You might also like
- Complementary and Alternative Medical Lab Testing Part 16: HematologyFrom EverandComplementary and Alternative Medical Lab Testing Part 16: HematologyNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderFrom EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo ratings yet
- Anaemia Protocol 2013Document25 pagesAnaemia Protocol 2013mohamed ElsyedNo ratings yet
- Anaemia in CKDDocument97 pagesAnaemia in CKDsowmiya mohanNo ratings yet
- Anemia in CKDDocument29 pagesAnemia in CKDTee Heng SeongNo ratings yet
- Journal Reading Wajib GastroDocument15 pagesJournal Reading Wajib GastroKarunia Dias BhaskoroNo ratings yet
- Anemia: Reporter: FM R1 余明謙 Supervisor: Dr 陳信儒Document50 pagesAnemia: Reporter: FM R1 余明謙 Supervisor: Dr 陳信儒余明謙No ratings yet
- Anemia CMEDocument64 pagesAnemia CME[ qιlα ]No ratings yet
- Special Report Diagnosis and Management of Iron Deficiency in CKD: A Summary of The NICE Guideline Recommendations and Their RationaleDocument11 pagesSpecial Report Diagnosis and Management of Iron Deficiency in CKD: A Summary of The NICE Guideline Recommendations and Their RationaledrnattoNo ratings yet
- Week 3 PHAR401F16-CKD-3 - (160906) - BBDocument39 pagesWeek 3 PHAR401F16-CKD-3 - (160906) - BBoxyc0n999No ratings yet
- Anemia Management in Peritoneal Dialysis: Perspectives From The Asia Paci Fic RegionDocument7 pagesAnemia Management in Peritoneal Dialysis: Perspectives From The Asia Paci Fic RegionSwingly ThineNo ratings yet
- Renal Association Clinical Practice Guideline On Anaemia of Chronic Kidney DiseaseDocument29 pagesRenal Association Clinical Practice Guideline On Anaemia of Chronic Kidney DiseasemelvinNo ratings yet
- AnemiaFactSheet ANNADocument5 pagesAnemiaFactSheet ANNARahmad HidayatNo ratings yet
- IDA in CKDDocument7 pagesIDA in CKDDr MonikaNo ratings yet
- Besarab 2010Document13 pagesBesarab 2010josephNo ratings yet
- Clinical Practice Guidelines For Evaluation of AnemiaDocument3 pagesClinical Practice Guidelines For Evaluation of Anemiaplease forgive meNo ratings yet
- Guidelines For The Management of Iron Deficiency AnaemiaDocument8 pagesGuidelines For The Management of Iron Deficiency AnaemiaAndrésGuarnizoNo ratings yet
- Iron Deficiency Anemia in Chronic Kidney Disease: ReviewDocument7 pagesIron Deficiency Anemia in Chronic Kidney Disease: ReviewSundas Ejaz100% (1)
- Anemia - PPTX PHDDocument67 pagesAnemia - PPTX PHDReyadh JassemNo ratings yet
- Pi Is 1548559519301144Document20 pagesPi Is 1548559519301144hemer hadyn calderon alvites0% (1)
- Pisani2015 Effect of Oral Liposomal Iron Versus Intravenous Iron PDFDocument8 pagesPisani2015 Effect of Oral Liposomal Iron Versus Intravenous Iron PDFAna Muñoa DuchateauNo ratings yet
- HEMATOLOGY Chapter 20 Rodaks Hematology, 5E (2016)Document14 pagesHEMATOLOGY Chapter 20 Rodaks Hematology, 5E (2016)Sachi Xandria de LaraNo ratings yet
- Joo Sten 2017Document7 pagesJoo Sten 2017langit rizki yuditamaNo ratings yet
- Hemodialysis Treatment in Patients With Severe Electrolyte DisordersDocument8 pagesHemodialysis Treatment in Patients With Severe Electrolyte DisordersRESIDENTES MEDICINA INTERNANo ratings yet
- Diagnosis of Iron Deficiency and Iron Overload Nov 06Document8 pagesDiagnosis of Iron Deficiency and Iron Overload Nov 06Danielcc LeeNo ratings yet
- A Study of Correlation of Serum IronDocument10 pagesA Study of Correlation of Serum Ironraheemrahi089No ratings yet
- Anemia Management in HD PatientsDocument75 pagesAnemia Management in HD PatientsAn TonNo ratings yet
- Kelompok 4A - CBL AnemiaDocument6 pagesKelompok 4A - CBL Anemiacornelia ayuNo ratings yet
- Hematological Manifestations of Connective Tissue Disorders: Aymen OmerDocument69 pagesHematological Manifestations of Connective Tissue Disorders: Aymen OmeraymenNo ratings yet
- Credibility of The Measurement of Serum Ferritin and Transferrin Receptor As Indicators of Iron Deficiency Anemia in Hemodialysis PatientsDocument5 pagesCredibility of The Measurement of Serum Ferritin and Transferrin Receptor As Indicators of Iron Deficiency Anemia in Hemodialysis PatientsTanveerNo ratings yet
- Elevated Ferritin What Should GP KnowDocument5 pagesElevated Ferritin What Should GP KnowDanielcc LeeNo ratings yet
- Low Alt CKDDocument5 pagesLow Alt CKDFebianti RukmanaNo ratings yet
- Case Challenge: Diagnosing and Managing CKD Comorbidities: Literature ReviewDocument8 pagesCase Challenge: Diagnosing and Managing CKD Comorbidities: Literature ReviewPratik TripathiNo ratings yet
- !!NEW DR Lausevic 20200714-003Document4 pages!!NEW DR Lausevic 20200714-003assialnadaweeNo ratings yet
- Case Questions TranscriptDocument7 pagesCase Questions TranscriptSa7arNo ratings yet
- Erythropoietin (EPO) : Treatment and Monitoring GuidelineDocument15 pagesErythropoietin (EPO) : Treatment and Monitoring GuidelineGagah BrillianNo ratings yet
- Anemia in CKDDocument9 pagesAnemia in CKDM. Ryan RamadhanNo ratings yet
- Iron DeficiencyDocument9 pagesIron DeficiencyJohn TorresNo ratings yet
- 1-3 Meta AnalysisDocument81 pages1-3 Meta Analysismarryskye9No ratings yet
- How I Treat Renal AnemiaDocument7 pagesHow I Treat Renal AnemiaCsr ArsNo ratings yet
- Jurnal AnastesiDocument12 pagesJurnal AnastesilissamariasianiparNo ratings yet
- Molecular Mechanisms of Hepcidin Regulation - Implications For The Anemia of CKDDocument16 pagesMolecular Mechanisms of Hepcidin Regulation - Implications For The Anemia of CKDGading AuroraNo ratings yet
- ANEMIA Pada Penyakit KronikDocument14 pagesANEMIA Pada Penyakit KronikAndrie WigunaNo ratings yet
- ACCP 2018 NephrologyDocument31 pagesACCP 2018 NephrologyMonica Febri Andari100% (1)
- Clinical Hematological: Assist Prof. Dr. Mudhir S. ShekhaDocument31 pagesClinical Hematological: Assist Prof. Dr. Mudhir S. ShekhaAhmed. Masud.OthmanNo ratings yet
- Meta Analisis StudiDocument13 pagesMeta Analisis StudiShafira Maulani putriNo ratings yet
- Boston Medical Center Maternity Care Guideline Guideline: Iron Defficiency Anemia Accepted: Updated: 04/2015Document4 pagesBoston Medical Center Maternity Care Guideline Guideline: Iron Defficiency Anemia Accepted: Updated: 04/2015Fernando Cardenas AriasNo ratings yet
- Amiodarone-Induced Hypothyroidism With EPO-resistant Anemia in A Patient With Chronic Renal FailureDocument3 pagesAmiodarone-Induced Hypothyroidism With EPO-resistant Anemia in A Patient With Chronic Renal Failureeki_megaraniNo ratings yet
- MISDC AnaemiaDocument33 pagesMISDC AnaemiawanyNo ratings yet
- Anemia in CKD (B BATCH)Document16 pagesAnemia in CKD (B BATCH)Mayank SharmaNo ratings yet
- Prevalence of Anemia Among Chronic Kidney Disease Patients in India: Single Centre StudyDocument6 pagesPrevalence of Anemia Among Chronic Kidney Disease Patients in India: Single Centre StudyAbdullah ZaawariNo ratings yet
- Using The Hemoglobin Content of Reticulocytes (RET-He) To Evaluate Anemia in Patients With CancerDocument7 pagesUsing The Hemoglobin Content of Reticulocytes (RET-He) To Evaluate Anemia in Patients With CancerMekar PalupiNo ratings yet
- Anaemia Management in People With Chronic Kidney Disease Anaemia Management in People With Chronic Kidney Disease OverviewDocument9 pagesAnaemia Management in People With Chronic Kidney Disease Anaemia Management in People With Chronic Kidney Disease Overviewraheemrahi089No ratings yet
- Soppi 2018Document5 pagesSoppi 2018dr_joe23No ratings yet
- Anaemia of Chronic Renal DiseaseDocument9 pagesAnaemia of Chronic Renal DiseaseVitabuNo ratings yet
- Hyperkalemia Associated With Use of Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor BlockersDocument11 pagesHyperkalemia Associated With Use of Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor BlockersdarekshepardNo ratings yet
- Diagnosis and Treatment of Iron Deficiency Anemia (IDA)Document7 pagesDiagnosis and Treatment of Iron Deficiency Anemia (IDA)Abdullah EssaNo ratings yet
- Anemia in Critically Ill and Perioperatif PatientsDocument20 pagesAnemia in Critically Ill and Perioperatif PatientsDeviana HidayatiNo ratings yet
- Anemia of Chronic DiseaseDocument5 pagesAnemia of Chronic DiseaseGufront MustofaNo ratings yet
- Reviews: Management of Hyperkalaemia in Chronic Kidney DiseaseDocument10 pagesReviews: Management of Hyperkalaemia in Chronic Kidney Diseasebagir_dm10No ratings yet
- GHTF sg1 n045 2008 Principles Ivd Medical Devices Classification 080219Document15 pagesGHTF sg1 n045 2008 Principles Ivd Medical Devices Classification 080219DeepaNo ratings yet
- Mineral HomeostasisDocument6 pagesMineral HomeostasisDeepaNo ratings yet
- Additive Impact of Alfacalcidol On Bone Mineral DensityDocument12 pagesAdditive Impact of Alfacalcidol On Bone Mineral DensityDeepaNo ratings yet
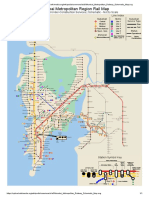
- Mumbai Metropolitan Railway Schematic MapDocument1 pageMumbai Metropolitan Railway Schematic MapDeepaNo ratings yet
- JCM 11 04676 v2Document14 pagesJCM 11 04676 v2DeepaNo ratings yet
- Professional Development Objectives Related To Modalities Specific TopicsDocument3 pagesProfessional Development Objectives Related To Modalities Specific TopicsCris100% (1)
- Engineering Mathematics Questions and AnswersDocument9 pagesEngineering Mathematics Questions and AnswersZaky Muzaffar100% (1)
- Lesson Plan Wid Awt Method 2Document7 pagesLesson Plan Wid Awt Method 2Yan LianNo ratings yet
- File 1) GRE 2009 From - Nov - 18 PDFDocument84 pagesFile 1) GRE 2009 From - Nov - 18 PDFhuyly34No ratings yet
- APS PresentationDocument32 pagesAPS PresentationRozack Ya ZhackNo ratings yet
- Micro Fibra Sintetica at 06-MapeiDocument2 pagesMicro Fibra Sintetica at 06-MapeiSergio GonzalezNo ratings yet
- THE Ketofeed Diet Book v2Document43 pagesTHE Ketofeed Diet Book v2jacosta12100% (1)
- CE Laws L8 L15Document470 pagesCE Laws L8 L15Edwin BernatNo ratings yet
- (Essential Skills For Nurses Series) Philippa Sully - Joan Dallas-Essential Communication Skills For Nursing and Midwifery-Mosby - Elsevier (2010) PDFDocument250 pages(Essential Skills For Nurses Series) Philippa Sully - Joan Dallas-Essential Communication Skills For Nursing and Midwifery-Mosby - Elsevier (2010) PDFRetno SumaraNo ratings yet
- Talent-Olympiad 9 Science SampleDocument12 pagesTalent-Olympiad 9 Science SampleFire GamingNo ratings yet
- Glossary of Terms 2nd PartDocument2 pagesGlossary of Terms 2nd Part2DJoyce D.N CapacieteNo ratings yet
- Nursing EnglishDocument139 pagesNursing EnglishSara Williams100% (3)
- AR Financial StatementsDocument281 pagesAR Financial StatementsISHA AGGARWALNo ratings yet
- Bank OD Account in Tally 1Document3 pagesBank OD Account in Tally 1yashusahu180No ratings yet
- Dphs Freshman Course List 2024-25Document1 pageDphs Freshman Course List 2024-25api-337771649No ratings yet
- 3rd Quarter SUMMATIVE TEST in MAPEHDocument3 pages3rd Quarter SUMMATIVE TEST in MAPEHzaile felineNo ratings yet
- I - Pronunciation Choose The Word Whose Stress Pattern Is Different From The Other Three in The Following QuestionsDocument6 pagesI - Pronunciation Choose The Word Whose Stress Pattern Is Different From The Other Three in The Following QuestionsHaNo ratings yet
- FO - Course Transition Info - Acknowledgement - SIT50422 - Dip Hospitality Management - V1Document2 pagesFO - Course Transition Info - Acknowledgement - SIT50422 - Dip Hospitality Management - V1nitesh.kc06No ratings yet
- Caterpillar Sis (01.2014) MultilanguageDocument10 pagesCaterpillar Sis (01.2014) MultilanguageTemmy Candra Wijaya100% (1)
- Panel Hospital List IGIDocument6 pagesPanel Hospital List IGIAbdul RahmanNo ratings yet
- RSM222.f22.CourseOutline v3 2022-09-05Document9 pagesRSM222.f22.CourseOutline v3 2022-09-05Kirsten WangNo ratings yet
- PROP CASES OUTLINE 7 - Right of Way - Light & ViewDocument108 pagesPROP CASES OUTLINE 7 - Right of Way - Light & ViewKringle Lim - DansalNo ratings yet
- DocumentationDocument44 pagesDocumentation19-512 Ratnala AshwiniNo ratings yet
- H I Ôn Thi Aptis & Vstep - Tài Liệu - Anna MaiDocument4 pagesH I Ôn Thi Aptis & Vstep - Tài Liệu - Anna Maihanh.mt2022No ratings yet
- Cyrille MATH INVESTIGATION Part2Document18 pagesCyrille MATH INVESTIGATION Part2Jessie jorgeNo ratings yet
- CalculusDocument101 pagesCalculuskusnoNo ratings yet
- Police Cranston School Committee Member Stole PTO FundsDocument1 pagePolice Cranston School Committee Member Stole PTO FundsashaydelineNo ratings yet
- A Control Method For Power-Assist Devices Using A BLDC Motor For Manual WheelchairsDocument7 pagesA Control Method For Power-Assist Devices Using A BLDC Motor For Manual WheelchairsAhmed ShoeebNo ratings yet
- SS EN 1991-1-1-2008 (2017) - PreviewDocument16 pagesSS EN 1991-1-1-2008 (2017) - PreviewNg SHun JieNo ratings yet
- Handbook - European Choral AssociationDocument24 pagesHandbook - European Choral AssociationMonica SaenzNo ratings yet