0% found this document useful (0 votes)
135 views4 pagesOfficial Business and Leave Forms
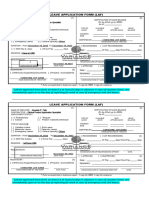
This document contains an official business slip, application for leave form, overtime approval request form, and service report form used by a company. The forms collect information such as employee name, dates and times, purpose or nature of official business, leave details, overtime hours requested, and service details to document work-related activities.
Uploaded by
Rhex TVCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
135 views4 pagesOfficial Business and Leave Forms
This document contains an official business slip, application for leave form, overtime approval request form, and service report form used by a company. The forms collect information such as employee name, dates and times, purpose or nature of official business, leave details, overtime hours requested, and service details to document work-related activities.
Uploaded by
Rhex TVCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd