You might also like
- Heart Failure - Nursing ManagementDocument9 pagesHeart Failure - Nursing ManagementAuni Akif Aleesa100% (1)
- URGE SURFING-DBT For Sub Use PDFDocument5 pagesURGE SURFING-DBT For Sub Use PDFAmy Powers100% (1)
- Treat Inflammation and Allergies with Hydrocortisone Sodium SuccinateDocument3 pagesTreat Inflammation and Allergies with Hydrocortisone Sodium SuccinateJesrel DelotaNo ratings yet
- S - LANSS Questionnaire Polish VersionDocument4 pagesS - LANSS Questionnaire Polish VersionBartosz Zaczek100% (1)
- Molero-AlabauGonzalez-AscasoHernandez-Romero - Effects of Torso Mesh Density and Electrode Distri...Document10 pagesMolero-AlabauGonzalez-AscasoHernandez-Romero - Effects of Torso Mesh Density and Electrode Distri...jmescalanteNo ratings yet
- 1471 2474 14 364Document6 pages1471 2474 14 364Luqmanul HakimNo ratings yet
- Bio Impedance Monitoring For Physicians 1Document35 pagesBio Impedance Monitoring For Physicians 1ChiquinquiraNo ratings yet
- Abstract-ISMRM 1351, 2011Document1 pageAbstract-ISMRM 1351, 2011shehadaNo ratings yet
- 08 JMSEDoddethermal Modeling ElectrosurgeryDocument8 pages08 JMSEDoddethermal Modeling ElectrosurgerydelacotteNo ratings yet
- Jurnal 4 RickyDocument6 pagesJurnal 4 RickyAde RyanNo ratings yet
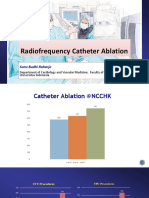
- Raharjo SB - 2018 - Conventional AblationDocument37 pagesRaharjo SB - 2018 - Conventional AblationZulhelmiNo ratings yet
- Aryana 2022Document11 pagesAryana 2022Marcos DuarteNo ratings yet
- Bio Impedance For Physicians Rev1Document35 pagesBio Impedance For Physicians Rev1roan2No ratings yet
- A New Four-Electrode Focused Impedance Measurement (FIM) System For Physiological StudyDocument6 pagesA New Four-Electrode Focused Impedance Measurement (FIM) System For Physiological StudygpaivNo ratings yet
- J Applied Clin Med Phys - 2023 - Ikeda - Impact of CT Scan Parameters On Deformable Image Registration Accuracy UsingDocument9 pagesJ Applied Clin Med Phys - 2023 - Ikeda - Impact of CT Scan Parameters On Deformable Image Registration Accuracy UsingPiotr JankowskiNo ratings yet
- Endocardial Infarct Scar Recognition by MyocardialDocument8 pagesEndocardial Infarct Scar Recognition by MyocardialMihai-Marian RuseiNo ratings yet
- Effects of Diode Laser (810 NM) Irradiation On Root Canal Walls: Thermographic and Morphological StudiesDocument4 pagesEffects of Diode Laser (810 NM) Irradiation On Root Canal Walls: Thermographic and Morphological StudiesendodoncistaNo ratings yet
- J of Cosmetic Dermatology - 2020 - Ruff - Thermal Effects of Percutaneous Application of Plasma Radiofrequency Energy OnDocument7 pagesJ of Cosmetic Dermatology - 2020 - Ruff - Thermal Effects of Percutaneous Application of Plasma Radiofrequency Energy OnVanessaGGSNo ratings yet
- Investigation of Temperature Effects of A Low-Level Laser Source Within The Muscle PhantomDocument5 pagesInvestigation of Temperature Effects of A Low-Level Laser Source Within The Muscle PhantomInternational Journal of Advances in Applied Sciences (IJAAS)No ratings yet
- Kramer2009 SkinDocument6 pagesKramer2009 SkinEdwin CallejasNo ratings yet
- safety limits fortDCSDocument2 pagessafety limits fortDCSlabsoneducationNo ratings yet
- Treating Cardiac Disease with Catheter-Based Tissue HeatingDocument20 pagesTreating Cardiac Disease with Catheter-Based Tissue HeatingMuhammed Luthufi ENo ratings yet
- 2.2 Saito2004Document5 pages2.2 Saito2004CamiloNo ratings yet
- Safe Energy Use in The Operating RoomDocument22 pagesSafe Energy Use in The Operating RoomBolivar IseaNo ratings yet
- Application Ofasub-0.1-Mm3 Implantable Mote Forinvivo Real-Time Wireless Temperature SensingDocument10 pagesApplication Ofasub-0.1-Mm3 Implantable Mote Forinvivo Real-Time Wireless Temperature SensingSomeBitchIKnowNo ratings yet
- Malignant Kidney Tumor AblationDocument4 pagesMalignant Kidney Tumor AblationMahamoodNo ratings yet
- Ki Energy Protects Insolated Rat Liver Mitochond From Oxidative InjuryDocument8 pagesKi Energy Protects Insolated Rat Liver Mitochond From Oxidative InjuryHordepNo ratings yet
- Low-Cost Body Impedance Analyzer For Healthcare ApplicationsDocument4 pagesLow-Cost Body Impedance Analyzer For Healthcare ApplicationsgpaivNo ratings yet
- Feasibility Study On Fabric-Sheet Unified Sensing Electrode For Non-Contact In-Bed Measurements of ECG, Body Proximity and Respiratory MovementDocument4 pagesFeasibility Study On Fabric-Sheet Unified Sensing Electrode For Non-Contact In-Bed Measurements of ECG, Body Proximity and Respiratory Movementmafia criminalNo ratings yet
- Recent Article On Long Wave Diathermy-1Document5 pagesRecent Article On Long Wave Diathermy-1Asad AnZariNo ratings yet
- Magnetic Compare To EsDocument4 pagesMagnetic Compare To EsNakarit SangsirinawinNo ratings yet
- Temperature Distribution in Tissues From A Regular Array of Hot Source Implants An Analytical ApproximationDocument10 pagesTemperature Distribution in Tissues From A Regular Array of Hot Source Implants An Analytical ApproximationHendrick ST., MTNo ratings yet
- A Full-Wave Numerical Assessment of Microwave Tomography For Monitoring Cancer AblationDocument4 pagesA Full-Wave Numerical Assessment of Microwave Tomography For Monitoring Cancer AblationhosseinNo ratings yet
- HIGH EFFICIENCY CARDIAC SYSTEMDocument32 pagesHIGH EFFICIENCY CARDIAC SYSTEMKshitij PawarNo ratings yet
- Absorbed Dose in Mgy From CT ScannersDocument9 pagesAbsorbed Dose in Mgy From CT Scannerscebuano88No ratings yet
- 10 1002@mp 16199Document19 pages10 1002@mp 16199Nima SalianiNo ratings yet
- Comparative Analysis of Savitzky-Golay and Butterworth Filters For Electrocardiogram De-Noising Using Daubechies WaveletsDocument16 pagesComparative Analysis of Savitzky-Golay and Butterworth Filters For Electrocardiogram De-Noising Using Daubechies WaveletsKota Krishna DheerajNo ratings yet
- Mahuvava C Et Al. (2022)Document13 pagesMahuvava C Et Al. (2022)Courage MahuvavaNo ratings yet
- Wristwearable Bioelectrical Impedance Analyzer With Miniature Electrodes For Daily Obesity Management2021scientific ReportsOpen AccessDocument10 pagesWristwearable Bioelectrical Impedance Analyzer With Miniature Electrodes For Daily Obesity Management2021scientific ReportsOpen AccessJulian Alberto Rojas MejiaNo ratings yet
- Effects of Electromagnetic Fields On Human Beings and Electronic DevicesDocument2 pagesEffects of Electromagnetic Fields On Human Beings and Electronic DevicesMohamed SayedNo ratings yet
- Radiation MeasurementsDocument6 pagesRadiation Measurementsالفيزياء الطبيةNo ratings yet
- 1 s2.0 S0360301622004187 MainDocument10 pages1 s2.0 S0360301622004187 Mainbo zhaoNo ratings yet
- Informe Nasa DalzielDocument114 pagesInforme Nasa DalzielluchomnzkuNo ratings yet
- Article 118Document7 pagesArticle 118Disha SojraniNo ratings yet
- Thermography in Dentistry-RevisitedDocument5 pagesThermography in Dentistry-RevisitedkittumdsNo ratings yet
- 2004 IEEE Conference on Nanotechnology Bone Nano-Transducer AbstractDocument2 pages2004 IEEE Conference on Nanotechnology Bone Nano-Transducer Abstractalexis jonathanNo ratings yet
- FTP IvanenkioDocument5 pagesFTP Ivanenkiorwong1231No ratings yet
- Ultrasonic Imaging of The Internal Vibration of Soft Tissue Under Forced VibrationDocument2 pagesUltrasonic Imaging of The Internal Vibration of Soft Tissue Under Forced Vibrationjuliogomez008No ratings yet
- Affect of Ultrashort Electron Beams On The Escherichea Coli SurvivalDocument7 pagesAffect of Ultrashort Electron Beams On The Escherichea Coli SurvivalIJAR JOURNALNo ratings yet
- Wound Heling AmperageDocument8 pagesWound Heling AmperagegamalramadiNo ratings yet
- LabVIEW Based EIS DataInterpreter 01Document1 pageLabVIEW Based EIS DataInterpreter 01Tushar Kanti BeraNo ratings yet
- 00924690Document2 pages00924690dyahputriaNo ratings yet
- Bene CH 2010Document14 pagesBene CH 2010Maria Clara BrandãoNo ratings yet
- ManuscriptDocument9 pagesManuscriptCélio MarquesNo ratings yet
- Review Article: Use of Radiofrequency Ablation in Benign Thyroid Nodules: A Literature Review and UpdatesDocument8 pagesReview Article: Use of Radiofrequency Ablation in Benign Thyroid Nodules: A Literature Review and Updatesagita kartika sariNo ratings yet
- IJETR022925Document7 pagesIJETR022925erpublicationNo ratings yet
- A Statistical Model For Multidimensional Irreversible Electroporation Cell Death in TissueDocument13 pagesA Statistical Model For Multidimensional Irreversible Electroporation Cell Death in TissueKrishnaveni Subramani SNo ratings yet
- Thermal Effects Associated With RF Exposures Hindawi WileyDocument18 pagesThermal Effects Associated With RF Exposures Hindawi WileymadhusoodhananppNo ratings yet
- Electrosurgical Generators: Technology Status Evaluation ReportDocument12 pagesElectrosurgical Generators: Technology Status Evaluation ReportnmmMJKJNo ratings yet
- (Journal of Neurosurgery) Studies of Electrical Skin Resistance in Peripheral Nerve LesionsDocument8 pages(Journal of Neurosurgery) Studies of Electrical Skin Resistance in Peripheral Nerve LesionsstefneluNo ratings yet
- ' Background Noise ' in ElectromyographyDocument17 pages' Background Noise ' in ElectromyographyNawaf RuwailiNo ratings yet
- Interfacing Bioelectronics and Biomedical SensingFrom EverandInterfacing Bioelectronics and Biomedical SensingHung CaoNo ratings yet
- Drinking Water Parameter Cooperation ProjectDocument240 pagesDrinking Water Parameter Cooperation ProjectramNo ratings yet
- LFDDocument2 pagesLFDDindin Torres100% (1)
- Fact Shett - OSHADocument2 pagesFact Shett - OSHALuiz Rubens Souza CantelliNo ratings yet
- Art Deco AssignmentDocument20 pagesArt Deco AssignmentAmerNo ratings yet
- Drug Study Pharmacology in MidwiferyDocument3 pagesDrug Study Pharmacology in MidwiferyLeander Isabelle NoolNo ratings yet
- Eng QP 6 17 PDFDocument4 pagesEng QP 6 17 PDFAkshar gargNo ratings yet
- GlipizideDocument3 pagesGlipizideapi-3797941100% (1)
- How To Get Appointed Ocn370397207Document46 pagesHow To Get Appointed Ocn370397207api-241896162No ratings yet
- Exploratory EssayDocument3 pagesExploratory Essayapi-251189694No ratings yet
- Accidental Death & Serious Injury Cover ExplainedDocument20 pagesAccidental Death & Serious Injury Cover ExplainedTomato GreenNo ratings yet
- Tests of SignificanceDocument111 pagesTests of SignificanceMeer100% (1)
- 1. !!!prac. СPRDocument55 pages1. !!!prac. СPRtop theNo ratings yet
- PDA Points To Consider For Aseptic ProcessingDocument14 pagesPDA Points To Consider For Aseptic ProcessingKevin ZhaoNo ratings yet
- Hip Alert ProcessDocument1 pageHip Alert Processapi-264494543No ratings yet
- Amflagrankchinances 1Document11 pagesAmflagrankchinances 1api-406801987No ratings yet
- Manual de Intrucciones Oximag PDFDocument134 pagesManual de Intrucciones Oximag PDFJose Ivan Carvajal CortizosNo ratings yet
- Jjpaf ApplicationDocument6 pagesJjpaf ApplicationCharles LeeNo ratings yet
- DR Anoop MisraDocument8 pagesDR Anoop MisraAbhishek S AatreyaNo ratings yet
- Neuro4Nurses Cerebellar StrokeDocument2 pagesNeuro4Nurses Cerebellar StrokeAisyahNurjannahNo ratings yet
- CleftlipandpalateDocument134 pagesCleftlipandpalatePARIJAT CHAKRABORTY100% (1)
- NootropicsDocument20 pagesNootropicsĽubomírLuptoAbrmanNo ratings yet
- Assessment of Chronic PainDocument7 pagesAssessment of Chronic PainFranciscoGarciaNo ratings yet
- Internal Medicine Clinical Practice Guidelines 2018 Midyear Review PDFDocument17 pagesInternal Medicine Clinical Practice Guidelines 2018 Midyear Review PDFveerrajuNo ratings yet
- Lplpo Pustu 2020Document21 pagesLplpo Pustu 2020Andi FatmasariNo ratings yet
- Synonyms: 1. Ostitis (DIETRICH) 2. Osteitis (BURRI) 3. Panostitis (KOCHER) 4. Osteomyeloperiostitis (MAGNUS)Document22 pagesSynonyms: 1. Ostitis (DIETRICH) 2. Osteitis (BURRI) 3. Panostitis (KOCHER) 4. Osteomyeloperiostitis (MAGNUS)AnastasiafynnNo ratings yet
- Cymbalta (Duloxetine HCL) Patient Information - Side Effects and Drug Images at RxlistDocument7 pagesCymbalta (Duloxetine HCL) Patient Information - Side Effects and Drug Images at Rxlisteiad-mahmoudNo ratings yet