasad: ImportantDocument5 pagesPVS Lakshmiprasad: ImportantRamesh BabuNo ratings yet
- Health Insurance PolicyDocument8 pagesHealth Insurance PolicyAnant KumarNo ratings yet
- Policy ScheduleDocument4 pagesPolicy ScheduleTECH IN BANGLANo ratings yet
- G.dinesh KumarDocument4 pagesG.dinesh KumarSrinivasan NarasimhanNo ratings yet
- Policy DocumentDocument9 pagesPolicy DocumentMahesh ShindeNo ratings yet
- Renewal NoticeDocument2 pagesRenewal NoticeMuzammil KhanNo ratings yet
- Ravi of Medical Insurance - Self - 2023Document8 pagesRavi of Medical Insurance - Self - 2023Cut Copy PateNo ratings yet
- Health Insurance Policy SUBHRANILDocument1 pageHealth Insurance Policy SUBHRANILsubhranil1No ratings yet
- Health Ins ReceiptDocument3 pagesHealth Ins ReceiptAayush KaulNo ratings yet
- Star HealthDocument4 pagesStar Healthsom kumarNo ratings yet
- Policy DocDocument4 pagesPolicy DocSachin PawarNo ratings yet
- Policy DocDocument5 pagesPolicy Docjafarali3061971No ratings yet
- P 131124 01 2023 008806 Policy DocDocument4 pagesP 131124 01 2023 008806 Policy DockasturihospitalsecunderabadNo ratings yet
- Mahadeb Karmakar Health Policy 2023 - RenewalDocument4 pagesMahadeb Karmakar Health Policy 2023 - Renewaljobs.somabho.kNo ratings yet
- Health Insurance 1Document1 pageHealth Insurance 1shivarkp88No ratings yet
- Policy DocDocument5 pagesPolicy DocRahul ShawNo ratings yet
- Health InsuranceDocument7 pagesHealth InsuranceRadhika Rampal100% (1)
- Policy DocDocument4 pagesPolicy DocAb de VilliersNo ratings yet
- Policy DocDocument4 pagesPolicy Dockiran gadheNo ratings yet
- LILI Karmakar Health Policy 2023Document4 pagesLILI Karmakar Health Policy 2023jobs.somabho.kNo ratings yet
- DS Policy Schedule 11250842406703 V1.0Document6 pagesDS Policy Schedule 11250842406703 V1.0citd trainingNo ratings yet
- Sumanth - Medical Insurance-ParentsDocument2 pagesSumanth - Medical Insurance-ParentsMohan kishoreNo ratings yet
- PolicyDocument4 pagesPolicyPrashant mhamunkarNo ratings yet
- Renewal Notice-5hshsDocument2 pagesRenewal Notice-5hshsHshshsvd hdhdNo ratings yet
- Policy DocDocument4 pagesPolicy DocVisheshNo ratings yet
- DS Policy Schedule 11230074563901 V1.0Document5 pagesDS Policy Schedule 11230074563901 V1.0Soorya ArunthavamNo ratings yet
- DS Policy Schedule 11230207673409 V1.0Document4 pagesDS Policy Schedule 11230207673409 V1.0Rajesh KsmNo ratings yet
- Star HealthDocument1 pageStar HealthpalanivelNo ratings yet
- Policy DocDocument3 pagesPolicy Dochiteshmohakar15No ratings yet
- Rwservlet PDFDocument4 pagesRwservlet PDFBhavya AhirNo ratings yet
- Nitesh 2022-23Document4 pagesNitesh 2022-23shambhuk2009No ratings yet
- PolicyDocument8 pagesPolicyjoshiaruna539No ratings yet
- Policy ScheduleDocument4 pagesPolicy ScheduleArvind BajpaiNo ratings yet
- ENDT07Document1 pageENDT07sushil kumarNo ratings yet
- Policy ScheduleDocument6 pagesPolicy ScheduleNITIN SHARMANo ratings yet
- Health Insurance PolicyDocument5 pagesHealth Insurance Policytaralsoni100% (4)
- Renewal NoticeDocument2 pagesRenewal NoticeSurinder PahwaNo ratings yet
- Renewal NoticeDocument2 pagesRenewal NoticeSai Kiran KodipyakaNo ratings yet
- Renewal Notice: Policy No.P/141126/01/2019/003982Document1 pageRenewal Notice: Policy No.P/141126/01/2019/003982manoharNo ratings yet
- Policy Schedule 3Document4 pagesPolicy Schedule 3star xeroxNo ratings yet
- Renewal Notice: Policy No.P/131112/01/2019/007048Document1 pageRenewal Notice: Policy No.P/131112/01/2019/007048mkm969No ratings yet
- Renewal NoticeDocument2 pagesRenewal NoticeSurya PrakashNo ratings yet
- Renewal NoticeDocument2 pagesRenewal NoticerajaNo ratings yet
- Policy DocDocument6 pagesPolicy DocSoma Shekar ANo ratings yet
- Policy DocDocument6 pagesPolicy Docce mgnregsNo ratings yet
- Policy Doc PDFDocument5 pagesPolicy Doc PDFprashantNo ratings yet
- One ThreeDocument5 pagesOne ThreeNaveen PNo ratings yet
- 2021-22 Star Health InsuranceDocument5 pages2021-22 Star Health InsurancePuthu Raja SevugapandianNo ratings yet
- Policy DocDocument4 pagesPolicy DocRaghav SharmaNo ratings yet
- Policy DocDocument6 pagesPolicy DocmaterialNo ratings yet
- Policy 417815024Document5 pagesPolicy 417815024MuraliMohanNo ratings yet
- Policy DocDocument4 pagesPolicy DocDrBiswajaya SharmaNo ratings yet
- Policy ScheduleDocument4 pagesPolicy ScheduleSannik APNo ratings yet
- Policy DocDocument3 pagesPolicy DocVishalNo ratings yet
- BA0000135013 Intermediary Code Name Phone No E-Mail Id: 55 K. Madan Prakash K. Madan Prakash 4/51, Pesil Garden, KovurDocument1 pageBA0000135013 Intermediary Code Name Phone No E-Mail Id: 55 K. Madan Prakash K. Madan Prakash 4/51, Pesil Garden, Kovurmy9884583870No ratings yet
- Tpl-Yiapl-Ph1&2-An-38 R0Document1 pageTpl-Yiapl-Ph1&2-An-38 R0Ramesh BabuNo ratings yet
- Tpl-Yiapl-Ph1&2-An-39 R0Document1 pageTpl-Yiapl-Ph1&2-An-39 R0Ramesh BabuNo ratings yet
- Tpl-Yiapl-Ph1&2-An-40 R0Document1 pageTpl-Yiapl-Ph1&2-An-40 R0Ramesh BabuNo ratings yet
- Plan For Removing ARFF's Impacted Temporary Retaining WallDocument3 pagesPlan For Removing ARFF's Impacted Temporary Retaining WallRamesh BabuNo ratings yet
- Tpl-Yiapl-Ph1&2-An-35 R1Document1 pageTpl-Yiapl-Ph1&2-An-35 R1Ramesh BabuNo ratings yet
- Tpl-Yiapl-Ph1&2-An-34 R0Document1 pageTpl-Yiapl-Ph1&2-An-34 R0Ramesh BabuNo ratings yet
- Tpl-Yiapl-Ph1&2-An-27 R0Document1 pageTpl-Yiapl-Ph1&2-An-27 R0Ramesh BabuNo ratings yet
- Tpl-Yiapl-Ph1&2-An-14 R0Document1 pageTpl-Yiapl-Ph1&2-An-14 R0Ramesh BabuNo ratings yet
- Tpl-Yiapl-Ph1&2-An-15 R1Document1 pageTpl-Yiapl-Ph1&2-An-15 R1Ramesh BabuNo ratings yet
- Tpl-Yiapl-Ph1&2-An-16 R1Document1 pageTpl-Yiapl-Ph1&2-An-16 R1Ramesh BabuNo ratings yet
- Podipireddi Srihari - ResumeDocument4 pagesPodipireddi Srihari - ResumeRamesh BabuNo ratings yet
- Tpl-Yiapl-Ph1&2-An-18 R0Document1 pageTpl-Yiapl-Ph1&2-An-18 R0Ramesh BabuNo ratings yet
- Appendix - 9 - List of MakesDocument105 pagesAppendix - 9 - List of MakesRamesh BabuNo ratings yet
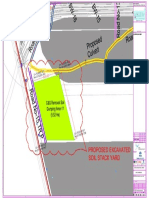
- 02 - Proposed Excavated Soil Stack YardDocument1 page02 - Proposed Excavated Soil Stack YardRamesh BabuNo ratings yet
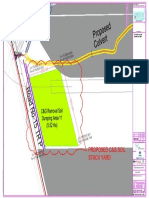
- 02 - Proposed C&G Soil Stack YardDocument1 page02 - Proposed C&G Soil Stack YardRamesh BabuNo ratings yet
- Appendix - 6 - Site Logistics PlanDocument16 pagesAppendix - 6 - Site Logistics PlanRamesh BabuNo ratings yet
- Appendix - 3 - Progress ReportingDocument9 pagesAppendix - 3 - Progress ReportingRamesh BabuNo ratings yet
- Appendix - 9 - List of MakesDocument71 pagesAppendix - 9 - List of MakesRamesh BabuNo ratings yet
- Wa0000.Document16 pagesWa0000.Ramesh BabuNo ratings yet
- PI Sheet AR26 - 6 - 042 3,5kNDocument1 pagePI Sheet AR26 - 6 - 042 3,5kNRamesh BabuNo ratings yet
- Final Uds Sukkur With AddendumDocument463 pagesFinal Uds Sukkur With AddendumAtifKhanNo ratings yet
- Quomundo LTD - Brochure-RevDocument14 pagesQuomundo LTD - Brochure-RevHeryanto GeoNo ratings yet
- "Turning Glove From GOLD To DIAMOND": Supermax Corporation Berhad Analyst Briefing Slides 4Q'2020 RESULTSDocument35 pages"Turning Glove From GOLD To DIAMOND": Supermax Corporation Berhad Analyst Briefing Slides 4Q'2020 RESULTSmroys mroysNo ratings yet
- Ichimoku (AATI)Document22 pagesIchimoku (AATI)Anthony FuNo ratings yet
- Unit 3 - Security AnalysisDocument33 pagesUnit 3 - Security AnalysisWasim DalviNo ratings yet
- Module 3 Debt ManagementDocument33 pagesModule 3 Debt ManagementJane BañaresNo ratings yet
- Athol Furniture, IncDocument21 pagesAthol Furniture, Incvinoth kumar0% (1)
- College"Giants of An Earlier Capitalism": The Chartered Trading Companies As Modern MultinationalsDocument23 pagesCollege"Giants of An Earlier Capitalism": The Chartered Trading Companies As Modern MultinationalsTodd BurstNo ratings yet
- Weele.5th Ed - Chapter 01.2010Document19 pagesWeele.5th Ed - Chapter 01.2010ravin100% (1)
- The Scope and Challenge of International MarketingDocument24 pagesThe Scope and Challenge of International MarketingBetty NiamienNo ratings yet
- The New Economic Geography Theory by Paul Krugman and Our Proposed Economic TheoryDocument36 pagesThe New Economic Geography Theory by Paul Krugman and Our Proposed Economic TheoryEulalio NinaNo ratings yet
- Acc106 Rubrics For Assignment - For Student RefDocument2 pagesAcc106 Rubrics For Assignment - For Student RefItik BerendamNo ratings yet
- Role of Digital MarketingDocument2 pagesRole of Digital MarketingUrmi ThadaniNo ratings yet
- Subway Creates Value For Customers Through Co-Creation. How Do You Describe The Profit Chain of The Subway?Document5 pagesSubway Creates Value For Customers Through Co-Creation. How Do You Describe The Profit Chain of The Subway?Atika AsadNo ratings yet
- M222994Document5 pagesM222994Carlos Takudzwa MudzengerereNo ratings yet
- Foundations of Engineering EconomyDocument62 pagesFoundations of Engineering EconomyMuhammad AmmarNo ratings yet
- Bim MercubuanaDocument19 pagesBim MercubuanaWallArsitekNewsNo ratings yet
- Tendernotice - 1 - 2020-09-27T221316.129 PDFDocument426 pagesTendernotice - 1 - 2020-09-27T221316.129 PDFPratik GuptaNo ratings yet
- Chapter 15 Test Bank Partnerships - Formation, Operations, and Changes in Ownership InterestsDocument22 pagesChapter 15 Test Bank Partnerships - Formation, Operations, and Changes in Ownership InterestsOBC LingayenNo ratings yet
- Factors Affecting Customer Satisfaction in The Fast Food Restaurants of KathmanduDocument11 pagesFactors Affecting Customer Satisfaction in The Fast Food Restaurants of KathmanduRoshanNo ratings yet
- Classification of Engineering ServicesDocument24 pagesClassification of Engineering ServicesPaul Vincent De GuzmanNo ratings yet
- MCQ SFM TybbaDocument6 pagesMCQ SFM TybbaDK FashionNo ratings yet
- Population Pyramid: Pyramid", Is A Graphical Illustration That Shows TheDocument7 pagesPopulation Pyramid: Pyramid", Is A Graphical Illustration That Shows TheUsmanNo ratings yet
- Tubo FSDocument7 pagesTubo FSdemonjoeNo ratings yet
- DerivDocument47 pagesDerivMahesh SabharwalNo ratings yet
- PCS Model Explained 278Document6 pagesPCS Model Explained 278maged_abdnaghoNo ratings yet
- TQM and QFDDocument19 pagesTQM and QFDtashapa100% (1)
- Lesson 3:: Total Quality Management PrincipleDocument17 pagesLesson 3:: Total Quality Management PrincipleJolina CabardoNo ratings yet
- LEAN Production or Lean Manufacturing or Toyota Production System (TPS) - Doing More With Less (Free Business E-Coach)Document4 pagesLEAN Production or Lean Manufacturing or Toyota Production System (TPS) - Doing More With Less (Free Business E-Coach)Amanpreet Singh AroraNo ratings yet
- Icaew Cfab Mi 2018 Sample Exam 3Document30 pagesIcaew Cfab Mi 2018 Sample Exam 3Anonymous ulFku1v100% (2)