You might also like
- Endografts For The Treatment of Abdominal Aortic ADocument15 pagesEndografts For The Treatment of Abdominal Aortic AAhmed MohammedNo ratings yet
- Cathetersandwires DrVaibhavDocument15 pagesCathetersandwires DrVaibhavAhmed MohammedNo ratings yet
- Proximal Abdominal EVT SupplementDocument6 pagesProximal Abdominal EVT SupplementAhmed MohammedNo ratings yet
- Doacs For VteDocument10 pagesDoacs For VteAhmed MohammedNo ratings yet
- Ecr 12 1 40Document6 pagesEcr 12 1 40Ahmed MohammedNo ratings yet
- Direct Oral Anticoagulants (DOACs)Document17 pagesDirect Oral Anticoagulants (DOACs)Ahmed MohammedNo ratings yet
- DOAC VTE Treatment April2020Document4 pagesDOAC VTE Treatment April2020Ahmed MohammedNo ratings yet
- Tips and Techniques For Optimal Stent Graft Placement in Angulated Aneurysm NecksDocument6 pagesTips and Techniques For Optimal Stent Graft Placement in Angulated Aneurysm NecksAhmed MohammedNo ratings yet
- Long-Term Follow-Up of Type II Endoleak Embolization Reveals The Need For Close SurveillanceDocument8 pagesLong-Term Follow-Up of Type II Endoleak Embolization Reveals The Need For Close SurveillanceAhmed MohammedNo ratings yet
- 5hodgikiss NewInnovationsinEndoleakManagementRead OnlyDocument6 pages5hodgikiss NewInnovationsinEndoleakManagementRead OnlyAhmed MohammedNo ratings yet
- VTE Risk Assessment Tool Caprini Score Card Eng 30apr2018Document2 pagesVTE Risk Assessment Tool Caprini Score Card Eng 30apr2018Ahmed MohammedNo ratings yet
- FR System - Vs Guage SystemDocument12 pagesFR System - Vs Guage SystemAhmed MohammedNo ratings yet
- Thromboprohylaxis and DVT in Surgical PRDocument7 pagesThromboprohylaxis and DVT in Surgical PRAhmed MohammedNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Music For Pain Relief - Binaural Beats Instant Download PDFDocument1 pageMusic For Pain Relief - Binaural Beats Instant Download PDFIoannis ManNo ratings yet
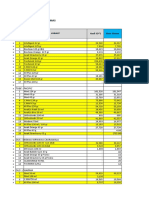
- Bahan Kemas - Selisih SO Vs Sistem FY2020 - 291220Document17 pagesBahan Kemas - Selisih SO Vs Sistem FY2020 - 291220Idan RidwanNo ratings yet
- Product Name: Max Bupa Health Recharge, Product UIN: MAXHLIP18129V011718Document51 pagesProduct Name: Max Bupa Health Recharge, Product UIN: MAXHLIP18129V011718906rahulNo ratings yet
- Update of Dental Local AnesthesiaDocument13 pagesUpdate of Dental Local AnesthesiaDeb SNo ratings yet
- Nathália Becker - Sleep Quality and Stress - A Literature Review 2015Document10 pagesNathália Becker - Sleep Quality and Stress - A Literature Review 2015gilangNo ratings yet
- Doctors Bag ChecklistDocument6 pagesDoctors Bag ChecklistFritz Jossane MendozaNo ratings yet
- What Causes IBS?Document4 pagesWhat Causes IBS?prima suci angrainiNo ratings yet
- Full Report Interventions For Children On The Autism Spectrum A Synthesis of Research EvidenceDocument503 pagesFull Report Interventions For Children On The Autism Spectrum A Synthesis of Research EvidenceGiedrė Skaisgirytė100% (1)
- Honora Lee Wolfe - Managing Menopause Naturally With Chinese Medicine-Blue Poppy Enterprises (1999)Document210 pagesHonora Lee Wolfe - Managing Menopause Naturally With Chinese Medicine-Blue Poppy Enterprises (1999)Echimov Anca100% (1)
- Metamizole A Review Profile of A Well Known Forgotten Drug Part II Clinical Profile PDFDocument16 pagesMetamizole A Review Profile of A Well Known Forgotten Drug Part II Clinical Profile PDFcristirusu23No ratings yet
- NCM 104 Lecture Chapter 5 - NCDDocument39 pagesNCM 104 Lecture Chapter 5 - NCDWilma Nierva BeraldeNo ratings yet
- Fridays LawsDocument2 pagesFridays LawsAHRMMNo ratings yet
- Pathophysiology of Alzheimers DiseaseDocument2 pagesPathophysiology of Alzheimers DiseaseJaysellePuguonTabijeNo ratings yet
- High Yield Plab TopicsDocument20 pagesHigh Yield Plab TopicsBeaulah HunidzariraNo ratings yet
- 89587501! PDFDocument8 pages89587501! PDFSRBBC AcademyNo ratings yet
- SLD Gi SarullaDocument1 pageSLD Gi SarullasacilatwaeNo ratings yet
- SulfonamidesDocument3 pagesSulfonamidesMahdi DiabNo ratings yet
- Pharmacology Chapter 3 and 4Document2 pagesPharmacology Chapter 3 and 4Dingal AijayNo ratings yet
- Indications For Barium StudyDocument4 pagesIndications For Barium Studysidorai100% (1)
- Stella Joy, Part II: Every Precious MomentDocument4 pagesStella Joy, Part II: Every Precious MomentToronto StarNo ratings yet
- History of PsychotherapyDocument21 pagesHistory of PsychotherapypamNo ratings yet
- Acute Fatty Liver of Pregnancy - NEJMDocument2 pagesAcute Fatty Liver of Pregnancy - NEJMJing CruzNo ratings yet
- International Society For Technology in Arthroplasty - Indicação de ArtigosDocument77 pagesInternational Society For Technology in Arthroplasty - Indicação de ArtigosJosé santanaNo ratings yet
- TSX-302A/2, Aquilion Prime CT SystemDocument5 pagesTSX-302A/2, Aquilion Prime CT Systemavinash.grey.bizNo ratings yet
- Challenging Behaviours (Power Point)Document17 pagesChallenging Behaviours (Power Point)tamNo ratings yet
- 3 Done Done Lesson Plan NewDocument19 pages3 Done Done Lesson Plan NewNavpreet Kaur100% (2)
- Clinicalmanifestationsand Treatmentofdrug-Induced HepatotoxicityDocument9 pagesClinicalmanifestationsand Treatmentofdrug-Induced HepatotoxicityChâu Khắc ToànNo ratings yet
- Gynaecological Ultrasound in Clinical PracticeDocument247 pagesGynaecological Ultrasound in Clinical Practiceyulb_1100% (5)
- Nursing Care Plan Mrs. Patao Ob Ward, GSGH Assessment SubjectiveDocument3 pagesNursing Care Plan Mrs. Patao Ob Ward, GSGH Assessment Subjectiveraizelc100% (2)
- A Simplified Appendicitis ScoreDocument6 pagesA Simplified Appendicitis ScoreDenny TombengNo ratings yet