You might also like
- Essentials of Clinical Toxicology: For 4 Year Medical StudentDocument102 pagesEssentials of Clinical Toxicology: For 4 Year Medical StudentShaban YasserNo ratings yet
- Drug Allergy Symptoms, Causes and Treatment (38 charactersDocument13 pagesDrug Allergy Symptoms, Causes and Treatment (38 charactersAlison ThorpeNo ratings yet
- PHARMACOLOGY HighlightedDocument37 pagesPHARMACOLOGY HighlightedEmeroot RootNo ratings yet
- Drug InteractionDocument24 pagesDrug InteractionChuol Mateat KanNo ratings yet
- Adverse Drug ReactionDocument6 pagesAdverse Drug Reactionpranal patil (Pranal)No ratings yet
- Fighting the Opioid Epidemic: The Role of Providers and the Clinical Laboratory in Understanding Who is VulnerableFrom EverandFighting the Opioid Epidemic: The Role of Providers and the Clinical Laboratory in Understanding Who is VulnerableNo ratings yet
- PT718Document15 pagesPT718Susmita GhoshNo ratings yet
- 1-Poisoning in Children Revised 2021Document63 pages1-Poisoning in Children Revised 2021Jawaher AbdullahNo ratings yet
- Rekonsiliasi Obat 2019Document20 pagesRekonsiliasi Obat 2019Truly SitorusNo ratings yet
- Adverse Drug Effects BDSDocument30 pagesAdverse Drug Effects BDSDr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- Drug-Induced Nausea and Vomiting MechanismsDocument5 pagesDrug-Induced Nausea and Vomiting MechanismsnimasNo ratings yet
- Drug Study EditedDocument8 pagesDrug Study EditedAcob, Jean LykaNo ratings yet
- Drug Interactions: Understanding How Medications Can Affect Each OtherDocument66 pagesDrug Interactions: Understanding How Medications Can Affect Each OtherCatalina BernevecNo ratings yet
- Meso 2022Document82 pagesMeso 2022cindi diaNo ratings yet
- Consumer Chemistry: Quarter 4 - Module 2Document28 pagesConsumer Chemistry: Quarter 4 - Module 2wetlog lolololim100% (2)
- Notes in PharmacologyDocument95 pagesNotes in PharmacologyMylz MendozaNo ratings yet
- New PDF For PharmacologyDocument236 pagesNew PDF For PharmacologyDIPENDRA KUMAR KUSHAWAHA100% (1)
- Pharm - NSG Science - Ppt.prevised2Document86 pagesPharm - NSG Science - Ppt.prevised2RAINBOW40No ratings yet
- Pharmacodynamics: Truly Sitorus, DR., M.Si., SPFKDocument49 pagesPharmacodynamics: Truly Sitorus, DR., M.Si., SPFKAli Alfatsyah JihadillahNo ratings yet
- Medicine Module: Properties and ClassificationDocument15 pagesMedicine Module: Properties and Classificationmelomaniac100% (2)
- Metoclopramide DrugDocument1 pageMetoclopramide DrugMatth N. ErejerNo ratings yet
- Pharmacology 3Document2 pagesPharmacology 3Mharlynne Nezlou L. PoliranNo ratings yet
- Adverse Drug ReactionDocument6 pagesAdverse Drug ReactionNunkoo RajNo ratings yet
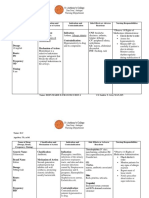
- Drug Action Indications Contraindications Adverse Reaction Nursing ConsiderationDocument2 pagesDrug Action Indications Contraindications Adverse Reaction Nursing ConsiderationEdmarkmoises ValdezNo ratings yet
- Ca1 Pharmacology HandoutDocument15 pagesCa1 Pharmacology Handoutgaboykatkat13No ratings yet
- Maria's Silly Fundamentals 1 (1)Document6 pagesMaria's Silly Fundamentals 1 (1)forbiddenkhfan216No ratings yet
- Principle of Drug ActionDocument15 pagesPrinciple of Drug ActionSeptaPratamaAptNo ratings yet
- Subject Covered in Pharmac y Curriculum: Augment AcademyDocument9 pagesSubject Covered in Pharmac y Curriculum: Augment AcademyRanjith RajapakshaNo ratings yet
- Principles of PharmacotherapyDocument40 pagesPrinciples of Pharmacotherapyjunitria13No ratings yet
- Causative Drugs For Drug Induced Cutaneous ReactionsDocument7 pagesCausative Drugs For Drug Induced Cutaneous ReactionsMiss AmyNo ratings yet
- Notes in PharmacologyDocument96 pagesNotes in Pharmacologydmd_2dd50% (2)
- Clinical Pharmacy QuizDocument3 pagesClinical Pharmacy QuizRoirajiv QuinNo ratings yet
- Unit 1Document15 pagesUnit 1kunalNo ratings yet
- PharmacologyDocument8 pagesPharmacologyJi-Han Abalo ImnidaNo ratings yet
- Quarter 4 Consumer Chemistry Week 1 6Document9 pagesQuarter 4 Consumer Chemistry Week 1 6Johannah SuraitNo ratings yet
- Roger Case Study and Nursing Process 2Document9 pagesRoger Case Study and Nursing Process 2E.R.ONo ratings yet
- Classification: Indication: CNS: Headache,: Name: D.C Age/Sex: 75 Y.o/ MDocument8 pagesClassification: Indication: CNS: Headache,: Name: D.C Age/Sex: 75 Y.o/ MEden Marie FranciscoNo ratings yet
- Drug AllergyDocument12 pagesDrug AllergyDimas Gatra DiantoroNo ratings yet
- Faktor Yang Mempengaruhi Respon ObatDocument23 pagesFaktor Yang Mempengaruhi Respon ObatYelli SidabutarNo ratings yet
- ANA P. BACANI - Activity Assignment 1 Medication ReconciliationDocument5 pagesANA P. BACANI - Activity Assignment 1 Medication ReconciliationAna Paula Bacani-SacloloNo ratings yet
- CR 2Document15 pagesCR 2tyleree3No ratings yet
- Saftey Margin & Drug ToxicityDocument27 pagesSaftey Margin & Drug Toxicitysubhashish01No ratings yet
- Medication Administration: 6 RightsDocument1 pageMedication Administration: 6 RightsKaren MatiasNo ratings yet
- CHAPTER 1 PharmacologyDocument21 pagesCHAPTER 1 PharmacologyGia Espinosa OcbeñaNo ratings yet
- Farmakogenetik FarmakogenomikDocument20 pagesFarmakogenetik FarmakogenomikNovi Siska AmaliaNo ratings yet
- Pharmacology Card Question ReviewDocument4 pagesPharmacology Card Question ReviewRedw AnNo ratings yet
- Drugallergy: Abdul Waheed,, Tiffany Hill,, Nidhi DhawanDocument8 pagesDrugallergy: Abdul Waheed,, Tiffany Hill,, Nidhi DhawanHusni mubarakNo ratings yet
- 1 Introduction To Pharmacology: 1.1 BackgroundDocument10 pages1 Introduction To Pharmacology: 1.1 BackgroundDental LecturesMMQNo ratings yet
- Clinical Condition and Medication Therapy of AmoxiDocument3 pagesClinical Condition and Medication Therapy of AmoxiRina HerowatiNo ratings yet
- Ampicillin 2Document1 pageAmpicillin 2Kristine YoungNo ratings yet
- Mechanism-Based Strategies for Preventing Adverse Drug ReactionsDocument2 pagesMechanism-Based Strategies for Preventing Adverse Drug Reactionsmegazhang94No ratings yet
- Benzodiazepine Allergy With Anesthesia Administration: A Review of Current LiteratureDocument8 pagesBenzodiazepine Allergy With Anesthesia Administration: A Review of Current LiteratureWahyudi WahyudiNo ratings yet
- Introduction Definitions and Sources of DrugsDocument4 pagesIntroduction Definitions and Sources of Drugssindhu mNo ratings yet
- Untitled Document-4Document10 pagesUntitled Document-4Redw AnNo ratings yet
- Drug InteractionsDocument36 pagesDrug Interactionsbaker371100% (2)
- Cology Text Book - CompressedDocument168 pagesCology Text Book - CompressedChillones GamingNo ratings yet
- Pharmacology For Nursing Care 6e Test BankDocument36 pagesPharmacology For Nursing Care 6e Test Banknaturedammitej0k0b100% (26)
- Application Letter FormatDocument1 pageApplication Letter FormatIsabel PeraltaNo ratings yet
- Exercise 5 - QC 1Document2 pagesExercise 5 - QC 1Isabel PeraltaNo ratings yet
- BATCH MANUFACTURING RECORD FOR ATORVASTATIN TABLETSDocument4 pagesBATCH MANUFACTURING RECORD FOR ATORVASTATIN TABLETSIsabel PeraltaNo ratings yet
- Act-S&i - Oc B6 - G4Document1 pageAct-S&i - Oc B6 - G4Isabel PeraltaNo ratings yet
- ACT. 4 WarehouseDocument2 pagesACT. 4 WarehouseIsabel PeraltaNo ratings yet
- Final Ampule Box Esquijo LopezDocument1 pageFinal Ampule Box Esquijo LopezIsabel PeraltaNo ratings yet
- APPGP MFG OC G4 PD UNIT DOSE AND BATCH FORMULATIONDocument5 pagesAPPGP MFG OC G4 PD UNIT DOSE AND BATCH FORMULATIONIsabel PeraltaNo ratings yet
- Activity 2BUSINESSPLANDocument3 pagesActivity 2BUSINESSPLANIsabel PeraltaNo ratings yet
- Chest Rub Ointment ExperimentDocument2 pagesChest Rub Ointment ExperimentIsabel PeraltaNo ratings yet
- Ppgp-Mfg-Oc G3 - Pd-2 - CP, CPP, Cqa NOTES On The ActivityDocument5 pagesPpgp-Mfg-Oc G3 - Pd-2 - CP, CPP, Cqa NOTES On The ActivityIsabel Peralta50% (2)
- PPGP MFG Oc g4 PD Unit Dose and Batch FormulationDocument3 pagesPPGP MFG Oc g4 PD Unit Dose and Batch FormulationIsabel PeraltaNo ratings yet
- PHM 302L: Pharmacognosy and Plant Chemistry: Week 4: Experiment 9 ResinsDocument23 pagesPHM 302L: Pharmacognosy and Plant Chemistry: Week 4: Experiment 9 ResinsIsabel PeraltaNo ratings yet
- Methyl Salicylate Menthol Camphor Chest RubDocument1 pageMethyl Salicylate Menthol Camphor Chest RubIsabel PeraltaNo ratings yet
- Chlorides of Sodium, Calcium and Potassium Chlorides of Sodium, Calcium and PotassiumDocument1 pageChlorides of Sodium, Calcium and Potassium Chlorides of Sodium, Calcium and PotassiumIsabel PeraltaNo ratings yet
- FPPGP MFG OC G4 PD UNIT DOSE AND BATCH FORMULATIONDocument4 pagesFPPGP MFG OC G4 PD UNIT DOSE AND BATCH FORMULATIONIsabel PeraltaNo ratings yet
- Email Worksheet OverviewDocument27 pagesEmail Worksheet OverviewIsabel PeraltaNo ratings yet
- GRP4Integrated Application Form XLSX FormatDocument15 pagesGRP4Integrated Application Form XLSX FormatIsabel PeraltaNo ratings yet
- Isabel P. Esquijo Bs Pharmacy Science, Technology and SocietyDocument2 pagesIsabel P. Esquijo Bs Pharmacy Science, Technology and SocietyIsabel PeraltaNo ratings yet
- Factors to Consider in Developing Nutraceuticals and Dietary SupplementsDocument5 pagesFactors to Consider in Developing Nutraceuticals and Dietary SupplementsIsabel PeraltaNo ratings yet
- Assignment A. List Down The Processes in Drug Development and Explain EachDocument2 pagesAssignment A. List Down The Processes in Drug Development and Explain EachIsabel PeraltaNo ratings yet
- Experiment 1 LABELDocument6 pagesExperiment 1 LABELIsabel PeraltaNo ratings yet
- Calculation of Doses - General ConsiderationsDocument30 pagesCalculation of Doses - General Considerationsalibel caballeroNo ratings yet
- Perpetual Help College of Manila: Business PlanDocument14 pagesPerpetual Help College of Manila: Business PlanIsabel PeraltaNo ratings yet
- PHM304: Microbiology and Parasitology: Week 2: Parasitic InfectionDocument36 pagesPHM304: Microbiology and Parasitology: Week 2: Parasitic InfectionIsabel PeraltaNo ratings yet
- Assignment 2Document2 pagesAssignment 2Isabel PeraltaNo ratings yet
- Experiment 1 LABELDocument6 pagesExperiment 1 LABELIsabel PeraltaNo ratings yet
- Sodium Phosphate Oral Solution UsesDocument7 pagesSodium Phosphate Oral Solution UsesIsabel PeraltaNo ratings yet
- Mangifera IndicaDocument19 pagesMangifera IndicaChelo Jan GeronimoNo ratings yet
- Case StudyDocument3 pagesCase StudyElisha Grace Gumal-inNo ratings yet
- Bunga Telang Utk DiabetesDocument7 pagesBunga Telang Utk DiabetesKong Kim LengNo ratings yet
- Chromium Supplementation For Women With Gestational Diabetes MellitusDocument7 pagesChromium Supplementation For Women With Gestational Diabetes MellitusSarly FebrianaNo ratings yet
- Soal Latihan PAS Kls 12Document12 pagesSoal Latihan PAS Kls 12rong rong14No ratings yet
- Overt Diabetes in PregnancyDocument12 pagesOvert Diabetes in PregnancyGestne AureNo ratings yet
- American Heart Association Guide For Improving Cardiovascular HealthDocument24 pagesAmerican Heart Association Guide For Improving Cardiovascular HealthLorena Galindo GuerreroNo ratings yet
- DLL Week 11 15Document13 pagesDLL Week 11 15Rasell de Luna100% (1)
- Afghanistan EssayDocument6 pagesAfghanistan Essaylpuaduwhd100% (2)
- Rina AmeliaDocument12 pagesRina AmeliaDerison MarsinovaNo ratings yet
- Insulin InjectionDocument7 pagesInsulin InjectionIrse P Bani MusaNo ratings yet
- Journal of Functional Foods: Douglas Xavier-Santos, Raquel Bedani, Egidio Dorea Lima, Susana Marta Isay Saad TDocument17 pagesJournal of Functional Foods: Douglas Xavier-Santos, Raquel Bedani, Egidio Dorea Lima, Susana Marta Isay Saad Thyuck babyNo ratings yet
- Practical guide to handling prescriptions and identifying drug interactionsDocument45 pagesPractical guide to handling prescriptions and identifying drug interactionsShivam Das, Tehsil KulpaharNo ratings yet
- Korelasi SMWT Dan DMDocument4 pagesKorelasi SMWT Dan DMPutriNo ratings yet
- Analogos de Insulina, Farmacocinética y FarmacodinamiaDocument11 pagesAnalogos de Insulina, Farmacocinética y FarmacodinamiaAlin VázquezNo ratings yet
- Patient Counselling For DiseasesDocument18 pagesPatient Counselling For DiseasesYathrika YathrikaNo ratings yet
- ACE Personal Trainer Manual Chapter 13Document59 pagesACE Personal Trainer Manual Chapter 13Đạt NguyễnNo ratings yet
- Type 1 diabetes exercise consensus statement reviewDocument14 pagesType 1 diabetes exercise consensus statement reviewArie AnggaNo ratings yet
- Prevention and Control of Diseases and DisordersDocument39 pagesPrevention and Control of Diseases and DisordersAprille Maye CayogNo ratings yet
- Functional Medicine Intake Final 07-17-12Document34 pagesFunctional Medicine Intake Final 07-17-12lianaidrisNo ratings yet
- Associations Between Dental Caries and Systemic Diseases: A Scoping ReviewDocument35 pagesAssociations Between Dental Caries and Systemic Diseases: A Scoping ReviewLeila FrotaNo ratings yet
- Diet & Disease PPT 2021 - Final EditedDocument156 pagesDiet & Disease PPT 2021 - Final Editedbonsa JalataNo ratings yet
- Medical Care of Adults With Down Syndrome A Clinical GuidelineDocument14 pagesMedical Care of Adults With Down Syndrome A Clinical GuidelineStephany Caroline Menezes da SilvaNo ratings yet
- Antidiabetic Effect of Lonicera Ligustrina in Alloxan Induced DiabetesDocument8 pagesAntidiabetic Effect of Lonicera Ligustrina in Alloxan Induced DiabetessrirampharmNo ratings yet
- Visceral FatDocument5 pagesVisceral FatClint BodungenNo ratings yet
- The Effect of Diabetic Foot Exercises on Foot Sensitivity in Patients with Type 2 DiabetesDocument6 pagesThe Effect of Diabetic Foot Exercises on Foot Sensitivity in Patients with Type 2 Diabetesmaarifah ifahNo ratings yet
- 204-Article Text-390-1-10-20200504 PDFDocument8 pages204-Article Text-390-1-10-20200504 PDFBram DaudNo ratings yet
- JNEP2019Document7 pagesJNEP2019Maheboob GanjalNo ratings yet
- A New Mouse Model of Type 2 Diabetes Mellitus Established Through Combination of High-Fat Diet, Streptozotocin and Glucocorticoid PDFDocument7 pagesA New Mouse Model of Type 2 Diabetes Mellitus Established Through Combination of High-Fat Diet, Streptozotocin and Glucocorticoid PDFSoni Sunarso SNo ratings yet
- 06 DiabetesDocument40 pages06 DiabetesAgnigundala Varun RaoNo ratings yet