You might also like
- Health Assessment 16Document11 pagesHealth Assessment 16shannon c. lewisNo ratings yet
- Deep Vein Thrombosis (NCP)Document4 pagesDeep Vein Thrombosis (NCP)24 PAULINO ALDRIN MUJAR0% (1)
- Peripheral AssessmentDocument9 pagesPeripheral AssessmentKinn NohaNo ratings yet
- Vascular SystemDocument33 pagesVascular SystemCarl Elexer Cuyugan Ano100% (3)
- Physical Signs: Download A Copy of This Study GuideDocument16 pagesPhysical Signs: Download A Copy of This Study Guidebjpalmer100% (3)
- Talley Sum Up ExaminationDocument57 pagesTalley Sum Up ExaminationGroup 14No ratings yet
- Drajat Leg UlcerDocument28 pagesDrajat Leg Ulcerdila2706No ratings yet
- IMPERIAL CARDIODocument6 pagesIMPERIAL CARDIODelos Santos John Lorenz ANo ratings yet
- AV Fistula ExamDocument4 pagesAV Fistula ExamKay BristolNo ratings yet
- Assessing The Peripheral-Vascular and Lymphatic SystemsDocument6 pagesAssessing The Peripheral-Vascular and Lymphatic SystemsElaisha Mae C. CarsulaNo ratings yet
- Ulcers, The Diabetic FootDocument10 pagesUlcers, The Diabetic FootmuhammadridhwanNo ratings yet
- Abdominal Assessment Key Points in Abdominal Physical ExaminationDocument19 pagesAbdominal Assessment Key Points in Abdominal Physical Examinationshannon c. lewisNo ratings yet
- Neuro Assessment ReportDocument9 pagesNeuro Assessment Reportcosmic latte pulpsNo ratings yet
- RELIEVING HEMORRHOID PAIN THROUGH NURSING INTERVENTIONSDocument3 pagesRELIEVING HEMORRHOID PAIN THROUGH NURSING INTERVENTIONSKaye OrtegaNo ratings yet
- PVD and Hematologic Disorders.Document9 pagesPVD and Hematologic Disorders.nycaNo ratings yet
- Raynauds and Buerguers DiseaseDocument3 pagesRaynauds and Buerguers DiseaseCHRISTIE MONTANO100% (1)
- PHYSICAL ASSESSMENT 2 GUIDEDocument19 pagesPHYSICAL ASSESSMENT 2 GUIDEjoanne.garciaNo ratings yet
- Health Assessment: AbdomenDocument18 pagesHealth Assessment: AbdomenBatiao Camille ClaireNo ratings yet
- General Physical Assessment: C. Richard Finley, Ed.D, PA-CDocument56 pagesGeneral Physical Assessment: C. Richard Finley, Ed.D, PA-CAlfina Aulia RizkiNo ratings yet
- Complex Wounds 2020Document38 pagesComplex Wounds 2020Ài ZìjǐNo ratings yet
- 1 OutlineDocument5 pages1 OutlinemickeyNo ratings yet
- Assessing AbdomenDocument33 pagesAssessing Abdomenjaypee01No ratings yet
- Score: 7: High Likelihood of AppendicitisDocument2 pagesScore: 7: High Likelihood of AppendicitisMichelle Vera GabunNo ratings yet
- Neuromusculosklatal Disorders FK UnayaDocument62 pagesNeuromusculosklatal Disorders FK UnayaSuci MayveraNo ratings yet
- Appendicitis Diagnosis and Treatment in 40 CharactersDocument14 pagesAppendicitis Diagnosis and Treatment in 40 CharactersNica EnriquezNo ratings yet
- Leg UlcerDocument28 pagesLeg UlcerRanindya PutriNo ratings yet
- 17 Epidermal New GrowthsDocument3 pages17 Epidermal New GrowthsWaiwit KritayakiranaNo ratings yet
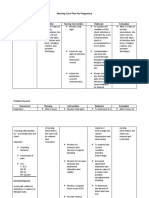
- Nursing Care Plan for Pregnancy Risk DiagnosisDocument2 pagesNursing Care Plan for Pregnancy Risk DiagnosisCheska PalomaNo ratings yet
- Varicose Case ProformaDocument2 pagesVaricose Case ProformaSneha Naulakha100% (1)
- Appendicitis: Basic Information DiagnosisDocument5 pagesAppendicitis: Basic Information DiagnosisCarlos Meza HernandezNo ratings yet
- Apendisitis: Ronny S, DR, SpotDocument34 pagesApendisitis: Ronny S, DR, SpotLili ManaoNo ratings yet
- Postpartal ThrombophlebitisDocument8 pagesPostpartal ThrombophlebitisnursereviewNo ratings yet
- 4 Abdominal+ExaminationDocument9 pages4 Abdominal+Examinationمرتضى حسين عبدNo ratings yet
- Chemotherapy Extravasation-MinDocument17 pagesChemotherapy Extravasation-Minapi-405380855No ratings yet
- Postpartal Thrombophlebitis: Client Assessment Data Base Activity/RestDocument8 pagesPostpartal Thrombophlebitis: Client Assessment Data Base Activity/RestLei OrtegaNo ratings yet
- SGD AppendicitisDocument11 pagesSGD Appendicitisนีล ไบรอันNo ratings yet
- Post-Partum Assessment: ProfileDocument15 pagesPost-Partum Assessment: ProfileMenly SusadaNo ratings yet
- Assessment Diagnosis Planning Implementation Evaluation Interventions Rationale Subjective Data: Na Independent: Goal MetDocument34 pagesAssessment Diagnosis Planning Implementation Evaluation Interventions Rationale Subjective Data: Na Independent: Goal MetHydie Mae AlcabedosNo ratings yet
- Cardiovascular ExaminationDocument10 pagesCardiovascular ExaminationSaurabh PaudyalNo ratings yet
- Examination of AbdomenDocument4 pagesExamination of Abdomengen. wadayioo samejoNo ratings yet
- H.A. Lec (L8 D) - Peripheral Vascular AssessmentDocument7 pagesH.A. Lec (L8 D) - Peripheral Vascular AssessmentCastallia LascuñaNo ratings yet
- IV Surgery PDFDocument265 pagesIV Surgery PDFاللهم أصلح أمريNo ratings yet
- Osce: Internal Medicine 1. JVP Measurement: © FAAS 3A, 2018Document11 pagesOsce: Internal Medicine 1. JVP Measurement: © FAAS 3A, 2018PatNo ratings yet
- Varicose VeinsDocument37 pagesVaricose VeinsJavier SaadNo ratings yet
- Ortho ReportDocument58 pagesOrtho ReportheyyymeeeNo ratings yet
- SKIN EXAM: STRUCTURE, FUNCTION, ASSESSMENTDocument67 pagesSKIN EXAM: STRUCTURE, FUNCTION, ASSESSMENTFelya Elsa Pratiwi KurniaNo ratings yet
- Physical Diagnosis Overview Guide ScribdDocument117 pagesPhysical Diagnosis Overview Guide ScribdTrisNo ratings yet
- Transe 1Document2 pagesTranse 1lija.medija.swuNo ratings yet
- Wrist and Hand Disease Description Pathophysiology Sign and Symptoms Management Carpal Tunnel SyndromeDocument4 pagesWrist and Hand Disease Description Pathophysiology Sign and Symptoms Management Carpal Tunnel SyndromeMei BejeranoNo ratings yet
- Peripheral Vascular Diseases GuideDocument4 pagesPeripheral Vascular Diseases GuideJulia Rae Delos SantosNo ratings yet
- Care of Clients in Emergent ConditionsDocument15 pagesCare of Clients in Emergent ConditionsJheanAlphonsineT.MeansNo ratings yet
- Head to Toe Assessment of Emergent ConditionsDocument19 pagesHead to Toe Assessment of Emergent ConditionsJheanAlphonsineT.MeansNo ratings yet
- FIX Leg UlcerDocument59 pagesFIX Leg UlcerDekka Andra100% (2)
- Romeo NCPDocument3 pagesRomeo NCPAnna LouisaNo ratings yet
- Ulcer Case by S.P.KamthankarDocument14 pagesUlcer Case by S.P.KamthankarJaweria SyedNo ratings yet
- Type of The Wound-JCF 4thDocument25 pagesType of The Wound-JCF 4thTaufik HidayantoNo ratings yet
- DeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Hand Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentFrom EverandHand Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentNo ratings yet
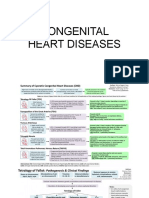
- Congenital Heart DiseasesDocument8 pagesCongenital Heart DiseasesCraigyyNo ratings yet
- Nursing Care of at Risk - High Risk - Sick Client Newborn To Adolescent Summary by JeffDocument11 pagesNursing Care of at Risk - High Risk - Sick Client Newborn To Adolescent Summary by JeffCraigyyNo ratings yet
- CVD TableDocument8 pagesCVD TableCraigyyNo ratings yet
- Enzyme and Vitamins, BiochemDocument2 pagesEnzyme and Vitamins, BiochemCraigyyNo ratings yet
- LEARNING ACTIVITY 11 - Nervous SystemDocument4 pagesLEARNING ACTIVITY 11 - Nervous SystemCraigyyNo ratings yet
- Bed MakingDocument4 pagesBed MakingCraigyyNo ratings yet
- Learning Activity 15 - Muscular SystemDocument3 pagesLearning Activity 15 - Muscular SystemCraigyyNo ratings yet
- 2020 Health Goals - Prevent Labor ComplicationsDocument1 page2020 Health Goals - Prevent Labor ComplicationsCraigyyNo ratings yet
- Assessing Blood PressureDocument4 pagesAssessing Blood PressureCraigyyNo ratings yet
- Parts and Functions of a MicroscopeDocument2 pagesParts and Functions of a MicroscopeCraigyyNo ratings yet
- Forum 2Document1 pageForum 2CraigyyNo ratings yet
- Fire Prevention - DauranDocument1 pageFire Prevention - DauranCraigyyNo ratings yet
- Assessing an Apical Pulse RateDocument2 pagesAssessing an Apical Pulse RateCraigyyNo ratings yet
- Assessment of HeartDocument4 pagesAssessment of HeartCraigyyNo ratings yet
- Assessing AbdomenDocument9 pagesAssessing AbdomenCraigyyNo ratings yet
- Assessing Respirations GuideDocument1 pageAssessing Respirations GuideCraigyyNo ratings yet
- Nursing Skills ChecklistDocument6 pagesNursing Skills ChecklistCraigyyNo ratings yet
- Eyes ChecklistDocument2 pagesEyes ChecklistCraigyyNo ratings yet
- 5-Week Bike Exercise Program Week 1Document1 page5-Week Bike Exercise Program Week 1CraigyyNo ratings yet
- The 4 Basic Tissue Types in The Human BodyDocument4 pagesThe 4 Basic Tissue Types in The Human Bodybeeluvit81444No ratings yet
- Bed Bath ProcedureDocument3 pagesBed Bath ProcedureCraigyyNo ratings yet
- DAVAO DOCTORS COLLEGE NURSING CARE PLAN FOR GDMDocument3 pagesDAVAO DOCTORS COLLEGE NURSING CARE PLAN FOR GDMkkd nyleNo ratings yet
- JP Drain CareDocument2 pagesJP Drain Carecarl delgadoNo ratings yet
- Theoretical Framewrok in Nursing By: May Vallerie V. Sarmiento RN Prof. Erlinda E. Domingo RN., MPH., Ceso Iv Professor IIIDocument27 pagesTheoretical Framewrok in Nursing By: May Vallerie V. Sarmiento RN Prof. Erlinda E. Domingo RN., MPH., Ceso Iv Professor IIIenam professorNo ratings yet
- NURS209 Case Presentation: Heart Failure ManagementDocument5 pagesNURS209 Case Presentation: Heart Failure ManagementWendera T. S CooperNo ratings yet
- Chickenpox Case StudyDocument12 pagesChickenpox Case Studywan yuen kiNo ratings yet
- Adderall Risks - Much More Than You Wanted To Know - Slate Star CodexDocument21 pagesAdderall Risks - Much More Than You Wanted To Know - Slate Star CodexPatrick LumambaNo ratings yet
- 2021 ESC Guidelines For The Diagnosis and Treatment of Acute and Chronic Heart FailureDocument128 pages2021 ESC Guidelines For The Diagnosis and Treatment of Acute and Chronic Heart Failureidirectored5438No ratings yet
- Aspirin Drug StudyDocument3 pagesAspirin Drug StudyIRISH CACAYANNo ratings yet
- 11 Domestic Violence Detection Amid The COVID-19Document5 pages11 Domestic Violence Detection Amid The COVID-19pequitas1522No ratings yet
- Mechanism of Action, Indications, Administration and Side Effects of RisperidoneDocument2 pagesMechanism of Action, Indications, Administration and Side Effects of RisperidoneLanzen DragneelNo ratings yet
- Pembrolizumab and Atezolizumab in TNBCDocument11 pagesPembrolizumab and Atezolizumab in TNBCasdffdsaNo ratings yet
- Etiology 1-Deficiency of Vitamin B1 (Thiamin) 2 - PathogenesisDocument139 pagesEtiology 1-Deficiency of Vitamin B1 (Thiamin) 2 - PathogenesisAlston Foods BVNo ratings yet
- Ventricular Tachycardia Storm Management in ADocument6 pagesVentricular Tachycardia Storm Management in Aselandia nisrinaNo ratings yet
- Diabetes InsipidusDocument2 pagesDiabetes InsipidusDanielle Ann ChiongNo ratings yet
- Data Sheet Data Sheet: Gelafusal GelafusalDocument2 pagesData Sheet Data Sheet: Gelafusal Gelafusalfahri azwarNo ratings yet
- Assesment For Burns and Fluid Calculation PDFDocument10 pagesAssesment For Burns and Fluid Calculation PDFRagaviNo ratings yet
- Consent HifuDocument2 pagesConsent HifuScribdTranslationsNo ratings yet
- Informe DEMO Del Holter de Arritmia Contec TLC9803Document14 pagesInforme DEMO Del Holter de Arritmia Contec TLC9803Edward MoralesNo ratings yet
- Basic Radiation Oncology Beyzadeoglu 2 Ed 2022Document541 pagesBasic Radiation Oncology Beyzadeoglu 2 Ed 2022Alexandr MateașNo ratings yet
- NDSAID Pan MangementDocument91 pagesNDSAID Pan MangementEslam EzzatNo ratings yet
- Hypochondriasis and Health Anxiety - A Guide For Clinicians (PDFDrive)Document289 pagesHypochondriasis and Health Anxiety - A Guide For Clinicians (PDFDrive)Fernanda SilvaNo ratings yet
- History TakingDocument4 pagesHistory TakingaliNo ratings yet
- Hypertensive Disorder in PregnancyDocument7 pagesHypertensive Disorder in PregnancyBiscuits and milkNo ratings yet
- Health Problems and RemediesDocument2 pagesHealth Problems and RemediesAdrienn Kolonicsné KocsisNo ratings yet
- Karakteristik Pasien Kanker Serviks Di Rsud Dr. Soetomo Surabaya Periode Januari - Desember 2017Document4 pagesKarakteristik Pasien Kanker Serviks Di Rsud Dr. Soetomo Surabaya Periode Januari - Desember 2017gita rahayuNo ratings yet
- EPALS DKA Flowchart Jan 23 V4Document1 pageEPALS DKA Flowchart Jan 23 V4Miguel BaiaNo ratings yet
- Chapter 61 Atypical and Parafungal AgentsDocument18 pagesChapter 61 Atypical and Parafungal AgentsbartsnewNo ratings yet
- Vertiginous EpilepsyDocument5 pagesVertiginous Epilepsyzudan2013No ratings yet
- 1 - Cervical CancerDocument87 pages1 - Cervical Cancerzuzuyasi65No ratings yet
- Sports InjuryDocument31 pagesSports InjuryANTONETTE DUMALENo ratings yet