You might also like
- Techniques of Body MechanicsDocument11 pagesTechniques of Body MechanicsJazelyn Mae UyNo ratings yet
- Funda Rle Bed MakingDocument4 pagesFunda Rle Bed MakingIvan MaximusNo ratings yet
- Treatment of The Mentally IllDocument8 pagesTreatment of The Mentally IllAchilles Ybarra100% (1)
- NCM 116 Lab Midterm ActivityDocument2 pagesNCM 116 Lab Midterm ActivityEula Dannah Alyssha EboraNo ratings yet
- Fracture (Cast Care)Document6 pagesFracture (Cast Care)Vane UcatNo ratings yet
- Psychia 03 30Document21 pagesPsychia 03 30allkhusairy6tuansiNo ratings yet
- A Case Study: Region 2 University of La Salette, Inc. Santiago City, IsabelaDocument11 pagesA Case Study: Region 2 University of La Salette, Inc. Santiago City, IsabelaronronNo ratings yet
- Hand Hygiene: Alcohol Based Hand RubDocument2 pagesHand Hygiene: Alcohol Based Hand RubKIERSTINE MARIE BARCELONo ratings yet
- NCM 109 Skills ChecklistDocument8 pagesNCM 109 Skills ChecklistReygine CariñoNo ratings yet
- Pulmo and CardioDocument60 pagesPulmo and CardioNevea CariñoNo ratings yet
- Nasogastric (NG) Tube Insertion Checklist: Lab Clin Clin Tasks Attempted 1 2 3 4 5 6 7Document5 pagesNasogastric (NG) Tube Insertion Checklist: Lab Clin Clin Tasks Attempted 1 2 3 4 5 6 7Richard PattersonNo ratings yet
- HA-RLE-WS # 5 Assessing General Status and Vital SignsDocument5 pagesHA-RLE-WS # 5 Assessing General Status and Vital SignsJULIE ANNE CORTEZ100% (1)
- Er 1Document8 pagesEr 1Justin HannahNo ratings yet
- Gi NclexDocument8 pagesGi NclexDerek Scott Tripp67% (3)
- Pedia Nursing Lecture on Growth and DevelopmentDocument59 pagesPedia Nursing Lecture on Growth and Developmentshenric16100% (1)
- Nle 3Document6 pagesNle 3Aijem RyanNo ratings yet
- Assessment of Breast and Lymphatic SystemDocument4 pagesAssessment of Breast and Lymphatic Systemclyde i amNo ratings yet
- Chapter 36 Skin Integrity and Wound CareDocument7 pagesChapter 36 Skin Integrity and Wound CareKathleen FrugalidadNo ratings yet
- PRE MS N2016 Ans KeyDocument33 pagesPRE MS N2016 Ans Keyaaron tabernaNo ratings yet
- Quiz MidtermDocument4 pagesQuiz MidtermAnonymous uosYCyXNo ratings yet
- Psychiatric Nursing Drills for Child Abuse VictimsDocument7 pagesPsychiatric Nursing Drills for Child Abuse Victimsstoto_arenNo ratings yet
- MCN Book ProjectDocument74 pagesMCN Book ProjectRonnie De Vera IINo ratings yet
- Bandage and Sling Guide for Wound CareDocument47 pagesBandage and Sling Guide for Wound Careriza sarmientoNo ratings yet
- A. Matching Type: M: Atch The Terms in The Left Column With The Correct Descriptions in The Right ColumnDocument9 pagesA. Matching Type: M: Atch The Terms in The Left Column With The Correct Descriptions in The Right ColumnCzarina Mae Quinones TadeoNo ratings yet
- Emergency Cardiac Medications for ArrhythmiasDocument14 pagesEmergency Cardiac Medications for ArrhythmiasRomzy BasañesNo ratings yet
- December2012nletips Funda 121005040112 Phpapp02 PDFDocument6 pagesDecember2012nletips Funda 121005040112 Phpapp02 PDFJessamine Rochelle Reyes EsbertoNo ratings yet
- CIP-NCM-121-Disaster Nursing-TuesdaysDocument3 pagesCIP-NCM-121-Disaster Nursing-TuesdaysKhen QuiringNo ratings yet
- Inbound 4624314230825210461Document58 pagesInbound 4624314230825210461Roy AmataNo ratings yet
- NCM103 - 2016 - Lecture2 - Response To Altered Respiratory FunctionDocument128 pagesNCM103 - 2016 - Lecture2 - Response To Altered Respiratory FunctionrimeoznekNo ratings yet
- NLE2Document10 pagesNLE2giansulakisosuNo ratings yet
- Body Mechanics ChecklistDocument7 pagesBody Mechanics ChecklistPrincess ZantuaNo ratings yet
- Donning of Personal Protective Equipment (PPE) Procedure ChecklistDocument3 pagesDonning of Personal Protective Equipment (PPE) Procedure ChecklistMonicaElizadePazNo ratings yet
- Types of LeadershipDocument13 pagesTypes of LeadershipMary Roan RonatoNo ratings yet
- Medical Surgical Nursing QuestionsDocument7 pagesMedical Surgical Nursing Questionseloisa mae gementizaNo ratings yet
- ExamDocument8 pagesExamcirujales100% (1)
- P2 Long Exam A 15 Block 3 Funda Lecture PDFDocument25 pagesP2 Long Exam A 15 Block 3 Funda Lecture PDFryllerylle05No ratings yet
- Health AssessmentDocument51 pagesHealth AssessmentJared Dela cruzNo ratings yet
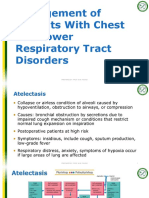
- Management of Chest and Lower Respiratory DisordersDocument32 pagesManagement of Chest and Lower Respiratory DisordersSam GarciaNo ratings yet
- MCI Mass Casualty IncidentDocument32 pagesMCI Mass Casualty Incidenttanya merdeNo ratings yet
- Funda Saved Ms2003Document103 pagesFunda Saved Ms2003June DumdumayaNo ratings yet
- 1Document3 pages1zhandygurlNo ratings yet
- Important Estimates in Pregnancy & Danger Signs in Pregnancy PDFDocument3 pagesImportant Estimates in Pregnancy & Danger Signs in Pregnancy PDFTandingco, Olivia Mari H.No ratings yet
- ) Administering Nasogastric Tube or Orogastric Tube FeedingDocument6 pages) Administering Nasogastric Tube or Orogastric Tube FeedingJohn Pearl FernandezNo ratings yet
- DR Notes at Benguet General HospitalDocument1 pageDR Notes at Benguet General HospitalTeanu Jose Gabrillo TamayoNo ratings yet
- Orthopedic NursingDocument2 pagesOrthopedic NursingMichelle TamorNo ratings yet
- Drainage normal after sigmoid colostomyDocument35 pagesDrainage normal after sigmoid colostomyJackie AbarraNo ratings yet
- Skeletal System ReviewerDocument4 pagesSkeletal System ReviewerMadelle Capending DebutonNo ratings yet
- St. Augustine Foundation Colleges Fundamentals of Caregiving SkillsDocument3 pagesSt. Augustine Foundation Colleges Fundamentals of Caregiving Skillsycofel07No ratings yet
- NCM 112 - Rle Skills Lab Performance Checklist Obtaining An ElectrocardiogramDocument3 pagesNCM 112 - Rle Skills Lab Performance Checklist Obtaining An ElectrocardiogramDominicManlutacNo ratings yet
- TAHBSO Procedure ExplainedDocument14 pagesTAHBSO Procedure ExplainedDafny CzarinaNo ratings yet
- Key Areas OF Responsibility: Core Competencies and IndicatorsDocument12 pagesKey Areas OF Responsibility: Core Competencies and Indicatorschristine_bayonaNo ratings yet
- RE Operative ARE: 06 September 2010 Perioperative Nursing Elvira LimDocument4 pagesRE Operative ARE: 06 September 2010 Perioperative Nursing Elvira LimCaren ReyesNo ratings yet
- Geria Lec Portfolio CasiaDocument9 pagesGeria Lec Portfolio CasiaMarie Ashley CasiaNo ratings yet
- Disaster Response GuidelinesDocument39 pagesDisaster Response GuidelinesNELSON NISPEROSNo ratings yet
- FUNDA Lab 11 Oxygen Therapy Suctioning Procedures23Document38 pagesFUNDA Lab 11 Oxygen Therapy Suctioning Procedures23loijhonmuchillasNo ratings yet
- Clinical Practicum 100.Pptx11Document24 pagesClinical Practicum 100.Pptx11krezelflores2No ratings yet
- Checklists For Transfer and AmbulationDocument15 pagesChecklists For Transfer and Ambulationmido100% (1)
- NCM Lab Checklist - PositioningDocument2 pagesNCM Lab Checklist - PositioningYanna Habib-MangotaraNo ratings yet
- Transfer IngDocument5 pagesTransfer IngCherrie FayeNo ratings yet
- Patient Transfer ChecklistDocument5 pagesPatient Transfer ChecklistraedaosamaNo ratings yet
- Leadership Roles and Responsibilities of A Nurse in Disaster Risk and Reduction ManagementDocument13 pagesLeadership Roles and Responsibilities of A Nurse in Disaster Risk and Reduction ManagementIrish Jane GalloNo ratings yet
- Annex B - Health Declaration FormNov2020Document4 pagesAnnex B - Health Declaration FormNov2020jhade_cabatoNo ratings yet
- ENDOCRINE SYSTEM Handouts For IloiloDocument19 pagesENDOCRINE SYSTEM Handouts For Iloilodelieup02No ratings yet
- PostDocument2 pagesPostIrish Jane GalloNo ratings yet
- Cardiac Study GuideDocument9 pagesCardiac Study GuideJane DiazNo ratings yet
- Maternal and Child Nursing Care EssentialsDocument12 pagesMaternal and Child Nursing Care EssentialsIrish Jane GalloNo ratings yet
- Alas Singko English Storybook - Coloring Book VersionDocument15 pagesAlas Singko English Storybook - Coloring Book VersionIrish Jane GalloNo ratings yet
- Liver DisordersDocument2 pagesLiver DisordersIrish Jane GalloNo ratings yet
- CRP Level 4 1ST Sem Ay 2022 2023Document1 pageCRP Level 4 1ST Sem Ay 2022 2023Irish Jane GalloNo ratings yet
- Attachment 1Document2 pagesAttachment 1Irish Jane GalloNo ratings yet
- Dialogue 2 Where Is The BankDocument2 pagesDialogue 2 Where Is The BankIrish Jane GalloNo ratings yet
- Intro To LogicDocument34 pagesIntro To LogicIrish Jane GalloNo ratings yet
- Submitted By: Russel Mark A. Plaida: Health Optimizing Physical Education H.O.P.E 1 Quarter 1Document10 pagesSubmitted By: Russel Mark A. Plaida: Health Optimizing Physical Education H.O.P.E 1 Quarter 1Irish Jane GalloNo ratings yet
- Acad - Writing Position PaperDocument11 pagesAcad - Writing Position PaperIrish Jane GalloNo ratings yet
- Attachment 1Document2 pagesAttachment 1Irish Jane GalloNo ratings yet
- Yellow Paper of Russel MarkDocument5 pagesYellow Paper of Russel MarkIrish Jane GalloNo ratings yet
- Case Simulation 3 - Respiratory ProblemDocument3 pagesCase Simulation 3 - Respiratory ProblemIrish Jane GalloNo ratings yet
- Yellow Paper of Russel MarkDocument5 pagesYellow Paper of Russel MarkIrish Jane GalloNo ratings yet
- Yellow Paper of Russel MarkDocument5 pagesYellow Paper of Russel MarkIrish Jane GalloNo ratings yet
- Quiz (4 Mei - 7 Mei)Document3 pagesQuiz (4 Mei - 7 Mei)NdyNo ratings yet
- Annexure 42 - Counselling Checklists-NewDocument18 pagesAnnexure 42 - Counselling Checklists-NewJay PaulNo ratings yet
- Module 5-Safety and Health at Work - MANUALDocument46 pagesModule 5-Safety and Health at Work - MANUALYhan Brotamonte BoneoNo ratings yet
- List of Adjective Appearance Adjectives Time AdjectivesDocument6 pagesList of Adjective Appearance Adjectives Time AdjectivesSitiNurul JannahNo ratings yet
- Vaccine Immune Interactions and Booster Shots Sep 2021Document11 pagesVaccine Immune Interactions and Booster Shots Sep 2021Les BennettNo ratings yet
- Common ColdDocument6 pagesCommon ColdChastin Perias0% (1)
- Psoriatic Arthritis Nature ReviewDocument17 pagesPsoriatic Arthritis Nature ReviewJose Shaid Delgado OlveraNo ratings yet
- Bartholin Gland Marsupialization - Overview, Periprocedural Care, Overview of TechniqueDocument6 pagesBartholin Gland Marsupialization - Overview, Periprocedural Care, Overview of TechniqueZega AgustianNo ratings yet
- Final Literature Review-Antineoplastic AgentsDocument5 pagesFinal Literature Review-Antineoplastic Agentsapi-703108884No ratings yet
- Dengue Hero-PcpDocument27 pagesDengue Hero-PcpRomina Mae FajardoNo ratings yet
- THE GALLUP ORGANIZATION For The American Board of Internal MedicineDocument38 pagesTHE GALLUP ORGANIZATION For The American Board of Internal MedicineabimorgNo ratings yet
- Precipitous LaborDocument7 pagesPrecipitous Labornursereview100% (4)
- AMS Clinical PathwayDocument88 pagesAMS Clinical Pathwayraitosan1412No ratings yet
- BluePrint 5th QuestionsDocument25 pagesBluePrint 5th QuestionsAbuFreihNo ratings yet
- Data Ruangan Intensive (071020)Document31 pagesData Ruangan Intensive (071020)Andrew WarankiranNo ratings yet
- Open Letter To Mayor-Elect Wu - Mass and CassDocument2 pagesOpen Letter To Mayor-Elect Wu - Mass and Cassdialynn dwyerNo ratings yet
- Bahasa Inggris KeperawatanDocument7 pagesBahasa Inggris KeperawatanGeldine Raudina25No ratings yet
- Obstetrical Nursing NotesDocument25 pagesObstetrical Nursing NotesFreeNursingNotes81% (16)
- Profil Skabies Di Poliklinik Kulit Dan Kelamin RSUD Dr. H. Andi Abdurrahman Noor Periode Januari-Desember 2021 (Jurnal)Document7 pagesProfil Skabies Di Poliklinik Kulit Dan Kelamin RSUD Dr. H. Andi Abdurrahman Noor Periode Januari-Desember 2021 (Jurnal)Klinik Pratama Ar-Raudhah 129No ratings yet
- Stroke Rehabilitation: Therapy Stroke Rehabilitation: TherapyDocument12 pagesStroke Rehabilitation: Therapy Stroke Rehabilitation: TherapyKripa MathaiNo ratings yet
- Pathology Lab GuidelinesDocument68 pagesPathology Lab GuidelinesLUZVIMINDA GORDO100% (1)
- Medical Device Classification GuideDocument30 pagesMedical Device Classification GuideAriska Oktavera 26No ratings yet
- DownloadfilesDocument26 pagesDownloadfilesDowntoearthNo ratings yet
- Benefits of A Food Supplement Containing Boswellia Serrata and Bromelain For Improving The Quality of Life in Patients With Osteoarthritis: A Pilot Study - 2019Document7 pagesBenefits of A Food Supplement Containing Boswellia Serrata and Bromelain For Improving The Quality of Life in Patients With Osteoarthritis: A Pilot Study - 2019ranasoftNo ratings yet
- Nursing Care Plan DMDocument8 pagesNursing Care Plan DMnikaaraaaNo ratings yet
- NLE RDocument51 pagesNLE RmariaNo ratings yet
- The Big Family Day OutDocument2 pagesThe Big Family Day OutPlimmerton Residents' AssociationNo ratings yet
- Global Assessment (PG-SGA) : Scored Patient-Generated SubjectiveDocument1 pageGlobal Assessment (PG-SGA) : Scored Patient-Generated SubjectiveSafira Ridha UlyaNo ratings yet
- Hepatitis C VirusDocument16 pagesHepatitis C Virusمصطفى رسول هاديNo ratings yet
- Allocation of Health Care ResourceDocument2 pagesAllocation of Health Care ResourceSha Btsta100% (1)