You might also like
- Asthma: Kinyua Md. MCM - A & E MKU Facilitator: Dr. AyungaDocument28 pagesAsthma: Kinyua Md. MCM - A & E MKU Facilitator: Dr. AyungaDennis MiritiNo ratings yet
- Module 5A: Dental Management of Patients With Asthma: Prepared By: Dr. Maria Luisa Ramos - ClementeDocument27 pagesModule 5A: Dental Management of Patients With Asthma: Prepared By: Dr. Maria Luisa Ramos - Clementeelaine100% (1)
- Asthmatic Attack: Miriti M.D Masters of Clinical Medicine Accidents and Emergency Facilitator: DR Simba DR MburuguDocument26 pagesAsthmatic Attack: Miriti M.D Masters of Clinical Medicine Accidents and Emergency Facilitator: DR Simba DR MburuguDennis MiritiNo ratings yet
- Pulmonary Diseases: Medically Compromised PatientDocument50 pagesPulmonary Diseases: Medically Compromised Patientمحمد عبدالهادي إسماعيلNo ratings yet
- Definition of Asthma: Controller) Medication Usually Prescribed inDocument5 pagesDefinition of Asthma: Controller) Medication Usually Prescribed inpiterwiselyNo ratings yet
- Asthma: Dr. Raed ShudifatDocument36 pagesAsthma: Dr. Raed ShudifatRema WaleedNo ratings yet
- Asthma Drugs GuideDocument135 pagesAsthma Drugs GuideDR. MUSICNo ratings yet
- Pedia Bronchial Asthma-1Document43 pagesPedia Bronchial Asthma-1MAHEJS HDNo ratings yet
- Chapter 29: Nursing Management: Obstructive Pulmonary DiseasesDocument5 pagesChapter 29: Nursing Management: Obstructive Pulmonary DiseasesjefrocNo ratings yet
- Respiratory Disorder Note BSC 3rd YearDocument41 pagesRespiratory Disorder Note BSC 3rd YearNancyNo ratings yet
- Clinical Pharmacy Lectures on Asthma ManagementDocument66 pagesClinical Pharmacy Lectures on Asthma Managementgurrya786No ratings yet
- Bronchial Asthma: Causes, Symptoms and TreatmentDocument21 pagesBronchial Asthma: Causes, Symptoms and TreatmentshaitabliganNo ratings yet
- Asthma: Chronic Inflammatory Airway DiseaseDocument22 pagesAsthma: Chronic Inflammatory Airway DiseaseAnna EmNo ratings yet
- Bronchial Asthma in Children FdneDocument36 pagesBronchial Asthma in Children FdneRonit ChandNo ratings yet
- ASTHMADocument9 pagesASTHMAmildred alidonNo ratings yet
- Bronchial AsthmaDocument64 pagesBronchial AsthmaDr. NasrumminallahNo ratings yet
- Acute Severe Asthma (Status Asthmaticus)Document20 pagesAcute Severe Asthma (Status Asthmaticus)blok etikakedokteranNo ratings yet
- Asthma Nursing Care Management and Study GuideDocument7 pagesAsthma Nursing Care Management and Study GuideRamakrishna BadeNo ratings yet
- AsthmaDocument10 pagesAsthmaAbirajanNo ratings yet
- Brochial Asthma EditedDocument40 pagesBrochial Asthma EditedMituran IshwarNo ratings yet
- AsthmaDocument9 pagesAsthmaNiña Jemia CortezNo ratings yet
- II. Upper Respiratory Tract DisordersDocument98 pagesII. Upper Respiratory Tract DisordersarielleortuosteNo ratings yet
- Asthama & COPDDocument84 pagesAsthama & COPDAbdullah BhattiNo ratings yet
- Nursing Theory: Asthma (Presentation)Document13 pagesNursing Theory: Asthma (Presentation)vinda astri permatasari100% (1)
- Acute Exacerbation of AsthmaDocument33 pagesAcute Exacerbation of Asthmafrankozed1No ratings yet
- Asthma in Children My PresentationDocument49 pagesAsthma in Children My PresentationPutra Skate100% (2)
- Bronchial Asthma 085523Document29 pagesBronchial Asthma 085523Satrumin ShirimaNo ratings yet
- Acute Lower Respiratory Tract Infection (ALRTI)Document43 pagesAcute Lower Respiratory Tract Infection (ALRTI)yosephNo ratings yet
- Asthma: Asthma (from the Greek άσθμα, ásthma, "panting") is a commonDocument11 pagesAsthma: Asthma (from the Greek άσθμα, ásthma, "panting") is a commonRomarie Salvador-CastilloNo ratings yet
- 01-Obstractihe Pulmonary Diseases (Asthma) PDFDocument50 pages01-Obstractihe Pulmonary Diseases (Asthma) PDFsima.koye2005No ratings yet
- Asthma Concept MapDocument7 pagesAsthma Concept Mapshehada bondad100% (2)
- Felső Légúti FertőzésekDocument20 pagesFelső Légúti FertőzésekKondász Antal Gábor MedNo ratings yet
- Asthma in Children CMEDocument37 pagesAsthma in Children CMEGideon K. MutaiNo ratings yet
- Asthma, Pulmonary Edema, ARDS, Pulmonary EmbolismDocument16 pagesAsthma, Pulmonary Edema, ARDS, Pulmonary EmbolismKoRnflakesNo ratings yet
- MF3 - AsthmaDocument42 pagesMF3 - AsthmaAnnbe BarteNo ratings yet
- Bronchial AsthmaDocument84 pagesBronchial AsthmaNavnik NaithikNo ratings yet
- LECTURE NOTE ON ASTHMA-WPS OfficeDocument7 pagesLECTURE NOTE ON ASTHMA-WPS OfficeNaija Nurses TVNo ratings yet
- Bronchial AsthmaDocument54 pagesBronchial AsthmaSehar162100% (2)
- Asthma: Prepared By: Genesis T. Consigna. BSN-3Document10 pagesAsthma: Prepared By: Genesis T. Consigna. BSN-3Digital ExpressNo ratings yet
- AsthmaDocument29 pagesAsthmaViji MNo ratings yet
- Allergic Rhinitis: University of Michigan Guidelines For Health System Clinical CareDocument12 pagesAllergic Rhinitis: University of Michigan Guidelines For Health System Clinical Carerko_akibNo ratings yet
- Reversible Airflow ObstructionDocument2 pagesReversible Airflow Obstruction85robertNo ratings yet
- Zuhaib SynopsisDocument24 pagesZuhaib Synopsisthehealer7No ratings yet
- AsthmaDocument18 pagesAsthmaELDHOSE RAJUNo ratings yet
- Asthma: Chronic Inflammation of The Airways. The Hyper-Responsive Airways Typical of AsthmaDocument7 pagesAsthma: Chronic Inflammation of The Airways. The Hyper-Responsive Airways Typical of AsthmaRaj PaulNo ratings yet
- Upper Respiratory DisordersDocument37 pagesUpper Respiratory DisordersClaire Maurice JuaneroNo ratings yet
- Acute ExaerbationDocument4 pagesAcute ExaerbationEden RamosNo ratings yet
- Feline Asthma: A Pathophysiologic Basis of TherapyDocument5 pagesFeline Asthma: A Pathophysiologic Basis of TherapyEnnur NufianNo ratings yet
- ACUTE ASTHMA ATTACK EMERGENCY TREATMENTDocument31 pagesACUTE ASTHMA ATTACK EMERGENCY TREATMENTMuneeb YounisNo ratings yet
- AsthmaDocument3 pagesAsthmaLizeth QuerubinNo ratings yet
- Group 2 Activity 8 Instrumentation 4 Phchem LabDocument3 pagesGroup 2 Activity 8 Instrumentation 4 Phchem LabJeyma DacumosNo ratings yet
- Bronchial AsthmaDocument46 pagesBronchial AsthmaZahidul ZahidNo ratings yet
- Case Study of AsthmaDocument6 pagesCase Study of Asthmabuzz Q100% (4)
- Lower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocument95 pagesLower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingRI NANo ratings yet
- AsthmaDocument45 pagesAsthmaRaquel M. MendozaNo ratings yet
- AsthmaDocument31 pagesAsthmakenmanikeseNo ratings yet
- Bronchial Asthma in Acute Exacerbation - FinalDocument17 pagesBronchial Asthma in Acute Exacerbation - Finalmary_sulit_150% (2)
- Asthma and CopdDocument44 pagesAsthma and CopdBeer Dilacshe100% (1)
- Fast Facts: Respiratory Allergies: Understand aeroallergens, improve treatment responseFrom EverandFast Facts: Respiratory Allergies: Understand aeroallergens, improve treatment responseNo ratings yet
- 7-Obturation 1Document38 pages7-Obturation 1Mahmoud HamamrehNo ratings yet
- Chapter 3 - ProteinsDocument35 pagesChapter 3 - ProteinsMahmoud HamamrehNo ratings yet
- Chapter 1 - Principles of NutritionDocument50 pagesChapter 1 - Principles of NutritionMahmoud HamamrehNo ratings yet
- Treatment Planning FPD Lec 2Document23 pagesTreatment Planning FPD Lec 20 0No ratings yet
- اندو مايكروDocument9 pagesاندو مايكروMahmoud HamamrehNo ratings yet
- اندو 2Document12 pagesاندو 2Mahmoud HamamrehNo ratings yet
- اندو3Document10 pagesاندو3Mahmoud HamamrehNo ratings yet
- Essential Attitudes, Personal Qualities, and Professional Behaviors Required in NursingDocument27 pagesEssential Attitudes, Personal Qualities, and Professional Behaviors Required in NursingshirleyNo ratings yet
- Pengumuman Jadwal Rapid Test Antigen Gratis Bagi Peserta Ujian SKB CPNS Pemerintah Kota Pangkalpinang 2021Document16 pagesPengumuman Jadwal Rapid Test Antigen Gratis Bagi Peserta Ujian SKB CPNS Pemerintah Kota Pangkalpinang 2021Syahrul SalehNo ratings yet
- CareGroup Case Study QuestionsDocument1 pageCareGroup Case Study QuestionsEnrica Melissa PanjaitanNo ratings yet
- Psychology Learning Objectives, Contents, Activities and EvaluationDocument12 pagesPsychology Learning Objectives, Contents, Activities and EvaluationSAYMABANUNo ratings yet
- Explaining Medication To Patients: Ni Kadek Ary Susandi, S.S., M.App - LingDocument11 pagesExplaining Medication To Patients: Ni Kadek Ary Susandi, S.S., M.App - LingmirahayuuNo ratings yet
- Rajiv Gandhi University Thesis Topics PediatricsDocument6 pagesRajiv Gandhi University Thesis Topics PediatricsWriteMyBusinessPaperSingapore100% (2)
- Teen Breathe June2020Document70 pagesTeen Breathe June2020Екатерина Кедрина100% (1)
- Centric Relation Registration With Intraoral Central Bearing On Curved vs. Flat Plates With Rim Trays in Edentulous PatientsDocument8 pagesCentric Relation Registration With Intraoral Central Bearing On Curved vs. Flat Plates With Rim Trays in Edentulous PatientsCamila MuñozNo ratings yet
- Sports Medicine 10-Lesson 4 - Lower Leg Muscles Turf ToeDocument5 pagesSports Medicine 10-Lesson 4 - Lower Leg Muscles Turf Toeapi-383568582No ratings yet
- bài thầy thông (E)Document42 pagesbài thầy thông (E)SumaleeNo ratings yet
- Turkey's Growing Healthcare Sector Driven by Private ProvidersDocument69 pagesTurkey's Growing Healthcare Sector Driven by Private ProviderssbulenterisNo ratings yet
- Scissor Lift ProcedureDocument2 pagesScissor Lift ProcedureAdhi LatifNo ratings yet
- MCN ReviewerDocument3 pagesMCN ReviewerJunghoon YangParkNo ratings yet
- ACUTE KIDNEY INJURY SIGNS, SYMPTOMS, AND CAUSESDocument10 pagesACUTE KIDNEY INJURY SIGNS, SYMPTOMS, AND CAUSESYanti TandjungNo ratings yet
- Maharashtra Government PGM Admissions 2015-2016 Round 2 Selection ListDocument30 pagesMaharashtra Government PGM Admissions 2015-2016 Round 2 Selection ListAbhinav BhardwajNo ratings yet
- Nursing Health AssessmentDocument19 pagesNursing Health AssessmentAHMAD HASIMI BIN ABDUL GHANI STUDENTNo ratings yet
- Triage in Polytauma: Prof. Dr. A. Chandrasekaran M.S., PH.D.Document73 pagesTriage in Polytauma: Prof. Dr. A. Chandrasekaran M.S., PH.D.ShrutiNo ratings yet
- Psikososial Dan Budaya Dalam KeperawatanDocument11 pagesPsikososial Dan Budaya Dalam KeperawatanMohamad SyakiebNo ratings yet
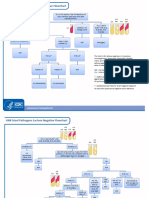
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- Seligman Attributional Style QuestionnaireDocument14 pagesSeligman Attributional Style QuestionnaireAnjali VyasNo ratings yet
- UntitledDocument7 pagesUntitledSucdi AbdirazakNo ratings yet
- Module 2Document43 pagesModule 2jbg060595No ratings yet
- Misrak FeyissaDocument41 pagesMisrak FeyissaN SNo ratings yet
- Experienced Pharmacist Seeking New OpportunityDocument3 pagesExperienced Pharmacist Seeking New OpportunityIman ElshafieNo ratings yet
- Rts Medicines 7778-1Document79 pagesRts Medicines 7778-1sam yadavNo ratings yet
- CEMP-Framework Beach Project Scope Rev0Document152 pagesCEMP-Framework Beach Project Scope Rev0gowthamNo ratings yet
- 21 - Piriformis SyndromeDocument11 pages21 - Piriformis SyndromewatiNo ratings yet
- Introduction To Basic Food PreparationDocument18 pagesIntroduction To Basic Food PreparationJiety PlarisanNo ratings yet
- Research Paper Topics For Developmental PsychologyDocument7 pagesResearch Paper Topics For Developmental PsychologyxbvtmpwgfNo ratings yet
- English: Second Quarter - Module 3Document17 pagesEnglish: Second Quarter - Module 3NMDNMSSD67% (3)