You might also like
- How to Heal Teeth Naturally & Cure Tooth Decay: The book on holistic dental care, healing cavities, toothaches, dental pains, oil pulling and more...From EverandHow to Heal Teeth Naturally & Cure Tooth Decay: The book on holistic dental care, healing cavities, toothaches, dental pains, oil pulling and more...Rating: 4 out of 5 stars4/5 (8)
- Teething: Krishna Chauhan 55 3 YearDocument29 pagesTeething: Krishna Chauhan 55 3 YearkrishnaNo ratings yet
- Impacted Wisdom Tooth, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandImpacted Wisdom Tooth, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Patterns of Tooth MovementDocument6 pagesPatterns of Tooth MovementAshish DeotaleNo ratings yet
- Dental Abscess, (Gum Boil) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDental Abscess, (Gum Boil) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Teeth Eruption WordDocument24 pagesTeeth Eruption WordAhmed hegazyNo ratings yet
- Preventive and InterseptiveDocument90 pagesPreventive and InterseptivemuhammadNo ratings yet
- Enamel and Dentine Maria BarraganDocument19 pagesEnamel and Dentine Maria Barraganjobar60No ratings yet
- LECTURE 5 Early EruptionDocument4 pagesLECTURE 5 Early Eruptionمؤمل رياض سعد كاظمNo ratings yet
- Principle of Maxillary Impacted Teeth: Done By: Yamamh Emad Hadeel Luay Yaseen TareqDocument26 pagesPrinciple of Maxillary Impacted Teeth: Done By: Yamamh Emad Hadeel Luay Yaseen TareqB AlhashimiNo ratings yet
- PBL Oral BiologyDocument12 pagesPBL Oral BiologyhusunasanNo ratings yet
- Developmental TeethDocument53 pagesDevelopmental Teethlyli Star AngeloNo ratings yet
- Early Eruption: Pediatric Dentistry 4th Stage Lec. 3Document7 pagesEarly Eruption: Pediatric Dentistry 4th Stage Lec. 3Ishtar AliNo ratings yet
- Occlusal SplintsDocument1 pageOcclusal SplintsrekabiNo ratings yet
- Dental CariesDocument20 pagesDental Carieschantelle acopNo ratings yet
- Developmental Anomalies of TeethDocument78 pagesDevelopmental Anomalies of TeethPauline Joy Cayago CastilloNo ratings yet
- PEDIATRIC PATHOLOGY TITLEDocument27 pagesPEDIATRIC PATHOLOGY TITLERayne GelleNo ratings yet
- Impacted Teeth Part ADocument27 pagesImpacted Teeth Part AMohsin HabibNo ratings yet
- Rabbit Dental Disease Diagnosis & TreatmentDocument6 pagesRabbit Dental Disease Diagnosis & TreatmentSebastián Ordóñez RamírezNo ratings yet
- The Tooth Worm: A History of Dental Caries TheoriesDocument32 pagesThe Tooth Worm: A History of Dental Caries TheoriesMonalisa DebbarmaNo ratings yet
- Important stages of primary and permanent tooth eruptionDocument39 pagesImportant stages of primary and permanent tooth eruptionJessica AlexanderNo ratings yet
- Tooth AcheDocument8 pagesTooth AcheWerly Eka LiaNo ratings yet
- Management of Developing DentitionDocument51 pagesManagement of Developing Dentitionahmed alshaariNo ratings yet
- Regressive Alterations of TeethDocument3 pagesRegressive Alterations of TeethBhaveshNo ratings yet
- Teeth Root Canal TreatmentDocument3 pagesTeeth Root Canal TreatmentAdit Wendy YRNo ratings yet
- Early Childhood Caries and Dental Trauma on Primary TeethDocument52 pagesEarly Childhood Caries and Dental Trauma on Primary TeethLila VininingtyasNo ratings yet
- Dental AbscessDocument14 pagesDental Abscessvinnu kalyanNo ratings yet
- Malocclusion (2nd Concept Map)Document4 pagesMalocclusion (2nd Concept Map)Stephanie Joy EscalaNo ratings yet
- Cracked Tooth Syndrome and Vertical Root Fracture 2 1 1Document85 pagesCracked Tooth Syndrome and Vertical Root Fracture 2 1 1Mohamed Ali AbdelhamedNo ratings yet
- Toothache and InfectionDocument31 pagesToothache and Infectionishaaadam114No ratings yet
- Periodontal Diseases in ChildrenDocument46 pagesPeriodontal Diseases in ChildrenJustine TanNo ratings yet
- Abnormalities of Teeth Eruption, Structure, Form, Number, and SizeDocument48 pagesAbnormalities of Teeth Eruption, Structure, Form, Number, and SizeNoor AlsanouriNo ratings yet
- Developmental Disturbances of Shape of TeethDocument18 pagesDevelopmental Disturbances of Shape of Teethneeruraj08No ratings yet
- Chapter 41.Ppt HypersensitivityDocument63 pagesChapter 41.Ppt HypersensitivityMaria Mercedes LeivaNo ratings yet
- Anatomic Anomalies - LectureDocument10 pagesAnatomic Anomalies - LectureKhalid BhatNo ratings yet
- Dental - GlossaryDocument8 pagesDental - GlossaryMadhura Pushpa kumaraNo ratings yet
- Impacted Wisdom Teeth Combat Strategies: A Potential ThreatDocument4 pagesImpacted Wisdom Teeth Combat Strategies: A Potential ThreatCiutac ŞtefanNo ratings yet
- Deepbite & Open BiteDocument36 pagesDeepbite & Open BiteNoor Zia100% (1)
- Cracked Tooth SyndromeDocument49 pagesCracked Tooth SyndromeUzair Aftab100% (1)
- Veterinary Dental SurgeryDocument23 pagesVeterinary Dental SurgeryUNICORN TIMENo ratings yet
- Development of Dentition WordDocument21 pagesDevelopment of Dentition Wordshubhangi_jain_10100% (1)
- DentoalveolarAbscess in Children LectureDocument22 pagesDentoalveolarAbscess in Children LectureARNOLD OBINo ratings yet
- What is a Root Canal TreatmentDocument5 pagesWhat is a Root Canal TreatmentjjahaddinNo ratings yet
- A Glimpse of DentistryDocument22 pagesA Glimpse of DentistryNidhi ShahNo ratings yet
- English ExamDocument9 pagesEnglish ExamblueNo ratings yet
- 10 Treatments for Cracked or Chipped TeethDocument12 pages10 Treatments for Cracked or Chipped TeethDaveNo ratings yet
- Dental CariesDocument5 pagesDental CariesnmiteiNo ratings yet
- Oral and Denture Care PPT Finale 1Document75 pagesOral and Denture Care PPT Finale 1Jan Joseph BanzuelaNo ratings yet
- Developmental Disturbances of TeethDocument45 pagesDevelopmental Disturbances of TeethAmritha JamesNo ratings yet
- Careis Dentis 2Document3 pagesCareis Dentis 2zayNo ratings yet
- Dentistry in Pet Rabbits: AbstractDocument14 pagesDentistry in Pet Rabbits: AbstractShuhada Hamid100% (2)
- Treatment of Open Bite & CrossbiteDocument57 pagesTreatment of Open Bite & CrossbiteDr. Sushil KumarNo ratings yet
- Developmental Disturbances of Oral StructuresDocument36 pagesDevelopmental Disturbances of Oral StructuresDR. H. DIANA J.HENRY CHRISTOPHERNo ratings yet
- Jenny's Smooth Teeth AnswersDocument3 pagesJenny's Smooth Teeth AnswersT LolaNo ratings yet
- Sequelae of TraumaDocument27 pagesSequelae of TraumaDr.O.R.GANESAMURTHINo ratings yet
- Developmental Disorders: Dr. Chakshu Aggarwal (MDS) SNR Lecturer Oral PathologyDocument38 pagesDevelopmental Disorders: Dr. Chakshu Aggarwal (MDS) SNR Lecturer Oral PathologydrchakshuaggarwalNo ratings yet
- Chapter 1 IntroductionDocument8 pagesChapter 1 IntroductionShilpi BdsNo ratings yet
- Prezentare (2) EnglezaDocument12 pagesPrezentare (2) EnglezaStupeliman CristinaNo ratings yet
- Ajman University of Science and TechnoloddgyDocument10 pagesAjman University of Science and TechnoloddgyZainab Al-ObaidiNo ratings yet
- Causes of Malocclusion Treatmemt of MalocclusionDocument4 pagesCauses of Malocclusion Treatmemt of MalocclusionTolea SirghiNo ratings yet
- CURS 8 and 9 Trauma and Its ManagementDocument96 pagesCURS 8 and 9 Trauma and Its Managementtaliya. shvetzNo ratings yet
- Pathology of the Orbit and Ophthalmology Course 3Document24 pagesPathology of the Orbit and Ophthalmology Course 3taliya. shvetzNo ratings yet
- Course 7 I, IIDocument17 pagesCourse 7 I, IItaliya. shvetzNo ratings yet
- Infectious Diseases CasesDocument30 pagesInfectious Diseases Casestaliya. shvetzNo ratings yet
- Dental caries in temporary dentitionDocument43 pagesDental caries in temporary dentitiontaliya. shvetzNo ratings yet
- ENT CourseDocument29 pagesENT Coursetaliya. shvetzNo ratings yet
- Dme C1Document7 pagesDme C1taliya. shvetzNo ratings yet
- Pathology of Wisdom MolarsDocument8 pagesPathology of Wisdom Molarstaliya. shvetzNo ratings yet
- Eruptive Disorders of Permanent TeethDocument6 pagesEruptive Disorders of Permanent Teethtaliya. shvetzNo ratings yet
- Notes From Dental Prosthesis (AutoRecovered)Document5 pagesNotes From Dental Prosthesis (AutoRecovered)taliya. shvetzNo ratings yet
- Impacted Canine Pathology and Treatment OptionsDocument4 pagesImpacted Canine Pathology and Treatment Optionstaliya. shvetzNo ratings yet
- 3-4-5 Larynx Pharynx EsophagusDocument25 pages3-4-5 Larynx Pharynx Esophagustaliya. shvetzNo ratings yet
- MD PW 1,2 Eyelids and AnatomyDocument84 pagesMD PW 1,2 Eyelids and Anatomytaliya. shvetzNo ratings yet
- ENT Course 1-2-3 General, Rhino. OtoDocument30 pagesENT Course 1-2-3 General, Rhino. Ototaliya. shvetzNo ratings yet
- ENT Summery TABLEDocument19 pagesENT Summery TABLEtaliya. shvetzNo ratings yet
- Construction Materials and Testing: "WOOD"Document31 pagesConstruction Materials and Testing: "WOOD"Aira Joy AnyayahanNo ratings yet
- 0 Plan Lectie Cls XDocument3 pages0 Plan Lectie Cls Xevil100% (1)
- UnitTest D10 Feb 2024Document26 pagesUnitTest D10 Feb 2024dev.shah8038No ratings yet
- Twingo 3 & Clio 4Document10 pagesTwingo 3 & Clio 4Alexandre Le GrandNo ratings yet
- Hotel Engineering Facilities: A Case Study of Maintenance PerformanceDocument7 pagesHotel Engineering Facilities: A Case Study of Maintenance PerformanceHoh Pui KeiNo ratings yet
- COR2-03 Admist The Mists and Coldest Frost PDFDocument16 pagesCOR2-03 Admist The Mists and Coldest Frost PDFLouis BachNo ratings yet
- MMME 21 1st Long Exam Lecture NotesDocument74 pagesMMME 21 1st Long Exam Lecture NotesGraver lumiousNo ratings yet
- MKTG 2126 - Assignment 3Document2 pagesMKTG 2126 - Assignment 3omar mcintoshNo ratings yet
- CBK Test QuestionsDocument2 pagesCBK Test QuestionsMehul GuptaNo ratings yet
- Manual PDFDocument9 pagesManual PDFRuth ResuelloNo ratings yet
- GMS175CSDocument4 pagesGMS175CScorsini999No ratings yet
- Classical Fields 2Document2 pagesClassical Fields 2Jonathan SanchezNo ratings yet
- Clock Al Ghadeer Setup GuideDocument4 pagesClock Al Ghadeer Setup Guideakberbinshowkat100% (2)
- MFC-L2710DW 2Document8 pagesMFC-L2710DW 2Pinto ModakNo ratings yet
- 24.ratios, Rates and Proportions PDFDocument9 pages24.ratios, Rates and Proportions PDFMilsonNo ratings yet
- Unit Rates and Cost Per ItemDocument213 pagesUnit Rates and Cost Per ItemDesiree Vera GrauelNo ratings yet
- Introduction to Globalization ExplainedDocument27 pagesIntroduction to Globalization ExplainedMichael Ron DimaanoNo ratings yet
- 01 A Brief Introduction To Cloud ComputingDocument25 pages01 A Brief Introduction To Cloud ComputingfirasibraheemNo ratings yet
- Design and Analysis of Buck ConverterDocument18 pagesDesign and Analysis of Buck Converterk rajendraNo ratings yet
- CD 1 - Screening & DiagnosisDocument27 pagesCD 1 - Screening & DiagnosiskhairulfatinNo ratings yet
- CHM131 Presentation - Oxidation of MetalsDocument11 pagesCHM131 Presentation - Oxidation of MetalsNazrul ShahNo ratings yet
- All Creatures Great and SmallDocument4 pagesAll Creatures Great and SmallsaanviranjanNo ratings yet
- Textbook of Heat Transfer Sukhatme S PDocument122 pagesTextbook of Heat Transfer Sukhatme S PSamer HouzaynNo ratings yet
- Dream Life - Allan HobsonDocument307 pagesDream Life - Allan HobsonJose MuñozNo ratings yet
- Red Lion Edict-97 - Manual PDFDocument282 pagesRed Lion Edict-97 - Manual PDFnaminalatrukNo ratings yet
- Technical Information System Overview Prosafe-Com 3.00 Prosafe-ComDocument49 pagesTechnical Information System Overview Prosafe-Com 3.00 Prosafe-Comshekoofe danaNo ratings yet
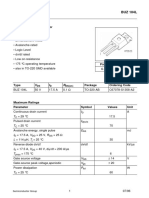
- Sipmos Power Transistor: BUZ 104LDocument10 pagesSipmos Power Transistor: BUZ 104LAlexsander MeloNo ratings yet
- DOJ OIG Issues 'Fast and Furious' ReportDocument512 pagesDOJ OIG Issues 'Fast and Furious' ReportFoxNewsInsiderNo ratings yet
- NST 021 Orientation SASDocument5 pagesNST 021 Orientation SASLady Mae AguilarNo ratings yet
- NOV Completion ToolsDocument12 pagesNOV Completion Toolsfffggg777No ratings yet