You might also like
- ASME Geometric Dimension Ing and Tolerance Professional CertificationDocument20 pagesASME Geometric Dimension Ing and Tolerance Professional CertificationPaul Anthony Red60% (5)
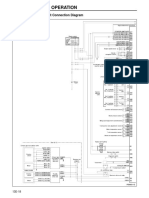
- Structure and Operation: 3. Electronic Control Unit Connection DiagramDocument16 pagesStructure and Operation: 3. Electronic Control Unit Connection DiagramAung Hlaing Min MyanmarNo ratings yet
- ENIRAM - Guide To Dynamic Trim Optimization 280611 PDFDocument14 pagesENIRAM - Guide To Dynamic Trim Optimization 280611 PDFPhineas MagellanNo ratings yet
- Ground Architecture (Mourad Medhat)Document146 pagesGround Architecture (Mourad Medhat)Aída SousaNo ratings yet
- Hospital Acquired PneumoniaDocument48 pagesHospital Acquired PneumoniaKartika RezkyNo ratings yet
- Shear and Diagonal Tension in BeamDocument16 pagesShear and Diagonal Tension in BeamMouy PhonThornNo ratings yet
- Occupational Therapy Examination Review Guide 4th Edition Ebook PDFDocument57 pagesOccupational Therapy Examination Review Guide 4th Edition Ebook PDFrobert.campbell485No ratings yet
- DIAGNOSIS OF TUBERCULOSIS DR T V RaoDocument63 pagesDIAGNOSIS OF TUBERCULOSIS DR T V Raotummalapalli venkateswara rao100% (2)
- P&G Interview QuestionsDocument2 pagesP&G Interview Questionssupu100% (3)
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Introduction To Waterborne PathogensDocument60 pagesIntroduction To Waterborne PathogensSyed Alwi Alattas100% (1)
- Module 6 - Using and Evaluating Instructional MaterialsDocument5 pagesModule 6 - Using and Evaluating Instructional MaterialsMaria Victoria Padro100% (4)
- ISO 20000-1 Gap Analysis QuestionaireDocument15 pagesISO 20000-1 Gap Analysis QuestionaireUsman Hamid67% (6)
- Gastrointestinal Endoscopes:: A Need To Shift From Disinfection To SterilizationDocument41 pagesGastrointestinal Endoscopes:: A Need To Shift From Disinfection To SterilizationdrelvNo ratings yet
- JMV 25666Document5 pagesJMV 25666Nathalia LedesmaNo ratings yet
- 209 Full PDFDocument8 pages209 Full PDFAngga PratamaNo ratings yet
- Artigo 03 Filmarray PneumoniaDocument6 pagesArtigo 03 Filmarray Pneumoniapriscila pimentel martinelliNo ratings yet
- 1 s2.0 S0009898121004009 MainDocument6 pages1 s2.0 S0009898121004009 MainRonaldo SilvaNo ratings yet
- Week4 1Document105 pagesWeek4 1dyah ayu shinta lesmanawatiNo ratings yet
- HC610-00-UK BALLARD Mini-BAL SelectedEvidenceBooklet COPY-05459 2021Document20 pagesHC610-00-UK BALLARD Mini-BAL SelectedEvidenceBooklet COPY-05459 2021Popescu ValiNo ratings yet
- Journal Acute Necrotizing Ulcerating Gingivitis On HIV PatientDocument5 pagesJournal Acute Necrotizing Ulcerating Gingivitis On HIV PatientginNo ratings yet
- Unexpected Acute Necrotizing Ulcerative Gingivitis in A Well-Controlled HIV-infected CaseDocument5 pagesUnexpected Acute Necrotizing Ulcerative Gingivitis in A Well-Controlled HIV-infected CasecatharineeSANo ratings yet
- The Ability of Two Chlorine Dioxide Chemistries To Inactivate Human Papillomavirus-Contaminated Endocavitary Ultrasound Probes and NasendoscopesDocument11 pagesThe Ability of Two Chlorine Dioxide Chemistries To Inactivate Human Papillomavirus-Contaminated Endocavitary Ultrasound Probes and NasendoscopesNathalia LedesmaNo ratings yet
- Estudio Corona 1 Ropa41-7-E67Document5 pagesEstudio Corona 1 Ropa41-7-E67eudaldoNo ratings yet
- Ventilator-Associated Tracheobronchitis and Pneumonia: Thinking Outside The BoxDocument8 pagesVentilator-Associated Tracheobronchitis and Pneumonia: Thinking Outside The BoxRoberto Linhares de FreitasNo ratings yet
- European Guidelines For Urinalysis A CollaborativeDocument7 pagesEuropean Guidelines For Urinalysis A CollaborativeTaufan LutfiNo ratings yet
- A Study On Ventilator Associated Pneumonia inDocument4 pagesA Study On Ventilator Associated Pneumonia inAl MuzakkiNo ratings yet
- Artykul Do Wytycznych PDFDocument7 pagesArtykul Do Wytycznych PDFEla BąkNo ratings yet
- 1 s2.0 S0195670118305425 MainDocument4 pages1 s2.0 S0195670118305425 MainMuhammad Cholid AlfahroziNo ratings yet
- 1 s2.0 S1198743X18308565 MainDocument6 pages1 s2.0 S1198743X18308565 MainYulia Niswatul FauziyahNo ratings yet
- DeseasDocument3 pagesDeseasTewodros abayneh TeddyNo ratings yet
- Piis1201971216312292 2Document3 pagesPiis1201971216312292 2Soraya Eugenia Morales LópezNo ratings yet
- Bovine Tuberculosis: Occupational Hazard in Abattoir WorkersDocument6 pagesBovine Tuberculosis: Occupational Hazard in Abattoir WorkersIOSRjournalNo ratings yet
- Molecular Analysis of Bacterial Contamination On Stethoscopes in An Intensive Care UnitDocument7 pagesMolecular Analysis of Bacterial Contamination On Stethoscopes in An Intensive Care UnitletuslearnNo ratings yet
- Westenbrink2015Document6 pagesWestenbrink2015rameshNo ratings yet
- JCM 02589-20Document3 pagesJCM 02589-20NorellaNo ratings yet
- Diagnostic Performance of DifferentDocument10 pagesDiagnostic Performance of Differentq8xx75sjnyNo ratings yet
- Human Infection With Delftia Tsuruhatensis Isolated From A Central Venous CatheterDocument3 pagesHuman Infection With Delftia Tsuruhatensis Isolated From A Central Venous CatheterRENE RIVASNo ratings yet
- Ultimos AntimicrobianosDocument3 pagesUltimos Antimicrobianosmargarita rodriguezNo ratings yet
- Prevention of HAI IndonesienDocument208 pagesPrevention of HAI IndonesienLipun SethiNo ratings yet
- Survival of Human Coronaviruses 229E and OC43 in Suspension and After Drying On Surfaces: A Possible Source of Hospital-Acquired InfectionsDocument6 pagesSurvival of Human Coronaviruses 229E and OC43 in Suspension and After Drying On Surfaces: A Possible Source of Hospital-Acquired InfectionsR JNo ratings yet
- Jurnal 2Document10 pagesJurnal 2GFORCE .ID.No ratings yet
- Ultraviolet Germicidal IrradiatDocument12 pagesUltraviolet Germicidal IrradiatIsfihanNo ratings yet
- Oseltamivir For Coronavirus Illness:: ResearchDocument6 pagesOseltamivir For Coronavirus Illness:: ResearchellaNo ratings yet
- Patogenos BacterianosDocument7 pagesPatogenos BacterianosHumberto QuinteroNo ratings yet
- 3B - COVID-19 Update - April 2020Document40 pages3B - COVID-19 Update - April 2020Tuệ HoàngNo ratings yet
- JCM 02881-20Document17 pagesJCM 02881-20SariSyahruniNo ratings yet
- Jurnal Mikro-2Document8 pagesJurnal Mikro-2Mila KarmilaNo ratings yet
- Laryngeal Complications of COVID-19Document8 pagesLaryngeal Complications of COVID-19Mariana BarrosNo ratings yet
- Fcimb 13 1131241Document11 pagesFcimb 13 1131241syavinaNo ratings yet
- Sars-Cov-2 Presence in The Saliva, Tears, and Cerumen of Covid-19 PatientsDocument6 pagesSars-Cov-2 Presence in The Saliva, Tears, and Cerumen of Covid-19 PatientsMuhammad ihsan arifNo ratings yet
- Case Study 2Document5 pagesCase Study 2Sanjeev KushwahaNo ratings yet
- Suspected Urinary Tract Infection in Primary Care, DenmarkDocument6 pagesSuspected Urinary Tract Infection in Primary Care, DenmarkImelda Nafa PawestriNo ratings yet
- Neocon 2017Document71 pagesNeocon 2017Jasleen KaurNo ratings yet
- JurnalDocument6 pagesJurnalDaffa AthaNo ratings yet
- PIIS1198743X20306972Document4 pagesPIIS1198743X20306972KARLA PATRICIA DIAZ LOPEZNo ratings yet
- Antimicrobial Susceptibility Among Pathogens Isolated in Early-Versus Late-Onset Ventilator-Associated PneumoniaDocument10 pagesAntimicrobial Susceptibility Among Pathogens Isolated in Early-Versus Late-Onset Ventilator-Associated PneumoniaJeremy CNo ratings yet
- Tuberculosis of The Nasal Cavities About Four CasesDocument5 pagesTuberculosis of The Nasal Cavities About Four CasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jurnal 20Document5 pagesJurnal 20Ahmad Fari Arief LopaNo ratings yet
- Minor Diagnostic Factors in Ventilator Associated Pneumonia in ChildrenDocument9 pagesMinor Diagnostic Factors in Ventilator Associated Pneumonia in ChildrenmariskaNo ratings yet
- DR - PARTHA - 2018 Clinical Microbiology II PDFDocument88 pagesDR - PARTHA - 2018 Clinical Microbiology II PDFNuzki YofandaNo ratings yet
- Community-Acquired Lung Respiratory Infections in HIV-infected Patients: Microbial Aetiology and OutcomeDocument11 pagesCommunity-Acquired Lung Respiratory Infections in HIV-infected Patients: Microbial Aetiology and OutcomeMuchamad Nur HadiNo ratings yet
- Respiratory Specimen Collection and ProcessingDocument20 pagesRespiratory Specimen Collection and ProcessingJose Adan Vazquez MoralesNo ratings yet
- Neves Siqueira 2016Document5 pagesNeves Siqueira 2016Rbdoin AabdNo ratings yet
- Streptococcal Tonsillitis As A Cause of Urticaria Tonsillitis and UrticariaDocument5 pagesStreptococcal Tonsillitis As A Cause of Urticaria Tonsillitis and UrticariasDamnNo ratings yet
- Nosocomial Infections in Pediatric Intensive Care UnitDocument6 pagesNosocomial Infections in Pediatric Intensive Care UnitEditor IJTSRDNo ratings yet
- Acute Viral Bacterial Rs ManagementDocument30 pagesAcute Viral Bacterial Rs ManagementDayita ApritutiNo ratings yet
- International Journal of Infectious Diseases: SciencedirectDocument7 pagesInternational Journal of Infectious Diseases: SciencedirectKinja NinjaNo ratings yet
- Community-Acquired Pneumonia in The Emergency DepartmentDocument7 pagesCommunity-Acquired Pneumonia in The Emergency DepartmentpachomdNo ratings yet
- Avinash Uttareshwar MeherDocument6 pagesAvinash Uttareshwar MeheravinashNo ratings yet
- 50+ MATLAB Projects For Engineering StudentsDocument5 pages50+ MATLAB Projects For Engineering StudentsaamyaNo ratings yet
- Miracle Mills 300 Series Hammer MillsDocument2 pagesMiracle Mills 300 Series Hammer MillsSNo ratings yet
- VSR Trans. PPT3Document16 pagesVSR Trans. PPT3VSR TRANSNo ratings yet
- Original Research PapersDocument13 pagesOriginal Research Papersrikaseo rikaNo ratings yet
- PTN Guide Compilation by EmeraldchowDocument24 pagesPTN Guide Compilation by EmeraldchowMirzaNo ratings yet
- Chapter 2 Ag - EconDocument7 pagesChapter 2 Ag - EconJay Kenneth Bajar Cernal100% (1)
- INS2015 Fundamentals of Finance HungCV 1Document3 pagesINS2015 Fundamentals of Finance HungCV 1Phương Anh NguyễnNo ratings yet
- One Wavelength To Loop SkywireDocument2 pagesOne Wavelength To Loop SkywireRobert TurnerNo ratings yet
- Mecanica MD - AZG-UDocument29 pagesMecanica MD - AZG-UStefanoViganóNo ratings yet
- Solution PDFDocument20 pagesSolution PDFVard FarrellNo ratings yet
- MiningDocument3 pagesMiningDherick RaleighNo ratings yet
- Sect. 4 Tech Docum PC7 AutoLube - 1209 PDFDocument46 pagesSect. 4 Tech Docum PC7 AutoLube - 1209 PDFAlexis MikeNo ratings yet
- Inglês - Degrees of ComparisonDocument4 pagesInglês - Degrees of ComparisonVersehgi IINo ratings yet
- Module 1 Inclusive Education Lecture 1 & Introduction - OnlineDocument32 pagesModule 1 Inclusive Education Lecture 1 & Introduction - OnlineSharon ShenNo ratings yet
- NC Error PropagationDocument12 pagesNC Error PropagationSalman KhanNo ratings yet
- Anaximenes of MiletusDocument4 pagesAnaximenes of MiletusRosel Gonzalo-AquinoNo ratings yet
- Ideal Vs Real OttoDocument5 pagesIdeal Vs Real Ottoa7med SoulimanNo ratings yet
- Hemo TecaDocument17 pagesHemo TecaMafer PilcoNo ratings yet
- Hamming Code - Error Detection Aim: AlgorithmDocument12 pagesHamming Code - Error Detection Aim: Algorithmkrithikgokul selvamNo ratings yet
- Interjections NotesDocument2 pagesInterjections NotesKanna ImuiNo ratings yet