You might also like
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- Bantuan Hidup Dasar Dan Lanjut: BHD-BHLDocument38 pagesBantuan Hidup Dasar Dan Lanjut: BHD-BHLIda Benecia DeseNo ratings yet
- Oxygen Therapy BasicsDocument14 pagesOxygen Therapy BasicsCabdiNo ratings yet
- Oxygen TherapyDocument33 pagesOxygen Therapyالغائب الحاضرNo ratings yet
- Oxygen Delivery Systems: Muhimbili National Hospital Critical Care OrientationDocument15 pagesOxygen Delivery Systems: Muhimbili National Hospital Critical Care OrientationfadhiliNo ratings yet
- Oxygen Therapy: Adel Alrihili BSN-RNDocument36 pagesOxygen Therapy: Adel Alrihili BSN-RNmacmohitNo ratings yet
- Terapi Oksigen Dan Tata Laksana Jalan NapasDocument20 pagesTerapi Oksigen Dan Tata Laksana Jalan NapaspiniNo ratings yet
- Terapi Oxygen Pada Pasien Covd-19Document24 pagesTerapi Oxygen Pada Pasien Covd-19normamNo ratings yet
- Ncma113-Finals Modules SummariesDocument3 pagesNcma113-Finals Modules Summariesroldanmarygrace023No ratings yet
- Terapi Oksigen Dan Tata Laksana Jalan NapasDocument23 pagesTerapi Oksigen Dan Tata Laksana Jalan NapasThivyaroobiniNo ratings yet
- Oxygen TherapyDocument2 pagesOxygen TherapyPhilip MusonyeNo ratings yet
- 7-Hypoxia Is A KillerDocument33 pages7-Hypoxia Is A KillerChamindraNo ratings yet
- Oxygen TherapyDocument41 pagesOxygen TherapyYOGAKRISHNANNo ratings yet
- Oxygen Therapy Principles and PracticeDocument34 pagesOxygen Therapy Principles and PracticeMark Anthony AlcantaraNo ratings yet
- DR Lodha Oxygen Therapy in Covid-19 PedsDocument30 pagesDR Lodha Oxygen Therapy in Covid-19 PedsBhoomika PandeyNo ratings yet
- DIXION Practice Anesthesia WorkstationsDocument7 pagesDIXION Practice Anesthesia WorkstationsDharma PoudelNo ratings yet
- Oxygen TherapyDocument59 pagesOxygen TherapyRosi AmaliaNo ratings yet
- Oxygen TherapyDocument33 pagesOxygen TherapySaudah IbrahimNo ratings yet
- Principles of oxygen therapy in the newbornDocument52 pagesPrinciples of oxygen therapy in the newbornKhirzaNo ratings yet
- Мэдээгүйжүүлэх аппаратDocument2 pagesМэдээгүйжүүлэх аппаратЖавхланбаяр ЖаргалсайханNo ratings yet
- Ncma113 Lec & Lab From Dash 10 - Summer Final 2021: Oxygen TherapyDocument12 pagesNcma113 Lec & Lab From Dash 10 - Summer Final 2021: Oxygen TherapyAliyah Julianne PayumoNo ratings yet
- Easy Oxygen TherapyDocument13 pagesEasy Oxygen TherapyKrizamay Ongat AggerNo ratings yet
- L04 - Part LL Updated Oxygen TherapyDocument12 pagesL04 - Part LL Updated Oxygen TherapyTariku GebreNo ratings yet
- Oxygen Therapy CPG GuideDocument4 pagesOxygen Therapy CPG Guidedragon66No ratings yet
- Spek Vent Vela ComphDocument4 pagesSpek Vent Vela ComphRinawatiNo ratings yet
- Oxygen Delivery Devices: Dr. HimanshuDocument40 pagesOxygen Delivery Devices: Dr. HimanshusnezaimNo ratings yet
- O2 Administration ReviewerDocument5 pagesO2 Administration ReviewerDustin Dela CruzNo ratings yet
- Terapi Oksigen Dan Tata Laksana Jalan NapasDocument23 pagesTerapi Oksigen Dan Tata Laksana Jalan NapasFiyandNo ratings yet
- Eathing IDI 2015Document58 pagesEathing IDI 2015Syamsul Bahri AkhasNo ratings yet
- Medx Anesthesia S6100Document2 pagesMedx Anesthesia S6100Luzon MedicalNo ratings yet
- BASIC OXYGEN RESPINA EditDocument51 pagesBASIC OXYGEN RESPINA EditTheopilus Obed LayNo ratings yet
- Comparison of FFP2, KN95, and N95 and Other Filtering Facepiece Respirator ClassesDocument3 pagesComparison of FFP2, KN95, and N95 and Other Filtering Facepiece Respirator ClassesfaithnicNo ratings yet
- Oxygen TherapyDocument21 pagesOxygen TherapyRaymund Christopher Dela PeñaNo ratings yet
- Terapi Oksigen PDFDocument50 pagesTerapi Oksigen PDFelianamuis100% (1)
- Oxygen Concentrator: Main Technical SpecificationsDocument2 pagesOxygen Concentrator: Main Technical SpecificationsBenn BasilNo ratings yet
- Oxygen AdministrationDocument27 pagesOxygen AdministrationakhilNo ratings yet
- NCM 118 Lec Prelim 2Document13 pagesNCM 118 Lec Prelim 2SammNo ratings yet
- Comparison of FFP2, KN95, and N95 and Other Filtering Facepiece Respirator ClassesDocument3 pagesComparison of FFP2, KN95, and N95 and Other Filtering Facepiece Respirator ClassesRavi S DwivedyNo ratings yet
- Niv HFNCDocument15 pagesNiv HFNCFrank VaronaNo ratings yet
- Oxygen TherapyDocument4 pagesOxygen Therapyharold smithNo ratings yet
- Basics of OxygenDocument78 pagesBasics of OxygenClarisse AcacioNo ratings yet
- Anesthesia System: Technical SpecificationDocument2 pagesAnesthesia System: Technical Specificationasep budiyantoNo ratings yet
- DR Kapil Dev Soni - Oxygen Therapy in AdultsDocument39 pagesDR Kapil Dev Soni - Oxygen Therapy in AdultsBhoomika PandeyNo ratings yet
- Philips Ev300 BrochureDocument2 pagesPhilips Ev300 BrochureErick PGNo ratings yet
- Oxygen Therapy: Dr. Aneela HussainDocument30 pagesOxygen Therapy: Dr. Aneela HussainMohammad AliNo ratings yet
- SBMJ 56Document3 pagesSBMJ 56sherryiqbalNo ratings yet
- Oxygen Therapy: by DR Finny Theo, MBBS, (DNB)Document59 pagesOxygen Therapy: by DR Finny Theo, MBBS, (DNB)The Telugu DoctorNo ratings yet
- 4-Oxygen TherapyDocument31 pages4-Oxygen Therapyabdisalaan hassanNo ratings yet
- Oxygen Therapy Sajoo RTDocument34 pagesOxygen Therapy Sajoo RTsajaNo ratings yet
- Administering Oxygen by Nasal CannulaDocument5 pagesAdministering Oxygen by Nasal CannulaAndrea Bayaga WaganNo ratings yet
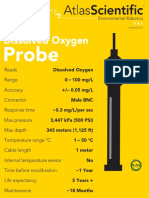
- DO ProbeDocument7 pagesDO ProbeasperfudNo ratings yet
- NIV and HFNCDocument16 pagesNIV and HFNCMarceline GarciaNo ratings yet
- OKSIGENDocument51 pagesOKSIGENlNo ratings yet
- Anaesthesia DFX WorkbookDocument10 pagesAnaesthesia DFX WorkbookSaurav SinghNo ratings yet
- Ventilation Modes and Parameters of Anesthesia MachineDocument2 pagesVentilation Modes and Parameters of Anesthesia MachineLuis RodriguezNo ratings yet
- Post Arrest CareDocument23 pagesPost Arrest CareMohamed RasoolNo ratings yet
- Dr. Subhasis Roy: Consultant, Sisu Sanjiban Hospital, Salt Lake, KolkataDocument19 pagesDr. Subhasis Roy: Consultant, Sisu Sanjiban Hospital, Salt Lake, Kolkatacy_alcantaraNo ratings yet
- Case Study AssigmentDocument8 pagesCase Study AssigmentArvin LabradaNo ratings yet
- Oxygen Therapy For NurseDocument46 pagesOxygen Therapy For NurseselviiNo ratings yet
- (ANES) Sat 05 Pharmacology of Inhalational Anesthetics (A2021)Document3 pages(ANES) Sat 05 Pharmacology of Inhalational Anesthetics (A2021)Ricky Justin NgoNo ratings yet
- (ANES) Sat 01 Ambulatory Anesthesia (A2021)Document3 pages(ANES) Sat 01 Ambulatory Anesthesia (A2021)Ricky Justin NgoNo ratings yet
- Adrenal Crisis Workup in ERDocument16 pagesAdrenal Crisis Workup in ERRicky Justin NgoNo ratings yet
- (ANES) Sat 02 Anesthesia Machine and Equipment (A2021)Document3 pages(ANES) Sat 02 Anesthesia Machine and Equipment (A2021)Ricky Justin NgoNo ratings yet
- MEDICINE 2 – NEPHRO: GENERAL LECTUREDocument13 pagesMEDICINE 2 – NEPHRO: GENERAL LECTURERicky Justin NgoNo ratings yet
- MED NE 1 14 Water-Metabolism-Hypernatremia-HyponatremiaDocument12 pagesMED NE 1 14 Water-Metabolism-Hypernatremia-HyponatremiaRicky Justin NgoNo ratings yet
- MED - IR.L3.MDR Organisms and Antibiotic StewardshipDocument6 pagesMED - IR.L3.MDR Organisms and Antibiotic StewardshipRicky Justin NgoNo ratings yet
- MED - EN.CCD4.When Acute Is Not CuteDocument9 pagesMED - EN.CCD4.When Acute Is Not CuteRicky Justin NgoNo ratings yet
- (OB GRP 2) SGD - Ovarian Cyst in PregnancyDocument4 pages(OB GRP 2) SGD - Ovarian Cyst in PregnancyRicky Justin NgoNo ratings yet
- Cholera Mindmap: Understanding The Disease, Symptoms, and PreventionDocument1 pageCholera Mindmap: Understanding The Disease, Symptoms, and PreventionUlysse BerraNo ratings yet
- Colquitt, LePine, & Noe (2000) JAP PDFDocument30 pagesColquitt, LePine, & Noe (2000) JAP PDFMeyrina PronityastutiNo ratings yet
- Pub Family Practice Examination and Board ReviewDocument937 pagesPub Family Practice Examination and Board ReviewMohammad PharaonNo ratings yet
- Critical Thinking, Clinical Reasoning, and Clinical Judgment, 7eDocument274 pagesCritical Thinking, Clinical Reasoning, and Clinical Judgment, 7eBrianna DoyleNo ratings yet
- Ca Print 1Document134 pagesCa Print 1Kyoko ANo ratings yet
- المعدات وغرف الانتاج والتنظيف والصيانة دليل الطالبDocument56 pagesالمعدات وغرف الانتاج والتنظيف والصيانة دليل الطالبbionorluxeNo ratings yet
- Vital-Action LevelsDocument34 pagesVital-Action LevelsLuis GallegosNo ratings yet
- 818503r10 Manual TAT2000 PDFDocument12 pages818503r10 Manual TAT2000 PDFadrian alonsoNo ratings yet
- G08 Water1 Report 202Document7 pagesG08 Water1 Report 202notmuappleNo ratings yet
- Attachment and Mind Theory in Psychotherapy and Psychopathology of SchizophreniaDocument11 pagesAttachment and Mind Theory in Psychotherapy and Psychopathology of SchizophreniaIris Druț-PerianNo ratings yet
- DR Barbara StarfieldDocument37 pagesDR Barbara StarfieldSuyanto SuyantoNo ratings yet
- Sop For Facility and Equipment Maintenance Management in Primary Health Care Clinic in IraqDocument79 pagesSop For Facility and Equipment Maintenance Management in Primary Health Care Clinic in IraqticoNo ratings yet
- Manual Therapy Interventions For Carpal Tunnel Syndrome A ReviewDocument10 pagesManual Therapy Interventions For Carpal Tunnel Syndrome A ReviewlathifatulNo ratings yet
- HHA - X-MET8000 Optimum + Expert Performance Document (Alloy) - Thin Window - V1-3Document5 pagesHHA - X-MET8000 Optimum + Expert Performance Document (Alloy) - Thin Window - V1-3Paula InesNo ratings yet
- OpenLMIS: Open Source Software for Managing Health Supply ChainsDocument4 pagesOpenLMIS: Open Source Software for Managing Health Supply Chainschibwe chatamaNo ratings yet
- Massive Hemoptysis An Update On The Role of Bronchoscopy in Diagnosis and Management PDFDocument21 pagesMassive Hemoptysis An Update On The Role of Bronchoscopy in Diagnosis and Management PDFdoc_next_doorNo ratings yet
- PDF097Document1 pagePDF097Hao LuoNo ratings yet
- Wahyu Agung Kenworth Motors Case StudyDocument2 pagesWahyu Agung Kenworth Motors Case StudyWahyu Utama100% (1)
- Quantum Academies Program OverviewDocument234 pagesQuantum Academies Program OverviewThomas Marti100% (1)
- Positioning A Client in BedDocument32 pagesPositioning A Client in BedGrape JuiceNo ratings yet
- Indian Journal of Public Health Research and DevelopmentDocument1 pageIndian Journal of Public Health Research and DevelopmentNusa karya engineeringNo ratings yet
- Mental Health DepressionDocument4 pagesMental Health DepressionKAIZEN KINGZNo ratings yet
- Case Study The Teaching HospitalDocument4 pagesCase Study The Teaching HospitalDerick DarkZide100% (4)
- 5 6136226561843528157Document15 pages5 6136226561843528157Om Prakash RajNo ratings yet
- Policy Paper-Bpa108Document6 pagesPolicy Paper-Bpa108Aripin SangcopanNo ratings yet
- Call For Papers: Innovations in Glaucoma Surgery: Improving The ResultsDocument1 pageCall For Papers: Innovations in Glaucoma Surgery: Improving The ResultsYulias YoweiNo ratings yet
- Shapiro (1992) A Preliminary Study of The Long Term MeditatorsDocument18 pagesShapiro (1992) A Preliminary Study of The Long Term MeditatorsMichel AngersNo ratings yet
- Penerapan Model Pembelajaran Problem Based Learning Untuk Meningkatkan Hasil Belajar Siswa Mata Pelajaran PAK Di Kelas V SDN 003 Bintan TimurDocument12 pagesPenerapan Model Pembelajaran Problem Based Learning Untuk Meningkatkan Hasil Belajar Siswa Mata Pelajaran PAK Di Kelas V SDN 003 Bintan Timurrony carolesNo ratings yet
- Chloe Ting - 2 Weeks Shred Challenge - Free Workout ProgramDocument5 pagesChloe Ting - 2 Weeks Shred Challenge - Free Workout ProgramIndecisiveGurl100% (2)
- MR No. Urine Test ResultsDocument1 pageMR No. Urine Test Results112345678900No ratings yet