You might also like
- The Anaerobic Threshold 50 Years of ControversyDocument31 pagesThe Anaerobic Threshold 50 Years of ControversyHansCristopherSaegerPizarroNo ratings yet
- A2 The Energy ContinuumDocument4 pagesA2 The Energy ContinuumMike Stallard0% (1)
- Clinical Nutrition: E. Wesselink, W.A.C. Koekkoek, S. Grefte, R.F. Witkamp, A.R.H. Van ZantenDocument14 pagesClinical Nutrition: E. Wesselink, W.A.C. Koekkoek, S. Grefte, R.F. Witkamp, A.R.H. Van ZantenabhijitNo ratings yet
- GI History IntroductoryDocument74 pagesGI History IntroductoryNur Hamizah Md FuziNo ratings yet
- Striver SDE Sheet (Core) Most Asked Interview QuestionsDocument40 pagesStriver SDE Sheet (Core) Most Asked Interview QuestionsDebasish Senapaty100% (1)
- Current Understanding of ItsDocument9 pagesCurrent Understanding of Itsnovia mentariNo ratings yet
- Mitochondrial Transfer and Regulators of Mesenchymal Stromal Cell Function and Therapeutic EfficacDocument22 pagesMitochondrial Transfer and Regulators of Mesenchymal Stromal Cell Function and Therapeutic EfficacEmiNo ratings yet
- Carb metabolism regulationDocument9 pagesCarb metabolism regulationHammad KambohNo ratings yet
- COVID-19: Hemoglobin, Iron, and Hypoxia Beyond Inflammation. A Narrative ReviewDocument7 pagesCOVID-19: Hemoglobin, Iron, and Hypoxia Beyond Inflammation. A Narrative ReviewAlejandroNo ratings yet
- Curries, Chutneys and Imperial Britain: Rohit Varman, "Curry," Consumption Markets and Culture (May 24, 2016), 5Document9 pagesCurries, Chutneys and Imperial Britain: Rohit Varman, "Curry," Consumption Markets and Culture (May 24, 2016), 5asdfhjjkNo ratings yet
- Glycogen Storage DiseasesDocument5 pagesGlycogen Storage DiseasessanflashNo ratings yet
- CIRRHOSIS Dr. VishvasDocument49 pagesCIRRHOSIS Dr. VishvasvishvasNo ratings yet
- Aging Cell - 2021 - Ogrodnik - Whole Body Senescent Cell Clearance Alleviates Age Related Brain Inflammation and CognitiveDocument16 pagesAging Cell - 2021 - Ogrodnik - Whole Body Senescent Cell Clearance Alleviates Age Related Brain Inflammation and CognitiveMediatheek SGANo ratings yet
- Clinical Application of EnzymesDocument6 pagesClinical Application of EnzymesTemesgen MucheyeNo ratings yet
- Delayed Ejaculation & Anorgasmia: Emmanuele A. JanniniDocument52 pagesDelayed Ejaculation & Anorgasmia: Emmanuele A. JanniniMahmoud Zedan100% (1)
- Dynamic Model of CHO Cell Metabolism PDFDocument17 pagesDynamic Model of CHO Cell Metabolism PDFIdalba SouzaNo ratings yet
- Sarcopenia, Frailty and Type 2 Diabetes Mellitus (Mol Med Rep 2021)Document9 pagesSarcopenia, Frailty and Type 2 Diabetes Mellitus (Mol Med Rep 2021)鍾斯凱No ratings yet
- Carbohydrate MetabolismDocument53 pagesCarbohydrate Metabolismjehram navalesNo ratings yet
- BIOLS 300 Lab 3 - Thin Layer Chromatography PowerpointDocument38 pagesBIOLS 300 Lab 3 - Thin Layer Chromatography PowerpointmariamNo ratings yet
- Supportive, Palliative Care & Survivorship in Prostate Cancer ICI April 2022 ZADocument39 pagesSupportive, Palliative Care & Survivorship in Prostate Cancer ICI April 2022 ZAMichaelNo ratings yet
- Sequence 02 Summary 4ms 2021 - 2022Document1 pageSequence 02 Summary 4ms 2021 - 2022FerielAdj100% (1)
- Photosynthesis in higher plants: The key process of lifeDocument14 pagesPhotosynthesis in higher plants: The key process of lifeShruti KumariNo ratings yet
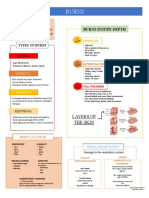
- BurnsDocument3 pagesBurnsCerezo, Cherrieus Ann C.No ratings yet
- Ly Mitochondrial DiseaseDocument9 pagesLy Mitochondrial DiseaseLe Phuong LyNo ratings yet
- NarcolepsyDocument8 pagesNarcolepsymaraNo ratings yet
- Practical training agreementDocument4 pagesPractical training agreementNace Atanasov100% (1)
- Beverage Analysis in Forensic and Liquor SamplesDocument6 pagesBeverage Analysis in Forensic and Liquor SamplesSachin ashokNo ratings yet
- Proteins: Structure, Functions and Recent UpdatesDocument59 pagesProteins: Structure, Functions and Recent UpdatesIvan Jhon AnamNo ratings yet
- Andropause Current ConceptsDocument9 pagesAndropause Current ConceptsHAVIZ YUADNo ratings yet
- Enzyme 1 PDFDocument96 pagesEnzyme 1 PDFBarack BLNo ratings yet
- Irritable Bowel Syndrome PTH 617 PresentationDocument14 pagesIrritable Bowel Syndrome PTH 617 Presentationapi-621438645No ratings yet
- InhalationalDocument87 pagesInhalationalsourabh jakharNo ratings yet
- Role of A Novel Transdermal Patch For Both Antihypertensive and Antiparkinsonism ActivityDocument8 pagesRole of A Novel Transdermal Patch For Both Antihypertensive and Antiparkinsonism ActivityMr.S. p.royNo ratings yet
- LRTIDocument13 pagesLRTIRomina Mae FajardoNo ratings yet
- Chapter 23 Metabolism and Energy ProductionDocument68 pagesChapter 23 Metabolism and Energy ProductionZahid HussainNo ratings yet
- The Renin Angiotensin Aldosterone System - RAASDocument3 pagesThe Renin Angiotensin Aldosterone System - RAASrienz nicnic peraltaNo ratings yet
- Glucocorticoids and Mineralocorticoids: Roles and EffectsDocument27 pagesGlucocorticoids and Mineralocorticoids: Roles and EffectsAmrit GaireNo ratings yet
- A Review of Liposomes As A Drug Delivery System CurrentDocument23 pagesA Review of Liposomes As A Drug Delivery System CurrentRayo Hernandez100% (1)
- Corometrics 250cx User and Operating ManualDocument194 pagesCorometrics 250cx User and Operating ManualRonnelSerranoNo ratings yet
- The Role of ATP as the Energy Currency in Living CellsDocument63 pagesThe Role of ATP as the Energy Currency in Living CellsRizky FebriantiNo ratings yet
- Red Hat Enterprise Linux-7-DM Multipath-en-USDocument63 pagesRed Hat Enterprise Linux-7-DM Multipath-en-USMuhammad Windiarto HermawanNo ratings yet
- Perioperative Acide-Base Balance - Ahmad DamlajDocument26 pagesPerioperative Acide-Base Balance - Ahmad DamlajpaulaNo ratings yet
- Clinical Therapeutics Hazel Mae B. ValdezDocument29 pagesClinical Therapeutics Hazel Mae B. ValdezMichelle Vera GabunNo ratings yet
- Acidosis & AlkalosisDocument29 pagesAcidosis & Alkalosiszaeem1993No ratings yet
- 12 Bicarbonate, Calcium, Phosphate and MagnesiumDocument38 pages12 Bicarbonate, Calcium, Phosphate and MagnesiumFrances FranciscoNo ratings yet
- ABG Interpretation GuideDocument32 pagesABG Interpretation GuidePervinNo ratings yet
- Acid-Base BalanceDocument7 pagesAcid-Base BalanceMichelle Mae JulianaNo ratings yet
- Chloremia (Hypochloremia) & Acute and Chronic Respiratory Alkalosis (Carbonic Acid Deficit)Document4 pagesChloremia (Hypochloremia) & Acute and Chronic Respiratory Alkalosis (Carbonic Acid Deficit)KQarlo Luis Pestaño Maniaol100% (1)
- Acid Base BalanceDocument45 pagesAcid Base BalanceSameer Ul BashirNo ratings yet
- ACID BASE BALANCE and disordersDocument47 pagesACID BASE BALANCE and disordersShivanand MaliNo ratings yet
- Acid-base and hydromineral balance regulationDocument55 pagesAcid-base and hydromineral balance regulationVio MincuNo ratings yet
- Midterm Notes by F.L.F.Sanjuan, RMT, DtaDocument3 pagesMidterm Notes by F.L.F.Sanjuan, RMT, DtaIbtisam YusufNo ratings yet
- Tissue PerfusionDocument70 pagesTissue PerfusionAlexNo ratings yet
- Acid-Base Balance PDFDocument10 pagesAcid-Base Balance PDFinah krizia lagueNo ratings yet
- Renal Tubular Acidosis Types and DiagnosisDocument71 pagesRenal Tubular Acidosis Types and DiagnosisariNo ratings yet
- Acid-Base Disorders NotesDocument10 pagesAcid-Base Disorders NotesLovely100% (1)
- Renal Tubular Acidosis Diagnosis and TypesDocument59 pagesRenal Tubular Acidosis Diagnosis and Typeskash_buNo ratings yet
- Metabolic AlkalosisDocument54 pagesMetabolic AlkalosispriyankagalhotraNo ratings yet
- Chapter 2 Electrolytes and Body Fluid AnalysiDocument103 pagesChapter 2 Electrolytes and Body Fluid AnalysiSanyii MamuyeNo ratings yet
- Metabolic AlkalosisDocument8 pagesMetabolic AlkalosisPauline PerezNo ratings yet
- Hema Quiz RatioDocument20 pagesHema Quiz RatioElla OrtegaNo ratings yet
- Quizzes RationaleDocument22 pagesQuizzes RationaleElla OrtegaNo ratings yet
- Histo QuizDocument1 pageHisto QuizElla OrtegaNo ratings yet
- Microscopic Analysis of Urine SedimentsDocument21 pagesMicroscopic Analysis of Urine SedimentsElla OrtegaNo ratings yet
- Errors and The CBC Result 2.0Document43 pagesErrors and The CBC Result 2.0Ella OrtegaNo ratings yet
- Chloride, Bicarbonate and LactateDocument25 pagesChloride, Bicarbonate and LactateElla OrtegaNo ratings yet
- Antihuman Globulin TestsDocument6 pagesAntihuman Globulin TestsElla OrtegaNo ratings yet
- 2.2 - Weak D AntigenDocument3 pages2.2 - Weak D AntigenElla OrtegaNo ratings yet
- Parathyroid Gland Anatomy and FunctionDocument3 pagesParathyroid Gland Anatomy and FunctionElla OrtegaNo ratings yet
- St. John, Isaac Newton and Prediction of MedicanesDocument6 pagesSt. John, Isaac Newton and Prediction of MedicanesMarthaNo ratings yet
- Brand Awareness Impact Repeat PurchaseDocument10 pagesBrand Awareness Impact Repeat Purchasegaurish raoNo ratings yet
- Massey University: Te Kunenga Ki PürehuroaDocument29 pagesMassey University: Te Kunenga Ki PürehuroaMartin GohNo ratings yet
- DISGRACED Teacher S Pack.1 PDFDocument33 pagesDISGRACED Teacher S Pack.1 PDFSaad Imran δδNo ratings yet
- PERSONALITY DEVELOPMENT COURSE MODULEDocument9 pagesPERSONALITY DEVELOPMENT COURSE MODULELeniel John DionoraNo ratings yet
- Common Neonatal Dermatological ConditionsDocument27 pagesCommon Neonatal Dermatological ConditionsArslan SiddiquiNo ratings yet
- Science 5 Quiz Bee ReviewerDocument7 pagesScience 5 Quiz Bee ReviewerRommel Urbano Yabis50% (2)
- Spectral Correlation of OFDM SignalsDocument6 pagesSpectral Correlation of OFDM Signalsazebshaikh3927No ratings yet
- Contemporary ArtDocument2 pagesContemporary ArtXpertz PrintingNo ratings yet
- Green Building ToolsDocument107 pagesGreen Building ToolsVholts Villa VitugNo ratings yet
- Jopillo Vs PeopleDocument1 pageJopillo Vs PeopleivybpazNo ratings yet
- Impala Job Application 2Document3 pagesImpala Job Application 2EXXARO MATLANo ratings yet
- IMC PlanDocument6 pagesIMC PlanRizwan Ahmed KhanNo ratings yet
- Test Practice 1Document5 pagesTest Practice 1syafwanNo ratings yet
- 3 Week Lit 121Document48 pages3 Week Lit 121Cassandra Dianne Ferolino MacadoNo ratings yet
- UNIT 1 - Revision: HFFFFFDocument3 pagesUNIT 1 - Revision: HFFFFFRedDinoandbluebird ChannelTMNo ratings yet
- Article 405: The Penal-Code With AmendmentsDocument2 pagesArticle 405: The Penal-Code With Amendmentsropal salamNo ratings yet
- Experiential Marketing How To Get Customers To Sense, Feel, Think, Act, RelateDocument6 pagesExperiential Marketing How To Get Customers To Sense, Feel, Think, Act, RelateBhaumik NayakNo ratings yet
- Reaction Paper XDocument2 pagesReaction Paper XRichmond Amurao95% (22)
- Just Say NO To Baby EinsteinDocument5 pagesJust Say NO To Baby Einsteinsmartypinto0% (1)
- Free-Range Chicken Farming PDFDocument138 pagesFree-Range Chicken Farming PDFDennis MacedoNo ratings yet
- Grade 10 Sasmo: secθ + tanθ = q, secθ q. q q q qDocument3 pagesGrade 10 Sasmo: secθ + tanθ = q, secθ q. q q q qAje GhazaNo ratings yet
- Archaeology - The Telltale ArtDocument15 pagesArchaeology - The Telltale ArtShubha PujariNo ratings yet
- English - Exam ECO - 2Document6 pagesEnglish - Exam ECO - 2yogie yohansyahNo ratings yet
- Fire Safety Al RaiDocument4 pagesFire Safety Al RairyecunarNo ratings yet
- Islamic Bank ArbitrationDocument27 pagesIslamic Bank Arbitrationapi-3711136No ratings yet
- Assessing ViolenceDocument6 pagesAssessing ViolenceKarlo Jose Dao-ayanNo ratings yet
- 3rd Party AffidavitDocument4 pages3rd Party Affidavitarafat ahmedNo ratings yet
- Hybrid - 01Document209 pagesHybrid - 01Santos ArwinNo ratings yet
- MGT162Document23 pagesMGT162ZulaiqhaAisya50% (2)