You might also like
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- S1P3G3 IgnacioDocument8 pagesS1P3G3 IgnacioJose Mari S IgnacioNo ratings yet
- SANDIGAN - Case #1 AY21-22 - 2nd SemDocument9 pagesSANDIGAN - Case #1 AY21-22 - 2nd SemHazelle Joyce SandiganNo ratings yet
- S1P4G3 IgnacioDocument10 pagesS1P4G3 IgnacioJose Mari S IgnacioNo ratings yet
- Pedia HST TemplateDocument9 pagesPedia HST TemplateRyan Loyd MarquezNo ratings yet
- S1P5G3 IgnacioDocument14 pagesS1P5G3 IgnacioJose Mari S IgnacioNo ratings yet
- S1P6G3 IgnacioDocument11 pagesS1P6G3 IgnacioJose Mari S IgnacioNo ratings yet
- NDR 325 (Provider of Care I: Adult & Elder Health) : Case Study PresentationDocument14 pagesNDR 325 (Provider of Care I: Adult & Elder Health) : Case Study PresentationR GhNo ratings yet
- Neurology Clinical History FormDocument2 pagesNeurology Clinical History FormZainab JawadNo ratings yet
- Medical History FormDocument4 pagesMedical History FormevalinadrNo ratings yet
- Clinical Evaluation - Pediatrics: General DataDocument2 pagesClinical Evaluation - Pediatrics: General DataColeen VergaraNo ratings yet
- Patient Intake Form DFC1Document2 pagesPatient Intake Form DFC125111980No ratings yet
- Case Study Presentation - Nephrotic SyndromeDocument56 pagesCase Study Presentation - Nephrotic SyndromeVivien Marie89% (27)
- Fibromyalgia Journal Appendix A - Additional SymptomsDocument1 pageFibromyalgia Journal Appendix A - Additional SymptomslauramariegonzalezNo ratings yet
- Medical Examination Form 2022-2023Document5 pagesMedical Examination Form 2022-2023Linh ĐặngNo ratings yet
- Pediatric History Taking EditDocument6 pagesPediatric History Taking EditWayNo ratings yet
- Case ReportDocument16 pagesCase ReportMonique BorresNo ratings yet
- Konfrens RS Stella Maris 6092022Document21 pagesKonfrens RS Stella Maris 6092022Maya Rosmaria PNo ratings yet
- Nephrotic SyndromeDocument56 pagesNephrotic SyndromeMurugesan100% (1)
- Case Analysis I. Case Diagnosis: Left-Sided Heart Failure II. Medical History: Patient's ProfileDocument3 pagesCase Analysis I. Case Diagnosis: Left-Sided Heart Failure II. Medical History: Patient's ProfileGuile RilleraNo ratings yet
- Hospital Claim - Template24 - Page4Document1 pageHospital Claim - Template24 - Page4chamuditha dilshanNo ratings yet
- POMER - Dengue Case PresentationDocument53 pagesPOMER - Dengue Case Presentationdenzel0711No ratings yet
- Grand Rounds Meningitis Oct 2021Document94 pagesGrand Rounds Meningitis Oct 2021jake estacaNo ratings yet
- Ward 1: Group 4: Paras, Payad, Pedrosa, Pinlac, Roldan, SalungaDocument30 pagesWard 1: Group 4: Paras, Payad, Pedrosa, Pinlac, Roldan, SalungaJoezelleNo ratings yet
- Medicine History and CounsellingDocument13 pagesMedicine History and Counsellingpranjl100% (1)
- Pedia History FormDocument6 pagesPedia History Formwinchloe38No ratings yet
- Peds WW Form1 - 1Document17 pagesPeds WW Form1 - 1Karess AvilloNo ratings yet
- Konfrens RS Stella Maris 6092022-2Document21 pagesKonfrens RS Stella Maris 6092022-2Maya Rosmaria PNo ratings yet
- Cebu Institute of Technology UniversityDocument10 pagesCebu Institute of Technology UniversityDara Sophia EncarguezNo ratings yet
- Sample SOAP NoteDocument6 pagesSample SOAP NoteLorrie83% (6)
- Medical History FormDocument2 pagesMedical History FormNarmin Abubaker AliNo ratings yet
- TB MeningitisDocument91 pagesTB MeningitischristianNo ratings yet
- Case Study QuestionnaireDocument6 pagesCase Study QuestionnaireKim TangoNo ratings yet
- Case 4 Lepto 1 AprilDocument26 pagesCase 4 Lepto 1 AprilCms CSUNo ratings yet
- PONR Assessment ToolDocument9 pagesPONR Assessment ToolNeirfla WassabiNo ratings yet
- Case Series - CapDocument162 pagesCase Series - CapMichael LinebargerNo ratings yet
- January 3 Case PresDocument44 pagesJanuary 3 Case PresKenneth NuñezNo ratings yet
- Healthhistoryform 2018Document2 pagesHealthhistoryform 2018iwasan991No ratings yet
- 4th Medi Pulmo Apr 15 - 17, 2021 QuestionsDocument22 pages4th Medi Pulmo Apr 15 - 17, 2021 QuestionsSheda BondNo ratings yet
- Case Presentation: Group 3-BDocument39 pagesCase Presentation: Group 3-BKenneth NuñezNo ratings yet
- 3B2 Preceptorial Nov 17 - D in PediPatientsDocument59 pages3B2 Preceptorial Nov 17 - D in PediPatientsAbigail PaasaNo ratings yet
- Major Depressive Disorder: Case PresentationDocument34 pagesMajor Depressive Disorder: Case PresentationAbigaille ChuaNo ratings yet
- Medicine: ClinicsDocument80 pagesMedicine: ClinicsDwight AvelinoNo ratings yet
- Cagayan State University College of Medicine Carig Campus, Tuguegarao City Surgery WardDocument7 pagesCagayan State University College of Medicine Carig Campus, Tuguegarao City Surgery WardRishi Du AgbugayNo ratings yet
- Clinical Case: Section A - Group 8Document68 pagesClinical Case: Section A - Group 8madison Deli100% (1)
- Long Case Rama FixDocument13 pagesLong Case Rama FixRamaNo ratings yet
- Smart Sheet For History Taking in SurgeryDocument7 pagesSmart Sheet For History Taking in Surgerymahmoud selimNo ratings yet
- Case Presentation COPDDocument79 pagesCase Presentation COPDmarianne.bilaoen09No ratings yet
- All Forms AdultsDocument13 pagesAll Forms AdultschevypickupNo ratings yet
- Review of Systems FDDocument1 pageReview of Systems FDchronicidalNo ratings yet
- Case Series CapDocument162 pagesCase Series CapDhruva PatelNo ratings yet
- Medical History Form 3 Years and OlderDocument3 pagesMedical History Form 3 Years and OlderJalisha SarmientoNo ratings yet
- Health History 3Document2 pagesHealth History 3boinkjilijoyNo ratings yet
- SOAP - Blank - Template Word Doc 2022Document6 pagesSOAP - Blank - Template Word Doc 2022Joan McutestNo ratings yet
- Colic Abdomen E.C Peritonitis E.C Perforasi Gaster + AKI + Dehidrasi Ringan-SedangDocument22 pagesColic Abdomen E.C Peritonitis E.C Perforasi Gaster + AKI + Dehidrasi Ringan-SedangInesia Putri WulandariNo ratings yet
- Case Presentation - Nephrotic SyndromeDocument52 pagesCase Presentation - Nephrotic Syndromemaryam farrukhNo ratings yet
- Drexel Medicine New Patient Questionnaire 20160504Document7 pagesDrexel Medicine New Patient Questionnaire 20160504Sameer shetyeNo ratings yet
- Pediatric History - TemplateDocument5 pagesPediatric History - TemplateJolaine ValloNo ratings yet
- Case Study Male MSW 1Document27 pagesCase Study Male MSW 1JONAMAY RAMIREZNo ratings yet
- Askep CKD HDDocument21 pagesAskep CKD HDAnjarwidiyonoNo ratings yet
- Applied Augustinian PhilosophyDocument2 pagesApplied Augustinian PhilosophyJose Mari S IgnacioNo ratings yet
- Synthesis About The 6 Pillars of Augustinian Institution and LCUP 6 CORE Values - IgnacioDocument1 pageSynthesis About The 6 Pillars of Augustinian Institution and LCUP 6 CORE Values - IgnacioJose Mari S IgnacioNo ratings yet
- Synthesis About St. Augustine On Love - IgnacioDocument1 pageSynthesis About St. Augustine On Love - IgnacioJose Mari S IgnacioNo ratings yet
- Reflections and Learnings For ST Augustine Search For The Truth-IgnacioDocument1 pageReflections and Learnings For ST Augustine Search For The Truth-IgnacioJose Mari S IgnacioNo ratings yet
- Synthesis About The 6 Pillars of Augustinian Institution and LCUP 6 CORE Values 2 - IgnacioDocument1 pageSynthesis About The 6 Pillars of Augustinian Institution and LCUP 6 CORE Values 2 - IgnacioJose Mari S IgnacioNo ratings yet
- S1P6G3 IgnacioDocument11 pagesS1P6G3 IgnacioJose Mari S IgnacioNo ratings yet
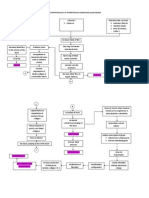
- Pathophysiology of Cerebrovascular AccidentDocument2 pagesPathophysiology of Cerebrovascular AccidentJohn Michael FernandezNo ratings yet
- Postanesthetic Aldrete Recovery Score: Original Criteria Modified Criteria Point ValueDocument3 pagesPostanesthetic Aldrete Recovery Score: Original Criteria Modified Criteria Point ValueBonny ChristianNo ratings yet
- SFEMG Normative DataDocument2 pagesSFEMG Normative DatasisasuNo ratings yet
- Endocrine System NotesDocument6 pagesEndocrine System NotesHannah Grace CorveraNo ratings yet
- Fluid Therapy Pedigree IndiaDocument29 pagesFluid Therapy Pedigree IndiaSantosh BhandariNo ratings yet
- Section 8.1 - Homeostasis: Sbi4U Ms. FranklinDocument15 pagesSection 8.1 - Homeostasis: Sbi4U Ms. FranklinSidemen For LifeNo ratings yet
- 9700 s03 QP 4Document12 pages9700 s03 QP 4Lâm Văn Sa HuỳnhNo ratings yet
- Name: Section: Activity 3 Just Go With The Flow!'Document1 pageName: Section: Activity 3 Just Go With The Flow!'lunaticxNo ratings yet
- Neurohormonal Hypothesis in Heart FailureDocument11 pagesNeurohormonal Hypothesis in Heart FailureCypress Trixia Mananquil MacapagalNo ratings yet
- Q1 Health Status QuestionnaireDocument2 pagesQ1 Health Status QuestionnaireKathleen ChuaNo ratings yet
- Anafi Kayser and Raizen Nature Reviews Neuroscience 2018Document8 pagesAnafi Kayser and Raizen Nature Reviews Neuroscience 2018Francisco MtzNo ratings yet
- Defining Characteristics Nursing Diagnosis Background Knowledge Desired Outcome Nursing Intervention Rationale EvaluationDocument2 pagesDefining Characteristics Nursing Diagnosis Background Knowledge Desired Outcome Nursing Intervention Rationale EvaluationnarsDNo ratings yet
- Clinical Case ScenarioDocument3 pagesClinical Case ScenarioHolly CividinNo ratings yet
- Pathophysiology of Hypertensive Cardiovascular DiseaseDocument3 pagesPathophysiology of Hypertensive Cardiovascular Diseasekhrizaleeh100% (9)
- Montaje Luz Limitador Carga Fassi PDFDocument2 pagesMontaje Luz Limitador Carga Fassi PDFAlfredo Dominguez ArandaNo ratings yet
- Hypovolemic ShockDocument25 pagesHypovolemic ShockManushi HenadeeraNo ratings yet
- Blood and Circulation, iGCSE BiologyDocument4 pagesBlood and Circulation, iGCSE BiologyMisterBlueSky89% (9)
- Solved Problems in Ergonomics 2012Document20 pagesSolved Problems in Ergonomics 2012rianna rose dela cruzNo ratings yet
- Laboratory Exercise - MuscleDocument3 pagesLaboratory Exercise - MuscleJohn Henry G. Gabriel IVNo ratings yet
- Apex - Motor-ReflexesDocument72 pagesApex - Motor-ReflexesDill MuloshiNo ratings yet
- Single Fiber Electromyography: Joze TronteljDocument25 pagesSingle Fiber Electromyography: Joze TronteljRuby Natali Muñoz SalamancaNo ratings yet
- Surgical Complications: Maj. Hafizur Rashid SazalDocument43 pagesSurgical Complications: Maj. Hafizur Rashid SazalHafizur RashidNo ratings yet
- ABCDE Approach - Glasgow Uni OSCEDocument3 pagesABCDE Approach - Glasgow Uni OSCEHaitham Zraigat100% (1)
- Bio Lab Report 2-The Effect of Boiling On The Rate of Aerobic Respiration of Germinating SeedsDocument5 pagesBio Lab Report 2-The Effect of Boiling On The Rate of Aerobic Respiration of Germinating SeedsKingsley Dah Sr.67% (3)
- NCM 112-Mod3Document19 pagesNCM 112-Mod3Samantha BolanteNo ratings yet
- Module in Science 9: First Quarter/Week 1/day4Document5 pagesModule in Science 9: First Quarter/Week 1/day4Frederick EspejoNo ratings yet
- Uworld Notes CK PDFDocument123 pagesUworld Notes CK PDFNik KalairNo ratings yet
- Valvular Heart DiseaseDocument27 pagesValvular Heart DiseaseOwen J. WieseNo ratings yet
- Chapter 21: Introduction To Pharmacology of CNS DrugsDocument19 pagesChapter 21: Introduction To Pharmacology of CNS DrugsJoslin Roz GalileaNo ratings yet
- Arterial Blood GasDocument55 pagesArterial Blood GasRathis Dasan100% (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)