You might also like
- Mccracken 2009Document8 pagesMccracken 2009Sofyan AndaraNo ratings yet
- Reconsidering Medicine: Reconfiguring the Relationship Between Philosophy of Science And Clinical MedicineFrom EverandReconsidering Medicine: Reconfiguring the Relationship Between Philosophy of Science And Clinical MedicineNo ratings yet
- PRM2022 4203138Document8 pagesPRM2022 4203138sarahNo ratings yet
- Illness Beliefs Among Patients With Chronic Widespread Pain - Associations With Self-Reported Health Status, Anxiety and Depressive Symptoms and Impact of PainDocument10 pagesIllness Beliefs Among Patients With Chronic Widespread Pain - Associations With Self-Reported Health Status, Anxiety and Depressive Symptoms and Impact of Painoh yuniNo ratings yet
- Low Back PainDocument8 pagesLow Back PainRajeev NepalNo ratings yet
- 2016 Article 160Document7 pages2016 Article 160Billy Ch SendukNo ratings yet
- Covic 2003 - Biopsychosocial Model in RADocument8 pagesCovic 2003 - Biopsychosocial Model in RADiego Francesco MacaliNo ratings yet
- Cancer Pain and Psychosocial FactorsDocument17 pagesCancer Pain and Psychosocial Factorsarif 2006No ratings yet
- Temperament Traits and Chronic Pain: The Association of Harm Avoidance and Pain-Related AnxietyDocument8 pagesTemperament Traits and Chronic Pain: The Association of Harm Avoidance and Pain-Related AnxietyHaryaman JustisiaNo ratings yet
- Actcr 1 (3) 14Document8 pagesActcr 1 (3) 14Robinson Trujillo CabanillaNo ratings yet
- s13018-021-02693-yDocument6 pagess13018-021-02693-yluisherrera1490No ratings yet
- Springer The ArticleDocument6 pagesSpringer The ArticleAnastasiaNo ratings yet
- A Prospective Cohort Study of Arm Pain in Primary Care and Physiotherapy-Prognostic DeterminantsDocument8 pagesA Prospective Cohort Study of Arm Pain in Primary Care and Physiotherapy-Prognostic DeterminantsFirdaus Septhy ArdhyanNo ratings yet
- Becker, 1997Document8 pagesBecker, 1997DijuNo ratings yet
- IndiacLBP PapaerDocument6 pagesIndiacLBP Papaercvissa1964No ratings yet
- Postural Awareness and Its Relation To Pain ValidaDocument11 pagesPostural Awareness and Its Relation To Pain ValidacderosasNo ratings yet
- Haemophilia Pain Coping QuestionnaireDocument12 pagesHaemophilia Pain Coping QuestionnaireyawnerNo ratings yet
- 2018 Article 2031Document10 pages2018 Article 2031marcelonorisNo ratings yet
- Manual Therapy: Systematic ReviewDocument8 pagesManual Therapy: Systematic Reviewubiktrash1492No ratings yet
- Medicine: The Effectiveness of Acupuncture For Chronic Pain With DepressionDocument6 pagesMedicine: The Effectiveness of Acupuncture For Chronic Pain With DepressionRatrika SariNo ratings yet
- A Randomized Controlled Neuroimaging Trial of Cognitive Behavioral Therapy ForDocument11 pagesA Randomized Controlled Neuroimaging Trial of Cognitive Behavioral Therapy ForSilvio LimaNo ratings yet
- Pny287 PDFDocument12 pagesPny287 PDFValentina lopezNo ratings yet
- PCS en InglesDocument23 pagesPCS en InglesClaudia Tatiana Zuñiga JimenezNo ratings yet
- Role of Kinesiophobia On Pain, Disability and Quality LUQUEDocument44 pagesRole of Kinesiophobia On Pain, Disability and Quality LUQUECelia CaballeroNo ratings yet
- Journal of Psychosomatic Research: Asish Subedi, Krishna Pokharel, Birendra Prasad Sah, Pashupati ChaudharyDocument6 pagesJournal of Psychosomatic Research: Asish Subedi, Krishna Pokharel, Birendra Prasad Sah, Pashupati Chaudharynermal93No ratings yet
- Asesemen PsikoDocument5 pagesAsesemen PsikofajarNo ratings yet
- Ahn 2012Document6 pagesAhn 2012Anonymous gMLTpER9IUNo ratings yet
- Low Back Pain A Comprehensive Review Pathophysiology 2019Document10 pagesLow Back Pain A Comprehensive Review Pathophysiology 2019Victor Andrés Olivares IbarraNo ratings yet
- Kraaimaat 2003Document21 pagesKraaimaat 2003tanviNo ratings yet
- JournalPsyhosomaticResearch-The Role of Emotion Regulation in Chronic Pain, 2018Document9 pagesJournalPsyhosomaticResearch-The Role of Emotion Regulation in Chronic Pain, 2018cj_catalinaNo ratings yet
- Cancer-Related Fatigue: A Systematic and Meta-Analytic Review of Non-Pharmacological Therapies For Cancer PatientsDocument43 pagesCancer-Related Fatigue: A Systematic and Meta-Analytic Review of Non-Pharmacological Therapies For Cancer Patientsjohn chinNo ratings yet
- Validation of The Hospital Anxiety and Depression Scale in Patients With Acute Low Back PainDocument10 pagesValidation of The Hospital Anxiety and Depression Scale in Patients With Acute Low Back PainJihanMukhtarNo ratings yet
- The Pain Anxiety Symptoms Scale - Development and Validation of A Scale To Measure Fear of PainDocument7 pagesThe Pain Anxiety Symptoms Scale - Development and Validation of A Scale To Measure Fear of Painapi-291366747No ratings yet
- Improvement in Anxiety and Pain After Whole Body Whirlpool Hydrotherapy Among Patients With Myofascial Pain SyndromeDocument8 pagesImprovement in Anxiety and Pain After Whole Body Whirlpool Hydrotherapy Among Patients With Myofascial Pain Syndromephysicallen1791No ratings yet
- Hae Feli 2005Document8 pagesHae Feli 2005malikrezaNo ratings yet
- Sensibilidad Cambio Clinico Instrumentos Generales Especificos Dolor CronicoDocument8 pagesSensibilidad Cambio Clinico Instrumentos Generales Especificos Dolor CronicovitorperonaNo ratings yet
- 01 Ajp 0000210912 95664 53Document8 pages01 Ajp 0000210912 95664 53HEMACHANDRAN GNo ratings yet
- The Tangled Mechanics of Pain in Complementary Medicine: By: Christopher K. Gaffney, PH.D., FAAAPDocument3 pagesThe Tangled Mechanics of Pain in Complementary Medicine: By: Christopher K. Gaffney, PH.D., FAAAPckgaffneyNo ratings yet
- Mahnig 2016Document7 pagesMahnig 2016Ayat BissNo ratings yet
- Kelompok A - Tugas Blok Akupuntur - Critical AppraisalDocument23 pagesKelompok A - Tugas Blok Akupuntur - Critical AppraisalRz FbNo ratings yet
- Research: The Prognosis of Acute and Persistent Low-Back Pain: A Meta-AnalysisDocument12 pagesResearch: The Prognosis of Acute and Persistent Low-Back Pain: A Meta-AnalysisDeivison Fellipe da Silva CâmaraNo ratings yet
- Pain Assessment Tool in The Critically Ill Post-Open Heart Surgery Patient PopulationDocument27 pagesPain Assessment Tool in The Critically Ill Post-Open Heart Surgery Patient PopulationjheighreinNo ratings yet
- Magnetic in Pelvic PainDocument16 pagesMagnetic in Pelvic PainNakarit SangsirinawinNo ratings yet
- Pain Practice - 2023 - YoonDocument14 pagesPain Practice - 2023 - YoonAbbey WaltzNo ratings yet
- Clinical Model For Pattern Recognition in Pain AssessmentDocument8 pagesClinical Model For Pattern Recognition in Pain AssessmentSteffani PinheiroNo ratings yet
- 2.chronicback PainDocument9 pages2.chronicback PainRiantiara PutrizaNo ratings yet
- Psychological Aspects of Persistent Pain Current State of The ScienceDocument17 pagesPsychological Aspects of Persistent Pain Current State of The Scienceraquelalcides1412No ratings yet
- Brief and Distinct Empirical Sleepiness and Fatigue Scales 2006Document9 pagesBrief and Distinct Empirical Sleepiness and Fatigue Scales 2006twice againNo ratings yet
- Pscyhiatry and Pain ManagementDocument8 pagesPscyhiatry and Pain ManagementYudith LouisaNo ratings yet
- Disability and Related Factors in Patients With Chronic Cervical Myofascial PainDocument8 pagesDisability and Related Factors in Patients With Chronic Cervical Myofascial Painaria tristayanthiNo ratings yet
- Seminars in Arthritis and RheumatismDocument9 pagesSeminars in Arthritis and Rheumatismkaren ceballosNo ratings yet
- Skala NyeriDocument20 pagesSkala NyeripuspaNo ratings yet
- ArticolDocument11 pagesArticolIepureNo ratings yet
- Texto Exercício aeróbico saúde mental uma revisão sistemática e meta-análise.Document15 pagesTexto Exercício aeróbico saúde mental uma revisão sistemática e meta-análise.canaldasprofissoesNo ratings yet
- VVs de Valoración y Estrategias de Afrontamiento en La Predicción de La Ans y La Depr en Dolor CrónicoDocument9 pagesVVs de Valoración y Estrategias de Afrontamiento en La Predicción de La Ans y La Depr en Dolor CrónicoAzucenaNo ratings yet
- Criteria for Complicated Grief Disorder DiagnosisDocument9 pagesCriteria for Complicated Grief Disorder DiagnosisAlexandra OanaNo ratings yet
- PAIN® Volume 36 Issue 3 1989 (Doi 10.1016 - 0304-3959 (89) 90095-X) Williams, David A. Thorn, Beverly E. - An Empirical Assessment of Pain Beliefs PDFDocument8 pagesPAIN® Volume 36 Issue 3 1989 (Doi 10.1016 - 0304-3959 (89) 90095-X) Williams, David A. Thorn, Beverly E. - An Empirical Assessment of Pain Beliefs PDFUmmuSallamahNo ratings yet
- Prevalence of Depression and Anxiety in SLE PDFDocument14 pagesPrevalence of Depression and Anxiety in SLE PDFRidho PratamaNo ratings yet
- TENS Literature - Review - and - Meta - Analysis - Of.99266Document9 pagesTENS Literature - Review - and - Meta - Analysis - Of.99266Adam ForshawNo ratings yet
- De Quervain DiseaseDocument4 pagesDe Quervain DiseaseDita MayasariNo ratings yet
- Ms Problem in Iranian Hand-Woven Shoe-Sole Making Operation N Developing Guideline For Work Station DesignDocument11 pagesMs Problem in Iranian Hand-Woven Shoe-Sole Making Operation N Developing Guideline For Work Station DesignDita MayasariNo ratings yet
- Hubungan Tingkat Risiko Ergonomi dan Beban Angkut Terhadap Keluhan Musculoskeletal Disorders (MSDs) pada Pabrik Pemotongan Kayu X Mranggen, DemakDocument8 pagesHubungan Tingkat Risiko Ergonomi dan Beban Angkut Terhadap Keluhan Musculoskeletal Disorders (MSDs) pada Pabrik Pemotongan Kayu X Mranggen, DemakDita MayasariNo ratings yet
- Discomfort, Fatigue, and Work Related MSD Associated With Prolonged Standing Among Malaysian Manufacturing WorkerDocument5 pagesDiscomfort, Fatigue, and Work Related MSD Associated With Prolonged Standing Among Malaysian Manufacturing WorkerDita MayasariNo ratings yet
- Ergonomic Evaluation of Risk Factor For MSD in Construction WorkerDocument7 pagesErgonomic Evaluation of Risk Factor For MSD in Construction WorkerDita MayasariNo ratings yet
- 301-Article Text-1577-1-10-20221108Document7 pages301-Article Text-1577-1-10-20221108Dita MayasariNo ratings yet
- The Effect of Muskuloskeletal Problem On Fatigue and Productivity of Office PersonelDocument7 pagesThe Effect of Muskuloskeletal Problem On Fatigue and Productivity of Office PersonelDita MayasariNo ratings yet
- Conduct Disorder and Somatic Health in ChildrenDocument3 pagesConduct Disorder and Somatic Health in ChildrenJeric C. ManaliliNo ratings yet
- Causes and Treatment of Respiratory and Metabolic Acidosis and AlkalosisDocument4 pagesCauses and Treatment of Respiratory and Metabolic Acidosis and AlkalosisKristie Stiles100% (1)
- Halaman Peserta - CBT Online AILA LMSDocument1 pageHalaman Peserta - CBT Online AILA LMSAisyah Salsabilah11No ratings yet
- S H Z P R N A: Colegio de Sta. Lourdes of Leyte Foundation, Inc. College of Nursing Tabontabon, LeyteDocument74 pagesS H Z P R N A: Colegio de Sta. Lourdes of Leyte Foundation, Inc. College of Nursing Tabontabon, LeyteGlenn ChavezNo ratings yet
- Sleep Study Test: PSG Summary ReportDocument12 pagesSleep Study Test: PSG Summary Reportkuwar palNo ratings yet
- IMAGINE+Caregiver+Program SSA+Document59 pagesIMAGINE+Caregiver+Program SSA+Nikola VeleskiNo ratings yet
- 63yo Professor Stroke Weakness Slurred SpeechDocument2 pages63yo Professor Stroke Weakness Slurred SpeechKoleen Lhyte T. UYNo ratings yet
- Specific Language Impairment (SLI) (The Term Developmental Language Disorder Is Preferred byDocument2 pagesSpecific Language Impairment (SLI) (The Term Developmental Language Disorder Is Preferred byGrim ReaperNo ratings yet
- ATLS Pre-Test (With Front Page)Document10 pagesATLS Pre-Test (With Front Page)Nourah A.Al Moqbel100% (2)
- DR Ty BLS PALS1Document4 pagesDR Ty BLS PALS1Burt Robinson LayosNo ratings yet
- Role of Gluten in Canine Epileptoid Cramping SyndromeDocument7 pagesRole of Gluten in Canine Epileptoid Cramping Syndromemira.hertteliNo ratings yet
- Old Age Psychiatry LectureDocument38 pagesOld Age Psychiatry LectureMo 'Fishpondz' IsmailNo ratings yet
- Genetic Diseases in the Philippines: Down SyndromeDocument4 pagesGenetic Diseases in the Philippines: Down SyndromeGracy JavierNo ratings yet
- Infantile, Childhood, and Adolescent Epilepsies.9Document34 pagesInfantile, Childhood, and Adolescent Epilepsies.9Silviana IlieNo ratings yet
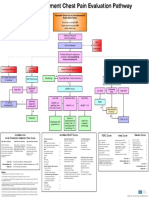
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidNo ratings yet
- Sleep TestingDocument1 pageSleep TestingTroy O'BrienNo ratings yet
- Febrile Seizures NCPDocument9 pagesFebrile Seizures NCPNurul IrhamnaNo ratings yet
- Psychopathology Assignment 2Document3 pagesPsychopathology Assignment 2Hooria AmerNo ratings yet
- OtosclerosisDocument10 pagesOtosclerosisdagne harmanNo ratings yet
- Jurnal AsliDocument10 pagesJurnal AsliNurulwidia SariNo ratings yet
- Hypothermia Alcohol Related IllnessDocument42 pagesHypothermia Alcohol Related IllnessSritharan GaneshamoorthyNo ratings yet
- Fieldwork Report-8Document12 pagesFieldwork Report-8vrindaNo ratings yet
- Diagnostic and Statistical Manual of Mental Disorders: Distinction From ICD Pre-DSM-1 (1840-1949)Document25 pagesDiagnostic and Statistical Manual of Mental Disorders: Distinction From ICD Pre-DSM-1 (1840-1949)Unggul YudhaNo ratings yet
- Paper PPT Edited 20.4Document24 pagesPaper PPT Edited 20.4shruti kumarNo ratings yet
- Notes On MigraineDocument18 pagesNotes On MigraineSaleh Mohammad ShoaibNo ratings yet
- Treating PTSD in the Middle EastDocument4 pagesTreating PTSD in the Middle Eastsyeda salmaNo ratings yet
- Iugr & IufdDocument25 pagesIugr & IufdÅbübâkêř Äbd-ëřhēēm BãřřîNo ratings yet
- WeCareJourney Edmund LimDocument12 pagesWeCareJourney Edmund LimPrabhuNo ratings yet
- Scoring Instructions For NICHQ Vanderbilt Assessment ScalesDocument2 pagesScoring Instructions For NICHQ Vanderbilt Assessment ScalesNet PrepNo ratings yet
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (249)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationFrom EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationRating: 5 out of 5 stars5/5 (9)
- Embrace Your Weird: Face Your Fears and Unleash CreativityFrom EverandEmbrace Your Weird: Face Your Fears and Unleash CreativityRating: 4.5 out of 5 stars4.5/5 (124)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouFrom EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNo ratings yet
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (558)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsFrom EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsRating: 4.5 out of 5 stars4.5/5 (48)
- Vagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerFrom EverandVagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerRating: 4.5 out of 5 stars4.5/5 (16)
- The Anatomy of Loneliness: How to Find Your Way Back to ConnectionFrom EverandThe Anatomy of Loneliness: How to Find Your Way Back to ConnectionRating: 4.5 out of 5 stars4.5/5 (162)
- The Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.From EverandThe Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.Rating: 5 out of 5 stars5/5 (14)
- Triggers: How We Can Stop Reacting and Start HealingFrom EverandTriggers: How We Can Stop Reacting and Start HealingRating: 5 out of 5 stars5/5 (58)