You might also like
- Update On (Approach To) Anemia1 (Changes)Document39 pagesUpdate On (Approach To) Anemia1 (Changes)Balchand KukrejaNo ratings yet
- Transfusion in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaDocument41 pagesTransfusion in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaAETCM Emergency medicineNo ratings yet
- 1 - Coating Solutions For Centrifugal Compressor Fouling (LR)Document4 pages1 - Coating Solutions For Centrifugal Compressor Fouling (LR)Mokhammad Fahmi Izdiharrudin100% (1)
- GSM Network SDCCH Congestion & Solutions-16Document15 pagesGSM Network SDCCH Congestion & Solutions-16abdullaaNo ratings yet
- Final Examination Rubric On The Zumba Exercises RoutineDocument1 pageFinal Examination Rubric On The Zumba Exercises RoutinePizzaTobacco123100% (1)
- Chapter 08 - Ion Exchange, Water Demineralization & Resin TestingDocument23 pagesChapter 08 - Ion Exchange, Water Demineralization & Resin TestingMohamed ElbehlilNo ratings yet
- Using SSPC Coating Material Standards 1Document18 pagesUsing SSPC Coating Material Standards 1achusanachu100% (1)
- Metabolism and AtpDocument20 pagesMetabolism and AtpAbdul Rafay ShaikhNo ratings yet
- EPO in Anemia CHFDocument10 pagesEPO in Anemia CHFAlizaPinkyNo ratings yet
- 3 - 8 - Uromodulin - JHyperten Ok-1Document10 pages3 - 8 - Uromodulin - JHyperten Ok-1Linda MaylianaNo ratings yet
- Paternostro 2020Document9 pagesPaternostro 2020my accountNo ratings yet
- ANEMIA P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document7 pagesANEMIA P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Arv IraNo ratings yet
- Prevalence of Anemia in Patients With Heart Failure: Edition: 29.1 - 12 Article(s)Document13 pagesPrevalence of Anemia in Patients With Heart Failure: Edition: 29.1 - 12 Article(s)Novia KurniantiNo ratings yet
- Anem 2Document6 pagesAnem 2vamiqrasoolNo ratings yet
- Iron Deficiency in Heart Failure: An OverviewDocument11 pagesIron Deficiency in Heart Failure: An OverviewFelipe SennNo ratings yet
- Anaemia, Iron Deficiency and Heart Failure in 2020 - Facts and NumbersDocument5 pagesAnaemia, Iron Deficiency and Heart Failure in 2020 - Facts and NumbersAriadna Barreto100% (1)
- A Systematic Review of Physical Activity in People With Haemophilia and Its Relationship With Bleeding Phenotype and Treatment RegimenDocument19 pagesA Systematic Review of Physical Activity in People With Haemophilia and Its Relationship With Bleeding Phenotype and Treatment RegimenDiogo GadelhaNo ratings yet
- HD 1Document7 pagesHD 1Arista RachmaNo ratings yet
- Clinical ResearchDocument6 pagesClinical Researchnurul wahyuniNo ratings yet
- Armstrong 2017 Diabetic Foot Ulcers and Their RecurrenceDocument11 pagesArmstrong 2017 Diabetic Foot Ulcers and Their Recurrencefebyan yohanesNo ratings yet
- Ferric Carboxymaltose in Patients With Heart Failure and Iron DeficiencyDocument13 pagesFerric Carboxymaltose in Patients With Heart Failure and Iron DeficiencyfathaNo ratings yet
- Ferreiro Et Al 2016Document18 pagesFerreiro Et Al 2016nurminsyahNo ratings yet
- Long-Term Outcomes of Lercanidipine Versus Other Calcium Channel Blockers in Newly Diagnosed Hypertension: A Nationwide Cohort StudyDocument8 pagesLong-Term Outcomes of Lercanidipine Versus Other Calcium Channel Blockers in Newly Diagnosed Hypertension: A Nationwide Cohort StudyApt. Mulyadi PrasetyoNo ratings yet
- Tema 2 Mortality in Kidney Disease Patients TreatedDocument9 pagesTema 2 Mortality in Kidney Disease Patients TreatedRomaniuc IuliaNo ratings yet
- Ehac 569Document14 pagesEhac 569Binod KumarNo ratings yet
- Diabetes Mellitus and Heart Failure 2017 The American Journal of MedicineDocument11 pagesDiabetes Mellitus and Heart Failure 2017 The American Journal of MedicineAlina PopaNo ratings yet
- Disseminated Intravascular Coagulation in Diabetic Ketoacidosis Rare But DangerousDocument4 pagesDisseminated Intravascular Coagulation in Diabetic Ketoacidosis Rare But DangerousAthenaeum Scientific PublishersNo ratings yet
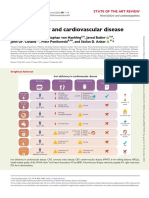
- Iron Deficiency and Cardiovascular DiseaseDocument14 pagesIron Deficiency and Cardiovascular DiseasemiguelalmenarezNo ratings yet
- KDIGO Acute Hyperkalemia Conf Report FINALDocument9 pagesKDIGO Acute Hyperkalemia Conf Report FINALJuan Carlos Kuan HigueraNo ratings yet
- 032 RuchalaDocument10 pages032 Ruchalamarcolius11No ratings yet
- European J of Heart Fail - 2022 - N Ez - Congestion in Heart Failure A Circulating Biomarker Based Perspective A ReviewDocument16 pagesEuropean J of Heart Fail - 2022 - N Ez - Congestion in Heart Failure A Circulating Biomarker Based Perspective A ReviewsilviaNo ratings yet
- Safety and Efficacy of Intravenous Ferric Derisomaltose Compared To Iron Sucrose For Iron Deficiency Anemia in Patients With Chronic Kidney Disease With and Without Heart FailureDocument8 pagesSafety and Efficacy of Intravenous Ferric Derisomaltose Compared To Iron Sucrose For Iron Deficiency Anemia in Patients With Chronic Kidney Disease With and Without Heart FailureRS Research SolutionsNo ratings yet
- Ejhf 2664Document16 pagesEjhf 2664GdfgdFdfdfNo ratings yet
- Breakthrough Bleeding in Hemophilia A Patients On ProphylaxisDocument4 pagesBreakthrough Bleeding in Hemophilia A Patients On ProphylaxisMichael John AguilarNo ratings yet
- HYPERKALEMIADocument9 pagesHYPERKALEMIAKhánh UyênNo ratings yet
- NutritionDocument3 pagesNutritionMira ApriliaNo ratings yet
- Clinical Cardiology - 2023 - Mo - Efficacy of Sacubitril Valsartan and SGLT2 Inhibitors in Heart Failure With ReducedDocument9 pagesClinical Cardiology - 2023 - Mo - Efficacy of Sacubitril Valsartan and SGLT2 Inhibitors in Heart Failure With ReducedLuluil MunirohNo ratings yet
- Hare2011 Article AssessmentAndTreatmentOfPreopeDocument13 pagesHare2011 Article AssessmentAndTreatmentOfPreopeAleksandar VilaNo ratings yet
- Ehf2 8 625Document9 pagesEhf2 8 625elza pratiwiNo ratings yet
- Anemia Besi Di Pasien HFDocument14 pagesAnemia Besi Di Pasien HFAdipNo ratings yet
- Treatment of Anemia in Kidney Disease: Beyond ErythropoietinDocument14 pagesTreatment of Anemia in Kidney Disease: Beyond ErythropoietinDesi MeliaNo ratings yet
- KDIGO HF Conf Report FINAL PDFDocument14 pagesKDIGO HF Conf Report FINAL PDFKarl Martin PinedaNo ratings yet
- CKD-Mineral Bone Disorder in Stage 4 and 5 CKD: What We Know Today?Document8 pagesCKD-Mineral Bone Disorder in Stage 4 and 5 CKD: What We Know Today?r chNo ratings yet
- Go 2006Document12 pagesGo 2006my accountNo ratings yet
- Transfusión en Pacientes PediatricosDocument14 pagesTransfusión en Pacientes PediatricosAndrea Abigail ChacónNo ratings yet
- Current Controversies in The Management of Patent Ductus Arteriosus in Preterm InfantsDocument6 pagesCurrent Controversies in The Management of Patent Ductus Arteriosus in Preterm InfantsManju KumariNo ratings yet
- Autosomal Recessive Hypercholesterolemia: Case ReportDocument7 pagesAutosomal Recessive Hypercholesterolemia: Case ReportLADY DIANEE SOTOMAYOR GUTIERREZNo ratings yet
- Relation of Gemfibrozil Treatment and Lipid LevelsDocument8 pagesRelation of Gemfibrozil Treatment and Lipid LevelsMario CoelhoNo ratings yet
- Oxidative Stress and Lipid Profile Among Hypertensive Patients at A Tertiary Centre in Kano, Northwest, NigeriaDocument9 pagesOxidative Stress and Lipid Profile Among Hypertensive Patients at A Tertiary Centre in Kano, Northwest, NigeriaidiNo ratings yet
- 64 anemiaIBDguidelinesDocument10 pages64 anemiaIBDguidelinesdwiwidyapNo ratings yet
- Pone 0165567Document14 pagesPone 0165567Pawan MishraNo ratings yet
- Hemoglobin Level in Dialysis Patients: Revisiting The Normal Hematocrit StudyDocument1 pageHemoglobin Level in Dialysis Patients: Revisiting The Normal Hematocrit StudyNexi anessaNo ratings yet
- Core CurriculamDocument13 pagesCore CurriculamdrnattoNo ratings yet
- 10 1 1 278 5572 PDFDocument7 pages10 1 1 278 5572 PDFAnggelia jopa sariNo ratings yet
- Anemia ThesisDocument4 pagesAnemia ThesisFinni Rice100% (2)
- Thrombocytopenia Associated With Chronic Liver DisDocument9 pagesThrombocytopenia Associated With Chronic Liver DisMaw BerryNo ratings yet
- Art Enfermedad Renal CronicaDocument8 pagesArt Enfermedad Renal CronicaLisset FernandezNo ratings yet
- Bleeding in AFDocument24 pagesBleeding in AFAlexandra RosaNo ratings yet
- Nephrol. Dial. Transplant. 2005 Klutstein Vii7 Vii10Document4 pagesNephrol. Dial. Transplant. 2005 Klutstein Vii7 Vii10Indah PratiwiNo ratings yet
- Anticoagulation in Patients With Kidney Failure OnDocument9 pagesAnticoagulation in Patients With Kidney Failure Onromany barsoomNo ratings yet
- EBPG Guideline On Haemodynamic InstabilityDocument23 pagesEBPG Guideline On Haemodynamic InstabilityJevon JavierNo ratings yet
- Tolvaptan For Volume Management in Heart FailureDocument13 pagesTolvaptan For Volume Management in Heart Failuredhimas satriaNo ratings yet
- Haemophilia - 2022 - Meijer - Diagnosis of Rare Bleeding DisordersDocument6 pagesHaemophilia - 2022 - Meijer - Diagnosis of Rare Bleeding Disordersyasmineessaheli2001No ratings yet
- Prevalence of Ventricular Arrhythmia and Its Associated Factors in Nondialyzed Chronic Kidney Disease PatientsDocument8 pagesPrevalence of Ventricular Arrhythmia and Its Associated Factors in Nondialyzed Chronic Kidney Disease Patientsjustin_saneNo ratings yet
- Neutrophil Lymphocyte Ratio As An Indicator For Disease Progression in Idiopathic Pulmonary FibrosisDocument9 pagesNeutrophil Lymphocyte Ratio As An Indicator For Disease Progression in Idiopathic Pulmonary FibrosishajajNo ratings yet
- Appropriate Use of Antibiotics in The NICUDocument6 pagesAppropriate Use of Antibiotics in The NICUmoniaNo ratings yet
- Surgical Antibiotic Prophylaxis - AdultDocument7 pagesSurgical Antibiotic Prophylaxis - AdultmoniaNo ratings yet
- Thienopyridines and Other ADP-Receptor AntagonistDocument34 pagesThienopyridines and Other ADP-Receptor AntagonistmoniaNo ratings yet
- Predictorsofpooradherence GJPHM Vo2No5Document10 pagesPredictorsofpooradherence GJPHM Vo2No5moniaNo ratings yet
- 2015 GomezArango ProbioticsreviewDocument10 pages2015 GomezArango ProbioticsreviewmoniaNo ratings yet
- Strokeaha 119 028400Document3 pagesStrokeaha 119 028400moniaNo ratings yet
- Comparative Effects of Amlodipine and Nifedipine GITS During Treatment and After Missing Two DosesDocument17 pagesComparative Effects of Amlodipine and Nifedipine GITS During Treatment and After Missing Two DosesmoniaNo ratings yet
- Stroke Prevention in Patients With Atrial FibrillaDocument8 pagesStroke Prevention in Patients With Atrial FibrillamoniaNo ratings yet
- ProbioticaarticleDocument41 pagesProbioticaarticlemoniaNo ratings yet
- Arthritis Rheumatology - 2018 - Fern Ndez Codina - Treatment Algorithms For Systemic Sclerosis According To ExpertsDocument9 pagesArthritis Rheumatology - 2018 - Fern Ndez Codina - Treatment Algorithms For Systemic Sclerosis According To ExpertsmoniaNo ratings yet
- Rifamycins and Anti-Diabetic Agents Drug-Drug InteractionsDocument2 pagesRifamycins and Anti-Diabetic Agents Drug-Drug InteractionsmoniaNo ratings yet
- 3 - Life History TraitsDocument16 pages3 - Life History TraitsJorge Botia BecerraNo ratings yet
- Pleskac - 2008 - Decision Making and Learning While Taking SequentiDocument20 pagesPleskac - 2008 - Decision Making and Learning While Taking SequentiDurgesh Haribhau SalunkheNo ratings yet
- Riding+out+the+storm+-+LatAm+2012 HSBC Dec2012Document98 pagesRiding+out+the+storm+-+LatAm+2012 HSBC Dec2012Sergio Gana GonzalezNo ratings yet
- Lab Ventilation SystemsDocument10 pagesLab Ventilation SystemsHyeong-Ho KimNo ratings yet
- 3rd - Sem-Ct-23-Chemical EngineeringDocument3 pages3rd - Sem-Ct-23-Chemical EngineeringJay RanjanNo ratings yet
- Nadca 13 Acrbooklet Revised - 5 8 2013Document36 pagesNadca 13 Acrbooklet Revised - 5 8 2013EMP KFMNo ratings yet
- Police Dogs From Albania As Indicators of Exposure Risk To Toxoplasma Gondii, Neospora Caninum and Vector-Borne Pathogens of Zoonotic and Veterinary ConcernDocument13 pagesPolice Dogs From Albania As Indicators of Exposure Risk To Toxoplasma Gondii, Neospora Caninum and Vector-Borne Pathogens of Zoonotic and Veterinary Concernshshsh12346565No ratings yet
- MSDS Hemolok GelDocument5 pagesMSDS Hemolok GelReniNo ratings yet
- Sa Bref 0505Document469 pagesSa Bref 0505tc5440No ratings yet
- Seko Tekna Evo TPG DatasheetDocument4 pagesSeko Tekna Evo TPG Datasheetনিস্তব্ধতার প্রহরেNo ratings yet
- Trauma Informed Care Information From Allison Sampson Jackson PDFDocument14 pagesTrauma Informed Care Information From Allison Sampson Jackson PDFMirjana StevanovicNo ratings yet
- Emersus Brochure PDFDocument11 pagesEmersus Brochure PDFDevagaran GunasekaranNo ratings yet
- Ass AsDocument1 pageAss AsMukesh BishtNo ratings yet
- Modul Ega A4Document62 pagesModul Ega A4ega nur fadillahNo ratings yet
- Multiwatt eDocument6 pagesMultiwatt edingeo11No ratings yet
- Iron Deficiency AnemiaDocument16 pagesIron Deficiency AnemiaSaboorMalikNo ratings yet
- Chemistry Notes On The Periodic Table: Syllabus 5070 O' LevelDocument8 pagesChemistry Notes On The Periodic Table: Syllabus 5070 O' LevelNancy Mohamed100% (1)
- 132kv 25kv Structure Height QuazigundDocument1 page132kv 25kv Structure Height QuazigundmanishNo ratings yet
- SPM 7 Form 5 Chapter 2: ElectricityDocument31 pagesSPM 7 Form 5 Chapter 2: Electricitylelon81No ratings yet
- Specifications of Materials and Finishes: Project: Location: OwnerDocument66 pagesSpecifications of Materials and Finishes: Project: Location: OwnerHarry Ecal100% (1)
- Disersa GuatemalasurDocument340 pagesDisersa GuatemalasurGerson David Ortíz MoralesNo ratings yet
- Philippine Electrical CodeDocument14 pagesPhilippine Electrical CodeJohn Oyan EstilloreNo ratings yet
- Tanjung Jati B Units 1 and 2 Pulverized Coal-Fired Radiant BoilerDocument2 pagesTanjung Jati B Units 1 and 2 Pulverized Coal-Fired Radiant BoileraviantaraNo ratings yet
- Cyndie-Possible Questions For Oral QuestioningDocument2 pagesCyndie-Possible Questions For Oral QuestioningOmel GarciaNo ratings yet