You might also like
- 5 Choices Mini BookDocument119 pages5 Choices Mini BookChristos Angnsts100% (1)
- Learn Spanish Like Crazy e BookDocument14 pagesLearn Spanish Like Crazy e Bookfrankovski100% (1)
- Gillberg 2007 Adult DISCO LongitudinalDocument9 pagesGillberg 2007 Adult DISCO LongitudinalSkymaker69No ratings yet
- Central Coherence in Adults With A High-Functioning Autism Spectrum Disorder. in A Search For A Non-Self-Reporting Screening ToolDocument8 pagesCentral Coherence in Adults With A High-Functioning Autism Spectrum Disorder. in A Search For A Non-Self-Reporting Screening ToolNp Luis Gómez0% (1)
- Ncbi - Nlm.nih - Gov-Autism Spectrum Disorder The Impact of Stressful and Traumatic Life Events and Implications For CliniDocument13 pagesNcbi - Nlm.nih - Gov-Autism Spectrum Disorder The Impact of Stressful and Traumatic Life Events and Implications For CliniJinny DavisNo ratings yet
- Autism Spectrum Disorder: Outcomes in Adulthood: ReviewDocument8 pagesAutism Spectrum Disorder: Outcomes in Adulthood: ReviewRosa Indah KusumawardaniNo ratings yet
- Coocurrencias y Edad en El Diagnóstioco de AutismoDocument14 pagesCoocurrencias y Edad en El Diagnóstioco de Autismopsi.danae.hardingNo ratings yet
- Autism in Adolescents and Adults MesibovDocument23 pagesAutism in Adolescents and Adults MesibovSmurfing is FunNo ratings yet
- Autism gender differences in clinical managementDocument6 pagesAutism gender differences in clinical managementElian Y. Sanchez-RiveraNo ratings yet
- The Relationship Between Carers Report oDocument8 pagesThe Relationship Between Carers Report oGustavo Godoy GarceteNo ratings yet
- Describing The Profile of Diagnostic Features in ADocument12 pagesDescribing The Profile of Diagnostic Features in AvcuadrosvNo ratings yet
- ASD Characteristics Common in Older Adults with DepressionDocument9 pagesASD Characteristics Common in Older Adults with DepressionKharisma FatwasariNo ratings yet
- Lever Geurts2016 Article PsychiatricCo OccurringSymptomDocument15 pagesLever Geurts2016 Article PsychiatricCo OccurringSymptommarc-iglesias-gonzalez-9667No ratings yet
- Visual attention to social and non-social objects across the autism spectrumFrom EverandVisual attention to social and non-social objects across the autism spectrumNo ratings yet
- CBCL Profiles of Children and Adolescents With Asperger Syndrome - A Review and Pilot StudyDocument12 pagesCBCL Profiles of Children and Adolescents With Asperger Syndrome - A Review and Pilot StudyWildan AnrianNo ratings yet
- Cognitive Functioning in Adolescents With SelfReported ADHD and Depression Results From A Population-Based StudyDocument14 pagesCognitive Functioning in Adolescents With SelfReported ADHD and Depression Results From A Population-Based StudyJesúsCoyacNo ratings yet
- A-Hudson, Hall & Harkness (2019)Document11 pagesA-Hudson, Hall & Harkness (2019)Jordanitha BhsNo ratings yet
- Anxiety and Depression in Adults With AutismDocument14 pagesAnxiety and Depression in Adults With AutismNyah RodriguesNo ratings yet
- Comorbid Mental Disorders in Children and Adolescents With Attention-Deficit:hyperactivity Disorder in A Large Nationwide StudyDocument12 pagesComorbid Mental Disorders in Children and Adolescents With Attention-Deficit:hyperactivity Disorder in A Large Nationwide StudyMarina HeinenNo ratings yet
- 10.1007@s10803 020 04450 2Document9 pages10.1007@s10803 020 04450 2generjustnNo ratings yet
- Co Morbidity in Asperger Syndrome: A Review of The LiteratureDocument20 pagesCo Morbidity in Asperger Syndrome: A Review of The LiteratureLorenaGeorgianaNo ratings yet
- Adults With Autism Spectrum Disorders OutcomesDocument9 pagesAdults With Autism Spectrum Disorders OutcomesAnaLaura JulcahuancaNo ratings yet
- Braithwaite - 2020 - Chapter 13 - Social Attentionchapter 13 - Social AttentionDocument33 pagesBraithwaite - 2020 - Chapter 13 - Social Attentionchapter 13 - Social AttentionRobert WardNo ratings yet
- CATQ ShortReport FINAL 02 05 21 PREPRINTDocument17 pagesCATQ ShortReport FINAL 02 05 21 PREPRINTJennifer Soares de Souza de FreitasNo ratings yet
- Sappok AJIID 2015Document15 pagesSappok AJIID 2015Jose Alonso Aguilar ValeraNo ratings yet
- Fuld2018 Article AutismSpectrumDisorderTheImpacDocument8 pagesFuld2018 Article AutismSpectrumDisorderTheImpacDanya KatsNo ratings yet
- Antisocial Article2Document11 pagesAntisocial Article2mimirozmiza7No ratings yet
- Sizoo 2009Document7 pagesSizoo 2009amarillonoexpectaNo ratings yet
- Asd Comorbid With Odd ResearchDocument10 pagesAsd Comorbid With Odd ResearchAnila OmerNo ratings yet
- CHAPTER 02, Literature ReviewDocument27 pagesCHAPTER 02, Literature ReviewAyesha ArshedNo ratings yet
- Medical Aspects of Autism Spectrum DisorderDocument12 pagesMedical Aspects of Autism Spectrum DisorderTimquannaNo ratings yet
- 1-s2.0-S027273582400031X-mainDocument12 pages1-s2.0-S027273582400031X-mainRubén Sánchez PeruchaNo ratings yet
- AutismoDocument8 pagesAutismoSol ContrerasNo ratings yet
- (Paperhub - Ir) 10.1016 J.ridd.2013.01.028Document14 pages(Paperhub - Ir) 10.1016 J.ridd.2013.01.028alejandraNo ratings yet
- PDD-NOS Diagnostic ChallengesDocument16 pagesPDD-NOS Diagnostic ChallengesTracey RompasNo ratings yet
- Differential Diagnosis and Comorbidity Distinguishing Autism From Other Mental Health Issues NeuropsychiatryDocument11 pagesDifferential Diagnosis and Comorbidity Distinguishing Autism From Other Mental Health Issues NeuropsychiatryJohn Bowen BrownNo ratings yet
- Co-Occurring Psychiatric Conditions in Autism Spectrum DisordersDocument23 pagesCo-Occurring Psychiatric Conditions in Autism Spectrum DisordersPAULANo ratings yet
- Chips Padres EscalassDocument10 pagesChips Padres EscalassB10. Oscar Alonso Díaz PintoNo ratings yet
- Craig2014 PDFDocument10 pagesCraig2014 PDFCristinaNo ratings yet
- Final Thesis in ProcessDocument61 pagesFinal Thesis in ProcessAyesha ArshedNo ratings yet
- Research PaperDocument6 pagesResearch PaperTham DangNo ratings yet
- Autism Research - 2021 - Vivanti - The Prevalence and Incidence of Early Onset Dementia Among Adults With Autism SpectrumDocument11 pagesAutism Research - 2021 - Vivanti - The Prevalence and Incidence of Early Onset Dementia Among Adults With Autism SpectrumLuas PelegriniNo ratings yet
- Adhd MakaleDocument11 pagesAdhd MakaleNESLİHAN ORALNo ratings yet
- ADHD & ASD in Adult Psych PatientsDocument102 pagesADHD & ASD in Adult Psych PatientsexpositrixNo ratings yet
- DownDocument43 pagesDownAndrea LópezNo ratings yet
- Prevalence of ADD-ADHD in Older AdultsDocument8 pagesPrevalence of ADD-ADHD in Older AdultsRyan BNo ratings yet
- Autism 3Document12 pagesAutism 3marwaawad729No ratings yet
- Self-Diagnosis of Autism ExploredDocument28 pagesSelf-Diagnosis of Autism ExploredAbominaciónNo ratings yet
- The Presence of Behavioural and Psychological Symptoms and Progression To Dementia in The Cognitively Impaired Older PopulationDocument11 pagesThe Presence of Behavioural and Psychological Symptoms and Progression To Dementia in The Cognitively Impaired Older PopulationCeci_SunshineNo ratings yet
- Autism Assessment 1Document11 pagesAutism Assessment 1pammiefisherNo ratings yet
- Anxiety and Depression. Autism in AdultsDocument14 pagesAnxiety and Depression. Autism in AdultsEdl ZsuzsiNo ratings yet
- Childhood Epilepsy and Autism Spectrum Disorders: Psychiatric Problems and AnticonvulsantsDocument9 pagesChildhood Epilepsy and Autism Spectrum Disorders: Psychiatric Problems and AnticonvulsantsTheo KhouryNo ratings yet
- Essay 2 Draft 2Document6 pagesEssay 2 Draft 2api-665989338No ratings yet
- Id AutismDocument16 pagesId AutismKusmarwaty DrahmaNo ratings yet
- The Childhood Autism Spectrum Test (CAST) :spanish Adaptation and ValidationDocument8 pagesThe Childhood Autism Spectrum Test (CAST) :spanish Adaptation and ValidationJose Alonso Aguilar ValeraNo ratings yet
- Adult PsychiatricDocument21 pagesAdult PsychiatricAndré SilvaNo ratings yet
- A Literature Analysis On The Quality of Life in Adults With AutismDocument11 pagesA Literature Analysis On The Quality of Life in Adults With AutismPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Research Final Paper-Brenna SchulteDocument15 pagesResearch Final Paper-Brenna Schulteapi-610116630No ratings yet
- Ijmrhs 21 41642Document4 pagesIjmrhs 21 41642emiliodiazneuropsicologoNo ratings yet
- What Is The Association Between ADI R Scores and Final Diagnosis of Autism in An All IQ Adult Autism Diagnostic ServiceDocument20 pagesWhat Is The Association Between ADI R Scores and Final Diagnosis of Autism in An All IQ Adult Autism Diagnostic Serviceaspire centerNo ratings yet
- Tsakanikos, Et Al. 2005 Psychopathology in Adults With Autism and Intellectual Disability. Journal On-Lineunpaginated in PressDocument12 pagesTsakanikos, Et Al. 2005 Psychopathology in Adults With Autism and Intellectual Disability. Journal On-Lineunpaginated in PressClaudia AndreeaNo ratings yet
- Jurnal AutismeDocument11 pagesJurnal AutismeKabhithra ThiayagarajanNo ratings yet
- ONions2018 Article HowDoParentsManageIrritabilityDocument15 pagesONions2018 Article HowDoParentsManageIrritabilityLD Kabinet Dnevni BoravakNo ratings yet
- Why Fold Asperger Syndrome Into Autism Spectrum Disorder in The DSM 5Document6 pagesWhy Fold Asperger Syndrome Into Autism Spectrum Disorder in The DSM 5LD Kabinet Dnevni BoravakNo ratings yet
- Reclassification of Rett Syndrome Diagnosis Stirs ConcernsDocument5 pagesReclassification of Rett Syndrome Diagnosis Stirs ConcernsLD Kabinet Dnevni BoravakNo ratings yet
- 10 1111@jcpp 13176Document15 pages10 1111@jcpp 13176LD Kabinet Dnevni BoravakNo ratings yet
- Curriculum Design Principles for Effective Teaching and LearningDocument5 pagesCurriculum Design Principles for Effective Teaching and LearningPatrick kenneth GacayanNo ratings yet
- Group Project Part 2 - Own Group AssessmentDocument1 pageGroup Project Part 2 - Own Group AssessmentDeveshwar BansalNo ratings yet
- Panduan Verifikasi InacbgDocument8 pagesPanduan Verifikasi InacbgDhoni SuhendraNo ratings yet
- Paranthropology Vol 2 No 3Document64 pagesParanthropology Vol 2 No 3Jack Hunter100% (1)
- Research ProposalDocument5 pagesResearch ProposalLueween Acay CansinoNo ratings yet
- Lesson PlanDocument2 pagesLesson PlanAmin MofrehNo ratings yet
- Spring 2015 - 100 Syllabus (Section 2 & 4)Document4 pagesSpring 2015 - 100 Syllabus (Section 2 & 4)hujie19930721No ratings yet
- REPORTDocument15 pagesREPORTAasheenNo ratings yet
- BSD Outside Learning Permission FormDocument2 pagesBSD Outside Learning Permission FormihappyscribdNo ratings yet
- Find Someone Who Social MediaDocument2 pagesFind Someone Who Social MediaandresNo ratings yet
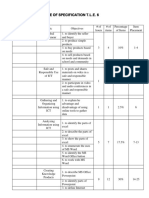
- Table of Specification T.L.E. 6Document3 pagesTable of Specification T.L.E. 6Autumn Thorn SebastianNo ratings yet
- Murray's Psychological Needs TheoryDocument4 pagesMurray's Psychological Needs TheoryLouriel NopalNo ratings yet
- Mcelroy Knowledge Management CycleDocument18 pagesMcelroy Knowledge Management CycleshahidNo ratings yet
- Verbal Advantage Powerful 3500 Vocabulary Words Yasser PDFDocument763 pagesVerbal Advantage Powerful 3500 Vocabulary Words Yasser PDFDharm D Veer Sorout67% (3)
- Friend, hobby, holiday memoriesDocument4 pagesFriend, hobby, holiday memoriesHiếu Nguyễn Minh100% (2)
- Management Accounting ResearchDocument3 pagesManagement Accounting Researchali asgharNo ratings yet
- Intuition and Problem Solving: Jo M.C. NelissenDocument18 pagesIntuition and Problem Solving: Jo M.C. NelissenAnonymous wx5GrtgxpXNo ratings yet
- BEd Case Study and Life Skills Project 2013 14Document4 pagesBEd Case Study and Life Skills Project 2013 14Chandra Reddy0% (2)
- Effects of Internet AddictionDocument14 pagesEffects of Internet AddictionHeraHeccateNo ratings yet
- Human Behavior in Organization 2022Document14 pagesHuman Behavior in Organization 2022bibaljennymae487No ratings yet
- Cbse Class 12 Marking Scheme 2017 18 PaintingDocument4 pagesCbse Class 12 Marking Scheme 2017 18 PaintingMayank KatiyarNo ratings yet
- Vampire The Requiem - SAS - Scenes of FrenzyDocument16 pagesVampire The Requiem - SAS - Scenes of FrenzyCaio César100% (1)
- Bonding and NurturingDocument14 pagesBonding and Nurturingapi-325621104No ratings yet
- Henry, G. K. G. - The Characters of Terence (Art, 1915)Document44 pagesHenry, G. K. G. - The Characters of Terence (Art, 1915)Verónica Díaz PereyroNo ratings yet
- What S in A Name Exploring Pansexuality OnlineDocument16 pagesWhat S in A Name Exploring Pansexuality OnlineBrendaNo ratings yet
- Infidelity in RelationshipsDocument3 pagesInfidelity in RelationshipsYadira Estrada GuevaraNo ratings yet
- SP Vocabulary Activity 1 List 2Document19 pagesSP Vocabulary Activity 1 List 2api-632674858No ratings yet
- Poems Questions N AnswersDocument18 pagesPoems Questions N AnswersAtiqahrafeeNo ratings yet