You might also like
- Goulds Pathophysiology For The Health Professions 6th Edition Vanmeter Test BankDocument8 pagesGoulds Pathophysiology For The Health Professions 6th Edition Vanmeter Test BankJessicaHardysrbxd100% (11)
- Vocabulary Success C1 - SAMPLE PAGES PDFDocument17 pagesVocabulary Success C1 - SAMPLE PAGES PDFAndreas Badeiro100% (1)
- Osteosarcoma of The Jaw An Analysis of A Series of 74 Cases (2013)Document8 pagesOsteosarcoma of The Jaw An Analysis of A Series of 74 Cases (2013)sTEVENNo ratings yet
- 95 123 3 PBDocument6 pages95 123 3 PBNeggy YudibrataNo ratings yet
- Ewings Sarcoma - DescriptionDocument3 pagesEwings Sarcoma - DescriptionDamodara KumaranNo ratings yet
- Osteo Blast OmaDocument5 pagesOsteo Blast OmamandetoperdiyuwanNo ratings yet
- Spindle Cell Tumor in Oral Cavity: A Rare Case Report: Ase EportDocument4 pagesSpindle Cell Tumor in Oral Cavity: A Rare Case Report: Ase EportDeka Dharma PutraNo ratings yet
- Sarcoma de Ewing S NEJMDocument11 pagesSarcoma de Ewing S NEJMbanzethyskyNo ratings yet
- Hyl 142Document11 pagesHyl 142Stefania CristinaNo ratings yet
- CA LS Bướu Nhiều Hốc - Multilocular Radiolucency in the Body of MandibleDocument4 pagesCA LS Bướu Nhiều Hốc - Multilocular Radiolucency in the Body of MandibleThành Luân NguyễnNo ratings yet
- International 4Document4 pagesInternational 4daffunkmadansyahNo ratings yet
- 7 OsteosarcomaDocument4 pages7 OsteosarcomaDodNo ratings yet
- Salivary Glands Neoplasms: Artigo de RevisãoDocument10 pagesSalivary Glands Neoplasms: Artigo de RevisãoCeriaindriasariNo ratings yet
- Bilateral Odontogenic Keratocyst in A NonsyndromicDocument5 pagesBilateral Odontogenic Keratocyst in A NonsyndromicRocio CacñahuarayNo ratings yet
- Solitary Central Osteoma of Mandible in A Geriatric Patient: Report and ReviewDocument4 pagesSolitary Central Osteoma of Mandible in A Geriatric Patient: Report and ReviewNurul SalsabilaNo ratings yet
- Lateral Periodontal CystDocument8 pagesLateral Periodontal CystTejas KulkarniNo ratings yet
- Occlusal CaseDocument3 pagesOcclusal CaseLatifa Hanif ZuhriNo ratings yet
- mooneAMS 3 66Document6 pagesmooneAMS 3 66dikiprestya391No ratings yet
- Chronic Recurrent Multifocal Osteomyelitis in Association With Pyoderma GangraenosumDocument7 pagesChronic Recurrent Multifocal Osteomyelitis in Association With Pyoderma GangraenosumDha Dina SevofrationNo ratings yet
- 9 PDFDocument3 pages9 PDFDennis hayonNo ratings yet
- Odontogenic Myxoma A Rare Case ReportDocument3 pagesOdontogenic Myxoma A Rare Case Reportvictorubong404No ratings yet
- Frequency of Impacted Canines in Orthodontic Patients Presenting To Armed Forces Institute of DentistryDocument4 pagesFrequency of Impacted Canines in Orthodontic Patients Presenting To Armed Forces Institute of DentistryJuseel López JulcaNo ratings yet
- AAOS2002 TumorDocument59 pagesAAOS2002 TumorHizkyas KassayeNo ratings yet
- Pof CR4Document5 pagesPof CR4Swab IndonesiaNo ratings yet
- Follicular With Plexiform Ameloblastoma in Anterior Mandible: Report of Case and Literature ReviewDocument6 pagesFollicular With Plexiform Ameloblastoma in Anterior Mandible: Report of Case and Literature Reviewluckytung07No ratings yet
- Osteosarcoma of Mandible: Abst TDocument3 pagesOsteosarcoma of Mandible: Abst TTriLightNo ratings yet
- Odontoma Compound 1Document4 pagesOdontoma Compound 1ashariNo ratings yet
- OsteomaDocument3 pagesOsteomaKHAIRUNISA RAHMA HANDAYANI HANDAYANINo ratings yet
- Cabt 12 I 5 P 45Document6 pagesCabt 12 I 5 P 45abeer alrofaeyNo ratings yet
- Oral Rhabdomyosarcoma A Case Report 2161 0681 3 161Document4 pagesOral Rhabdomyosarcoma A Case Report 2161 0681 3 161Nabila RizkikaNo ratings yet
- Odontogenic Cysts and Odontogenic Tumors in A Large Rural Area From India. A 10-Year ReflectionDocument5 pagesOdontogenic Cysts and Odontogenic Tumors in A Large Rural Area From India. A 10-Year ReflectionAlan VargasNo ratings yet
- Multiple Bilateral Taurodontism. A Case ReportDocument3 pagesMultiple Bilateral Taurodontism. A Case ReportJing XueNo ratings yet
- Unusual Clinicoradiographic Presentation of A Lateral Periodontal CystDocument5 pagesUnusual Clinicoradiographic Presentation of A Lateral Periodontal CystTzitzi FloresNo ratings yet
- Unilateral Mandibular Swelling in A Young Female Patient A Case ReportDocument4 pagesUnilateral Mandibular Swelling in A Young Female Patient A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intra-Oral Lingual Schwannoma - A Rare Case Report From An Indian Tertiary Care HospitalDocument3 pagesIntra-Oral Lingual Schwannoma - A Rare Case Report From An Indian Tertiary Care HospitalIJAR JOURNALNo ratings yet
- Nasopalatine Duct Cyst: Report of A Case With Review of LiteratureDocument4 pagesNasopalatine Duct Cyst: Report of A Case With Review of LiteratureKaty LunaNo ratings yet
- Ojsadmin, 1340Document4 pagesOjsadmin, 1340Dr NisrinNo ratings yet
- Cureus 0012 00000008418Document10 pagesCureus 0012 00000008418فرجني موغNo ratings yet
- Gilan Jindexedin ISCDocument7 pagesGilan Jindexedin ISCfavorendaNo ratings yet
- A Giant Peripheral Ossifying Fibroma of The - 2024 - International Journal of SDocument5 pagesA Giant Peripheral Ossifying Fibroma of The - 2024 - International Journal of SRonald QuezadaNo ratings yet
- Alshagroud2017 Article MetastasizingPleomorphicAdenomDocument7 pagesAlshagroud2017 Article MetastasizingPleomorphicAdenommawarmelatiNo ratings yet
- Osteoblastoma of The JawsDocument3 pagesOsteoblastoma of The JawsAngelia PratiwiNo ratings yet
- NigerJClinPract244483-3890557 104825Document6 pagesNigerJClinPract244483-3890557 104825CalvintNo ratings yet
- JDS 17 370Document15 pagesJDS 17 370Ferry HendrawanNo ratings yet
- 70 - Review Article PDFDocument5 pages70 - Review Article PDFHandiniNo ratings yet
- Tripathy 2015Document19 pagesTripathy 2015Someshwar GuptNo ratings yet
- Pulpitis JurnalDocument2 pagesPulpitis JurnalIsmail YusufNo ratings yet
- Case Report - Non Ossifying Fibroma of TibiaDocument3 pagesCase Report - Non Ossifying Fibroma of TibiaChristabella Natalia WijayaNo ratings yet
- Bonnie Vorasubin, MD Arthur Wu, MD Chi Lai, MD Elliot Abemayor, MD, PHDDocument1 pageBonnie Vorasubin, MD Arthur Wu, MD Chi Lai, MD Elliot Abemayor, MD, PHDmandible removerNo ratings yet
- Ameloblastic Fibroma: Report of A Case: Su-Gwan Kim, DDS, PHD, and Hyun-Seon Jang, DDS, PHDDocument3 pagesAmeloblastic Fibroma: Report of A Case: Su-Gwan Kim, DDS, PHD, and Hyun-Seon Jang, DDS, PHDdoktergigikoeNo ratings yet
- Giant CellDocument5 pagesGiant CellTamimahNo ratings yet
- Lapsus Journal OriginalDocument5 pagesLapsus Journal Originalrozi piresNo ratings yet
- Lateral Periodontal Cyst: Report of Case and Review of The LiteratureDocument5 pagesLateral Periodontal Cyst: Report of Case and Review of The LiteraturePutri Bella KharismaNo ratings yet
- Case Report Malignant Peripheral Nerve Sheath Tumor of SinonasalDocument84 pagesCase Report Malignant Peripheral Nerve Sheath Tumor of SinonasalAyunita ArifinNo ratings yet
- Central Giant Cell Granuloma A Potential Endodontic MisdiagnosisDocument3 pagesCentral Giant Cell Granuloma A Potential Endodontic MisdiagnosisDr.O.R.GANESAMURTHINo ratings yet
- Mature Cystic Teratoma of The Right Cerebellopontine Angle A Rare Case ReportDocument5 pagesMature Cystic Teratoma of The Right Cerebellopontine Angle A Rare Case ReportHaribabuBabuNo ratings yet
- Case Report - Craniofacial Fibrous Dysplasia With Aneurysmal Bone Cyst: A Rare CoexistenceDocument3 pagesCase Report - Craniofacial Fibrous Dysplasia With Aneurysmal Bone Cyst: A Rare CoexistenceSachin HosamaniNo ratings yet
- Systemic Lupus Erythematosus and Hearing Disorders: Literature Review and Meta-Analysis of Clinical and Temporal Bone FindingsDocument11 pagesSystemic Lupus Erythematosus and Hearing Disorders: Literature Review and Meta-Analysis of Clinical and Temporal Bone FindingsLNo ratings yet
- Article-Ossifying Fibroma in The Maxilla and MandibleDocument12 pagesArticle-Ossifying Fibroma in The Maxilla and MandibleMaged NabilNo ratings yet
- Calcifying Epithelial Odontogenic Tumor - A CaseDocument5 pagesCalcifying Epithelial Odontogenic Tumor - A CaseKharismaNisaNo ratings yet
- International Journal of Dental Science and Innovative Research (IJDSIR)Document7 pagesInternational Journal of Dental Science and Innovative Research (IJDSIR)bella07ciaoNo ratings yet
- Diagnostic Problems in Tumors of Head and Neck: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Head and Neck: Selected TopicsRating: 5 out of 5 stars5/5 (1)
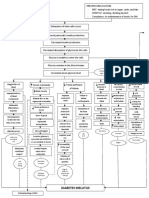
- Diabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)Document3 pagesDiabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)John Henry ValenciaNo ratings yet
- Indranila 2021Document22 pagesIndranila 2021reski utamiNo ratings yet
- Health Law BibliographyDocument11 pagesHealth Law BibliographyIeien MuthmainnahNo ratings yet
- Pe Sacroiliac Joint PainDocument2 pagesPe Sacroiliac Joint Painusama_yasinNo ratings yet
- NCPDocument3 pagesNCPJyn Jyn0% (1)
- Sensorium.: NiirDocument6 pagesSensorium.: NiirSundar RajanNo ratings yet
- Abnormal Psychology: Historical and Modern Perspectives: Total Assessment Guide (T.A.G.)Document29 pagesAbnormal Psychology: Historical and Modern Perspectives: Total Assessment Guide (T.A.G.)Rachelle SalcedoNo ratings yet
- Biology QuestionsDocument41 pagesBiology QuestionsB.srihariNo ratings yet
- HY RenalDocument50 pagesHY RenalJeniNo ratings yet
- Cholera Philippine Setting.Document1 pageCholera Philippine Setting.Lara TechiesNo ratings yet
- School Form 8 SF8 Learner Basic Health and Nutrition ReportDocument10 pagesSchool Form 8 SF8 Learner Basic Health and Nutrition ReportRey Moca100% (1)
- Neuromuscular Junction Disorders: Myasthenia GravisDocument20 pagesNeuromuscular Junction Disorders: Myasthenia GravisIzabella MihályNo ratings yet
- RestimeDocument3 pagesRestimekaiserdarkNo ratings yet
- Cardiology-5 DysrhythmiaDocument16 pagesCardiology-5 DysrhythmiaMahmoud RamadanNo ratings yet
- A Study On Impact of COVID-19 Lockdown On Psychological Health, Economy and Social Life of People in KashmirDocument12 pagesA Study On Impact of COVID-19 Lockdown On Psychological Health, Economy and Social Life of People in KashmirDavit SoesantoNo ratings yet
- MEDSURG Topic 1 10 A Cauti 1Document26 pagesMEDSURG Topic 1 10 A Cauti 1VINCE KHALID ASARAL ABDULLAHNo ratings yet
- Effect of Nateglinide On The Incidence of DiabetesDocument31 pagesEffect of Nateglinide On The Incidence of Diabetesfred opinionNo ratings yet
- Physical Edu. Revised Notes - 2023-24Document96 pagesPhysical Edu. Revised Notes - 2023-24bhaisahabjino.1No ratings yet
- L12.1-OB-Intrapartum Assessment (Nov1221)Document9 pagesL12.1-OB-Intrapartum Assessment (Nov1221)Erald PaderangaNo ratings yet
- Lecture 7 Acupuncture Acupressure 2020S2 - StudentDocument39 pagesLecture 7 Acupuncture Acupressure 2020S2 - StudentAyeitzreg100% (2)
- Hs Sexlinked InheritanceDocument14 pagesHs Sexlinked InheritanceMarcelo Pessoa NetoNo ratings yet
- Broward Teachers Union Lawsuit Against School DistrictDocument18 pagesBroward Teachers Union Lawsuit Against School DistrictMichelle SolomonNo ratings yet
- Microorganism and Their Effects On Living ThingDocument16 pagesMicroorganism and Their Effects On Living ThingrubihambaliNo ratings yet
- COVID-19 AWARENESS PPT FinalDocument37 pagesCOVID-19 AWARENESS PPT FinalFranz goNo ratings yet
- EWMA Lower Leg Ulcer Diagnosis SuppDocument76 pagesEWMA Lower Leg Ulcer Diagnosis SuppAna CayumilNo ratings yet
- Fit Well Core Concepts and Labs in Physical Fitness and Wellness 13Th Edition Full ChapterDocument41 pagesFit Well Core Concepts and Labs in Physical Fitness and Wellness 13Th Edition Full Chapterwilliam.decker273100% (26)
- Aortic Valve Stenosis A D A7Document15 pagesAortic Valve Stenosis A D A7Ahmed DsoukiNo ratings yet
- A Dentist Exposes The Root Canal Cover Up PDFDocument1 pageA Dentist Exposes The Root Canal Cover Up PDFhanalei77No ratings yet