You might also like
- Avances en LESDocument8 pagesAvances en LESFranciscoJoseNo ratings yet
- Gran Neg MDR, IDSADocument17 pagesGran Neg MDR, IDSAFranciscoJoseNo ratings yet
- Hipotension OrtostaticaDocument10 pagesHipotension OrtostaticaFranciscoJoseNo ratings yet
- Hypertension in Pregnancy: Diagnosis, Blood Pressure Goals, and Pharmacotherapy: A Scientific Statement From The American Heart AssociationDocument21 pagesHypertension in Pregnancy: Diagnosis, Blood Pressure Goals, and Pharmacotherapy: A Scientific Statement From The American Heart AssociationElias Emmanuel JaimeNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Denawaka GangaDocument9 pagesDenawaka GangaErandikaNo ratings yet
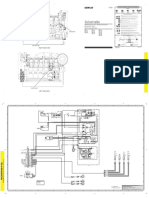
- Plano Grupo ElectrogenoDocument2 pagesPlano Grupo Electrogenoluis alberto rodriguezNo ratings yet
- ZavzpretDocument21 pagesZavzpretNeethu Anna StephenNo ratings yet
- VBAC Parents Guide v2 April 2019Document110 pagesVBAC Parents Guide v2 April 2019The VBAC Link100% (4)
- Warm Vs Cold ShockDocument8 pagesWarm Vs Cold ShockmarleeramirezNo ratings yet
- Engineering ManualDocument27 pagesEngineering ManualThousif Rahman67% (3)
- 3 - 2017 - Superia X 5 StarDocument26 pages3 - 2017 - Superia X 5 Starsomnath serviceNo ratings yet
- Technical Data Book: RAC For SEDA (INV, R410A, 60Hz, C/O)Document43 pagesTechnical Data Book: RAC For SEDA (INV, R410A, 60Hz, C/O)joserosineiassisdasilvaNo ratings yet
- Dissertation - December 2022Document71 pagesDissertation - December 2022Musasa TinasheNo ratings yet
- 2 Way 3 Way Piping DiagramDocument1 page2 Way 3 Way Piping DiagrammarrukhjNo ratings yet
- Honey & Bee Product Recipes: November 2007Document29 pagesHoney & Bee Product Recipes: November 2007Kyra ThomasNo ratings yet
- Finasteride 5mg PDFDocument18 pagesFinasteride 5mg PDFddandan_2No ratings yet
- Ibsen in PracticeDocument17 pagesIbsen in PracticevictorkalkaNo ratings yet
- ECSS Q ST 70 02C (15november2008)Document45 pagesECSS Q ST 70 02C (15november2008)jsadachiNo ratings yet
- NeseritideDocument28 pagesNeseritideNavojit Chowdhury100% (1)
- Edc Power Plant FacilitiesDocument32 pagesEdc Power Plant FacilitiesMichael TayactacNo ratings yet
- "Fish" From Gourmet RhapsodyDocument4 pages"Fish" From Gourmet RhapsodySean MattioNo ratings yet
- Piriformis MuscleDocument3 pagesPiriformis MuscleBen CampbellNo ratings yet
- Neonatal Ventilation, Step by StepDocument99 pagesNeonatal Ventilation, Step by StepMarely Ovando Castillo93% (14)
- Moisture Sorption Isotherms Characteristics of Food ProductsDocument10 pagesMoisture Sorption Isotherms Characteristics of Food ProductsMustapha Bello50% (2)
- India TodayDocument76 pagesIndia TodaySanket RaveendraNo ratings yet
- Product Brochure-Electronically Controlled Air Dryer-ECA PDFDocument4 pagesProduct Brochure-Electronically Controlled Air Dryer-ECA PDFAnonymous O0T8aZZNo ratings yet
- SpaceX ProposalDocument6 pagesSpaceX ProposalTexas WatchdogNo ratings yet
- 4 ReactorsDocument58 pages4 ReactorsKiran ShresthaNo ratings yet
- Fire Prevention and Response Plan for Greenergie PlantDocument8 pagesFire Prevention and Response Plan for Greenergie PlantMelba MangabatNo ratings yet
- Ben'S Muffler RepairDocument9 pagesBen'S Muffler RepairDana LantoNo ratings yet
- Tugas UNtar 3Document28 pagesTugas UNtar 3Daniel Filemon PosoNo ratings yet
- CS Risk and Crisis Management FinalDocument62 pagesCS Risk and Crisis Management FinaldangermanNo ratings yet
- Inr Si47 1038g e PDFDocument107 pagesInr Si47 1038g e PDFsd23No ratings yet