You might also like
- Fluorescence Microscopy: Super-Resolution and other Novel TechniquesFrom EverandFluorescence Microscopy: Super-Resolution and other Novel TechniquesAnda CorneaNo ratings yet
- Deep Network Design for Medical Image Computing: Principles and ApplicationsFrom EverandDeep Network Design for Medical Image Computing: Principles and ApplicationsNo ratings yet
- Recognition and Classification of Diabetic Retinopathy Using Retinal Fundus ImagesDocument7 pagesRecognition and Classification of Diabetic Retinopathy Using Retinal Fundus ImagesIJRASETPublicationsNo ratings yet
- Diabetic Retinopathy Detection Using SVMDocument10 pagesDiabetic Retinopathy Detection Using SVMIJRASETPublicationsNo ratings yet
- PPDocument2 pagesPPraju yNo ratings yet
- Niemeijer2004comparative - DriveDocument9 pagesNiemeijer2004comparative - DriveJosé Ignacio OrlandoNo ratings yet
- A Study of The Attitudes of Road User in Enhancing The Gross National Happiness Using Combined Fuzzy Cognitive Maps (CFCMS)Document4 pagesA Study of The Attitudes of Road User in Enhancing The Gross National Happiness Using Combined Fuzzy Cognitive Maps (CFCMS)IIR indiaNo ratings yet
- Identification of Retinal Diseases Using Blood Vessel Segmentation Based On Robinson Compass Mask and K-Means Clustering AlgorithmDocument7 pagesIdentification of Retinal Diseases Using Blood Vessel Segmentation Based On Robinson Compass Mask and K-Means Clustering AlgorithmIJRASETPublicationsNo ratings yet
- Hard Exudates Detection: A Review: July 2020Document9 pagesHard Exudates Detection: A Review: July 2020Diana Baltodano GarciaNo ratings yet
- Comparative Study of Diabetic Retinopathy Detection Using Machine Learning TechniquesDocument7 pagesComparative Study of Diabetic Retinopathy Detection Using Machine Learning TechniquesIJRASETPublications100% (1)
- Early Diabetic Retinopathy Detection Using Deep LearningDocument7 pagesEarly Diabetic Retinopathy Detection Using Deep LearningIJRASETPublicationsNo ratings yet
- Automated Classification of Age-Related Macular Degeneration From Optical Coherence Tomography Images Using Deep Learning ApproachDocument11 pagesAutomated Classification of Age-Related Macular Degeneration From Optical Coherence Tomography Images Using Deep Learning ApproachIAES IJAINo ratings yet
- Data Preprocessing Techniques For Retinal OCT and Fundus ImagesDocument5 pagesData Preprocessing Techniques For Retinal OCT and Fundus ImagesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Final Revision of Octane Paper For Nature MedicineDocument41 pagesFinal Revision of Octane Paper For Nature MedicineElias Alboadicto Villagrán DonaireNo ratings yet
- Detection of Diabetic Retinopathy Using Deep LearningDocument9 pagesDetection of Diabetic Retinopathy Using Deep LearningIJRASETPublicationsNo ratings yet
- Retinal Image Segmentation and Disease Classification Using Deep LearningDocument13 pagesRetinal Image Segmentation and Disease Classification Using Deep LearningIJRASETPublicationsNo ratings yet
- A Novel Computationally Simple K-Means Segmentation Model For Retinal Image SegmentationDocument8 pagesA Novel Computationally Simple K-Means Segmentation Model For Retinal Image SegmentationMalathiMohanNo ratings yet
- Disease Prediction Based On Retinal Images Using Deep Neural NetworksDocument3 pagesDisease Prediction Based On Retinal Images Using Deep Neural NetworksNahid HasanNo ratings yet
- Multi-Class Retinal Diseases Detection Using Deep CNN With Minimal Memory Consumption PDFDocument11 pagesMulti-Class Retinal Diseases Detection Using Deep CNN With Minimal Memory Consumption PDFavinashkumar12110No ratings yet
- Identification of Diabetic Retinopathy Using Fuzzy Logic and Back Propagation Neural NetworkDocument8 pagesIdentification of Diabetic Retinopathy Using Fuzzy Logic and Back Propagation Neural Networkpurushothaman sinivasanNo ratings yet
- Patient Monitoring System Based On Internet of ThingsDocument15 pagesPatient Monitoring System Based On Internet of ThingsSiddhi PatilNo ratings yet
- Research Article Diabetic Retinopathy Detection Using Local Extrema Quantized Haralick Features With Long Short-Term Memory NetworkDocument12 pagesResearch Article Diabetic Retinopathy Detection Using Local Extrema Quantized Haralick Features With Long Short-Term Memory NetworkHyacinth A RotaNo ratings yet
- Omicron Detection With X-Ray and CT-Scan Using Machine LearningDocument6 pagesOmicron Detection With X-Ray and CT-Scan Using Machine LearningIJRASETPublicationsNo ratings yet
- Using Genetic Algorithm For Identification of Diabetic Retinal Exudates in Digital Color ImagesDocument11 pagesUsing Genetic Algorithm For Identification of Diabetic Retinal Exudates in Digital Color ImagesSebastin AshokNo ratings yet
- Mia-Unet: Multi-Scale Iterative Aggregation U-Network For Retinal Vessel SegmentationDocument24 pagesMia-Unet: Multi-Scale Iterative Aggregation U-Network For Retinal Vessel Segmentationtsureda1290No ratings yet
- Multi-Lesion Segmentation of Diabetic Retinopathy Using Deep LearningDocument6 pagesMulti-Lesion Segmentation of Diabetic Retinopathy Using Deep LearningIJRASETPublicationsNo ratings yet
- A Brain Tumor Detection Using Image ProcessingDocument5 pagesA Brain Tumor Detection Using Image ProcessingIJRASETPublicationsNo ratings yet
- 2021discrimination of Diabetic Retinopathy From Optical Coherence Tomography Angiography Images Using Machine Learning MethodsDocument6 pages2021discrimination of Diabetic Retinopathy From Optical Coherence Tomography Angiography Images Using Machine Learning MethodsyogeshNo ratings yet
- A Practical Guide To Optical Coherence Tomography Angiography InterpretationDocument17 pagesA Practical Guide To Optical Coherence Tomography Angiography InterpretationANIENo ratings yet
- Retinal Disease Classification Using TomograohyDocument13 pagesRetinal Disease Classification Using TomograohyUmakant DodtalleNo ratings yet
- A Viewful Survey: The Neural Network For Blood Cell Image Classification and Diseases IdentificationDocument5 pagesA Viewful Survey: The Neural Network For Blood Cell Image Classification and Diseases IdentificationIJRASETPublicationsNo ratings yet
- Early Diabetic Retinopathy Detection Using Deep Learning AlgorithmsDocument10 pagesEarly Diabetic Retinopathy Detection Using Deep Learning AlgorithmsIJRASETPublicationsNo ratings yet
- MCPANetDocument19 pagesMCPANetpuja maneNo ratings yet
- Detection of Brain HemorrhageDocument8 pagesDetection of Brain HemorrhageIJRASETPublicationsNo ratings yet
- Reconstruction and Visualization of 5m Sectional Coronal Views For Macula Vasculature in OptoVue OCTADocument14 pagesReconstruction and Visualization of 5m Sectional Coronal Views For Macula Vasculature in OptoVue OCTAvahidsmpNo ratings yet
- Ocular Disease Diagnosis in Fundus Images Using Deep LearningDocument6 pagesOcular Disease Diagnosis in Fundus Images Using Deep LearningIJRASETPublicationsNo ratings yet
- Eye PaperDocument5 pagesEye Paperviany leproNo ratings yet
- 3714 11712 1 PB PDFDocument9 pages3714 11712 1 PB PDFSiswo WardoyoNo ratings yet
- Convolutional Neural Network Based Retinal Vessel SegmentationDocument10 pagesConvolutional Neural Network Based Retinal Vessel SegmentationcseijNo ratings yet
- Deep-Learning-Based Automatic Computer-Aided Diagnosis System For Diabetic RetinopathyDocument17 pagesDeep-Learning-Based Automatic Computer-Aided Diagnosis System For Diabetic RetinopathyAsritha ReddyNo ratings yet
- A Novel Approach To The Detection of Macula in Human Retinal ImageryDocument6 pagesA Novel Approach To The Detection of Macula in Human Retinal ImageryRabia SaeedNo ratings yet
- Automated Extraction of Retinal Blood Vessels For Early Diagnosis of Diabetic Retinopathy Using Enhancement Filters and AdaboostDocument9 pagesAutomated Extraction of Retinal Blood Vessels For Early Diagnosis of Diabetic Retinopathy Using Enhancement Filters and AdaboostDr. Sunder Ali KhowajaNo ratings yet
- Intelligence-Based Medicine: Rutuja ShindeDocument15 pagesIntelligence-Based Medicine: Rutuja ShinderNo ratings yet
- Morales 2015Document8 pagesMorales 2015José Micael Delgado BarbosaNo ratings yet
- Detection and Classification of Leukemia Using Deep LearningDocument5 pagesDetection and Classification of Leukemia Using Deep LearningIJRASETPublicationsNo ratings yet
- (IJIT-V6I4P9) :sudharsan KDocument8 pages(IJIT-V6I4P9) :sudharsan KIJITJournalsNo ratings yet
- Automatic Cerebrovascular Segmentation Methods-A ReviewDocument8 pagesAutomatic Cerebrovascular Segmentation Methods-A ReviewIAES IJAINo ratings yet
- DPSF: A Novel Dual Parametric Sigmoid Function For Optical Coherence Tomography Image EnhancementDocument11 pagesDPSF: A Novel Dual Parametric Sigmoid Function For Optical Coherence Tomography Image EnhancementokuwobiNo ratings yet
- Macular OCT Classification Using A Multi-Scale Convolutional Neural Network EnsembleDocument12 pagesMacular OCT Classification Using A Multi-Scale Convolutional Neural Network EnsembleLexNo ratings yet
- AlqudahDocument13 pagesAlqudahSamuel Lozano JuárezNo ratings yet
- Retina Blood Vessel SegmentationDocument28 pagesRetina Blood Vessel SegmentationRevati WableNo ratings yet
- Local Energy Based Shape Histogram (LESH) and Adaboost Machine Learning Techniques To Detect Lung CancerDocument10 pagesLocal Energy Based Shape Histogram (LESH) and Adaboost Machine Learning Techniques To Detect Lung CancerIJRASETPublicationsNo ratings yet
- Pancreas Disease Detection and Segmentation Using Abdominal CT ScanDocument9 pagesPancreas Disease Detection and Segmentation Using Abdominal CT ScanIJAR JOURNALNo ratings yet
- Explainable End-To-End Deep Learning For Diabetic Retinopathy Detection Across Multiple DatasetsDocument25 pagesExplainable End-To-End Deep Learning For Diabetic Retinopathy Detection Across Multiple DatasetsokuwobiNo ratings yet
- Baran Et Al-2016-Journal of BiophotonicsDocument9 pagesBaran Et Al-2016-Journal of BiophotonicsJuan DovalNo ratings yet
- Skin Cancer Detection and Classification Using GUI and Deep Neural NetworkDocument11 pagesSkin Cancer Detection and Classification Using GUI and Deep Neural NetworkIJRASETPublicationsNo ratings yet
- Abbas-Ibrahim2020 Article DenseHyperAnAutomaticRecognitiDocument29 pagesAbbas-Ibrahim2020 Article DenseHyperAnAutomaticRecognitiJaiminGajjarNo ratings yet
- Advancing Opthalmic Diagnostics: U-Net For Retinal Blood Vessel SegmentationDocument8 pagesAdvancing Opthalmic Diagnostics: U-Net For Retinal Blood Vessel SegmentationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Segmentation Errors in Macular Ganglion Cell Analysis As Determined by Optical Coherence Tomography in Eyes With Macular PathologyDocument8 pagesSegmentation Errors in Macular Ganglion Cell Analysis As Determined by Optical Coherence Tomography in Eyes With Macular PathologyMadhu C KNo ratings yet
- Biometric Retina Identification Based On Neural NeDocument8 pagesBiometric Retina Identification Based On Neural NeSyahyusufyNo ratings yet
- Es Unit1Document83 pagesEs Unit1venneti kiranNo ratings yet
- Es Unit1Document83 pagesEs Unit1venneti kiranNo ratings yet
- Ilovepdf MergedDocument12 pagesIlovepdf Mergedvenneti kiranNo ratings yet
- 198 Automatic Diabetic Retinopathy Grading System Basedon Detecting Multiple Retinal LesionsDocument23 pages198 Automatic Diabetic Retinopathy Grading System Basedon Detecting Multiple Retinal Lesionsvenneti kiranNo ratings yet
- Thesis Without SigDocument54 pagesThesis Without Sigvenneti kiranNo ratings yet
- Real Time Applications of Iot in Agriculture: Discussion: Kiran VennetiDocument6 pagesReal Time Applications of Iot in Agriculture: Discussion: Kiran Vennetivenneti kiranNo ratings yet
- Assignment 4Document5 pagesAssignment 4SnehaNo ratings yet
- Owner's Manual Pulsar NS160Document52 pagesOwner's Manual Pulsar NS160arNo ratings yet
- Web Development Internship TaskDocument12 pagesWeb Development Internship TaskradhaNo ratings yet
- British Cost Accounting 1887-1952 PreviewDocument27 pagesBritish Cost Accounting 1887-1952 PreviewJessica JessNo ratings yet
- Electrical Engineering Portal Com Electrical Thumb Rules You Must Follow Part 1Document10 pagesElectrical Engineering Portal Com Electrical Thumb Rules You Must Follow Part 1m khNo ratings yet
- 106資優特訓班Document96 pages106資優特訓班utaNo ratings yet
- Or Or: Correlation Between Carbon Residue and Molecular WeightDocument4 pagesOr Or: Correlation Between Carbon Residue and Molecular WeightNiranjana Murthy PNo ratings yet
- Data Center Cooling SolutionsDocument24 pagesData Center Cooling SolutionsGemelita Ortiz100% (1)
- The Brain's Sense of Movement - Alan BerthozDocument352 pagesThe Brain's Sense of Movement - Alan BerthozKaroline MarxNo ratings yet
- Apartments? Not in My Backyard. Stouffville & Affordable Housing. Presentation To Public HearingDocument14 pagesApartments? Not in My Backyard. Stouffville & Affordable Housing. Presentation To Public HearingArnold Neufeldt-FastNo ratings yet
- Technical Manual Organizational, Direct Support, and General Support Maintenance Repair Parts and Special Tools Lists (Including Depot Maintenance Repair Parts and Special Tools)Document30 pagesTechnical Manual Organizational, Direct Support, and General Support Maintenance Repair Parts and Special Tools Lists (Including Depot Maintenance Repair Parts and Special Tools)Henry PalNo ratings yet
- 32 KV High Voltage Power Transmission Line and Stress On Brassica JunceaDocument4 pages32 KV High Voltage Power Transmission Line and Stress On Brassica Junceamuhammad mushofahNo ratings yet
- Workshop Practical Attendance SheetDocument2 pagesWorkshop Practical Attendance SheetSachidhanandam MNo ratings yet
- Department of Human Services: Course Information Course DescriptionDocument9 pagesDepartment of Human Services: Course Information Course DescriptionS ElburnNo ratings yet
- Question Bank 1st UnitDocument2 pagesQuestion Bank 1st UnitAlapati RajasekharNo ratings yet
- The Journal of The Acoustical Society of AmericaDocument12 pagesThe Journal of The Acoustical Society of Americadr01dNo ratings yet
- Bash SHELL Script in LinuxDocument6 pagesBash SHELL Script in LinuxHesti WidyaNo ratings yet
- All About Immanuel KantDocument20 pagesAll About Immanuel KantSean ChoNo ratings yet
- A Review of Charging Algorithms For Nickel Andlithium - BattersehDocument9 pagesA Review of Charging Algorithms For Nickel Andlithium - BattersehRaghavendra KNo ratings yet
- Weekly Science Report 29th July 2022Document12 pagesWeekly Science Report 29th July 2022John SmithNo ratings yet
- Minatitlan COMPLETE SCOPE - Control ValvesDocument43 pagesMinatitlan COMPLETE SCOPE - Control ValvesErnesto VazquezNo ratings yet
- Ductile-Iron Pressure Pipe: Standard Index of Specifications ForDocument2 pagesDuctile-Iron Pressure Pipe: Standard Index of Specifications ForTamil funNo ratings yet
- Wood Support-Micro Guard Product DataDocument13 pagesWood Support-Micro Guard Product DataM. Murat ErginNo ratings yet
- Ii Week 12 (Seminar)Document30 pagesIi Week 12 (Seminar)ccNo ratings yet
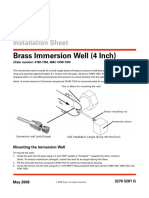
- Brass Immersion Well (4 Inch) : Installation SheetDocument2 pagesBrass Immersion Well (4 Inch) : Installation SheetKim Nicolas SaikiNo ratings yet
- Course Reader For Chapter IiiDocument33 pagesCourse Reader For Chapter Iiipau baniagaNo ratings yet
- Measurement of Hindered Phenolic Antioxidant Content in HL Turbine Oils by Linear Sweep VoltammetryDocument6 pagesMeasurement of Hindered Phenolic Antioxidant Content in HL Turbine Oils by Linear Sweep VoltammetryMohanadNo ratings yet
- Electrostatics DPPDocument10 pagesElectrostatics DPPhimesh2006hNo ratings yet
- Obermeier1985 - Thermal Conductivity, Density, Viscosity, and Prandtl-Numbers of Di - and Tri Ethylene GlycolDocument5 pagesObermeier1985 - Thermal Conductivity, Density, Viscosity, and Prandtl-Numbers of Di - and Tri Ethylene GlycolNgoVietCuongNo ratings yet
- History of Sport PsychologyDocument13 pagesHistory of Sport PsychologyObii DenisNo ratings yet