You might also like
- Applications of Robotics For Laryngeal SurgeryDocument11 pagesApplications of Robotics For Laryngeal SurgerySanNo ratings yet
- 2021 2.206 机器人辅助双螺钉固定微小移位的舟骨腰部骨折不愈合或延迟愈合,无需植骨Document6 pages2021 2.206 机器人辅助双螺钉固定微小移位的舟骨腰部骨折不愈合或延迟愈合,无需植骨du jiafeiNo ratings yet
- Interdigital Approach To Trigger Finger Injection Using Ultrasound GuidanceDocument3 pagesInterdigital Approach To Trigger Finger Injection Using Ultrasound GuidanceputriNo ratings yet
- 2016 - Hand Transplantation Versus Hand Prosthetics - Pros and ConsDocument7 pages2016 - Hand Transplantation Versus Hand Prosthetics - Pros and ConsMikiNo ratings yet
- Mechatronics: Umut Mayetin, Serdar KucukDocument17 pagesMechatronics: Umut Mayetin, Serdar Kucukalamin khondakerNo ratings yet
- 2020 A Hybrid, Soft Exoskeleton Glove Equipped With A TelescopicDocument7 pages2020 A Hybrid, Soft Exoskeleton Glove Equipped With A TelescopicANSHUMAAN P BHAGATNo ratings yet
- Robotic Orthosis For Upper Limb Rehabilitation: P EedingsDocument13 pagesRobotic Orthosis For Upper Limb Rehabilitation: P EedingsDaniel TamashiroNo ratings yet
- Muscle Sensor DocumentDocument21 pagesMuscle Sensor Documentvidyadhar GNo ratings yet
- Sensors 21 02927Document16 pagesSensors 21 02927Ashish Presanna ChandranNo ratings yet
- Three-Dimensional Robotic-Assisted Endomicroscopy With A Force Adaptive Robotic ArmDocument6 pagesThree-Dimensional Robotic-Assisted Endomicroscopy With A Force Adaptive Robotic ArmJames BenavidesNo ratings yet
- My SeminarDocument17 pagesMy SeminarRajesh RadhakrishnanNo ratings yet
- Robotic Surgery in Otolaryngology and Head and Neck Surgery: A ReviewDocument12 pagesRobotic Surgery in Otolaryngology and Head and Neck Surgery: A ReviewErick CorputtyNo ratings yet
- Robotics in SurgeryDocument9 pagesRobotics in SurgeryPriyansh AggarwalNo ratings yet
- Bio MechatonicsDocument25 pagesBio MechatonicsSatish HSNo ratings yet
- Hand Extension Robot Orthosis HERO Glove Development and Testing With Stroke Survivors With Severe Hand ImpairmentDocument11 pagesHand Extension Robot Orthosis HERO Glove Development and Testing With Stroke Survivors With Severe Hand ImpairmentMark CagnanNo ratings yet
- Literature Review and Proposed Research: Alba Perez GraciaDocument34 pagesLiterature Review and Proposed Research: Alba Perez GraciaShubha ShriNo ratings yet
- An Actuated Finger Exoskeleton For Hand Rehabilitation Following Stroke 2007Document6 pagesAn Actuated Finger Exoskeleton For Hand Rehabilitation Following Stroke 2007newkid2202No ratings yet
- Validation of A Robotic Testing Procedure For Shoulder in Vitro Biomechanical 9001Document8 pagesValidation of A Robotic Testing Procedure For Shoulder in Vitro Biomechanical 9001Samrat SinghaNo ratings yet
- Life 12 00188Document17 pagesLife 12 00188Ligia BoazuNo ratings yet
- A Hybrid Arm-Hand Rehabilitation Robot With EMG-Based Admittance ControllerDocument11 pagesA Hybrid Arm-Hand Rehabilitation Robot With EMG-Based Admittance ControllerHoney RoseNo ratings yet
- Millers Anesthesia - Sixth Edition - Chapter 66 - Anesthesia For Robotic Surgery - 233Document44 pagesMillers Anesthesia - Sixth Edition - Chapter 66 - Anesthesia For Robotic Surgery - 233Adriana VickNo ratings yet
- EVALUATION OF THE RADIATION DOSE TO THE HANDS OF ORTHOPAEDIC SURGEONS DURING FLUOROSCOPY USING STORED IMAGES (Radiation Protection Dosimetry) (2020)Document6 pagesEVALUATION OF THE RADIATION DOSE TO THE HANDS OF ORTHOPAEDIC SURGEONS DURING FLUOROSCOPY USING STORED IMAGES (Radiation Protection Dosimetry) (2020)Piotr JankowskiNo ratings yet
- Quantitative Diagnosis of Rotator Cuff Tears Based On Sonographic Pattern RecognitionDocument13 pagesQuantitative Diagnosis of Rotator Cuff Tears Based On Sonographic Pattern RecognitionJuwita Valen RamadhanniaNo ratings yet
- Home-Based Rehabilitation For Patients With Spinal Cord InjuryDocument15 pagesHome-Based Rehabilitation For Patients With Spinal Cord InjuryonikabekunNo ratings yet
- A Novel Compliant Surgical Robot-Preliminary Design AnalysisDocument15 pagesA Novel Compliant Surgical Robot-Preliminary Design AnalysisAbhinav D PremNo ratings yet
- Design and Optimization of An Index Finger Exoskeleton With Semi-Wrapped Fixtures and Series Elastic ActuatorsDocument10 pagesDesign and Optimization of An Index Finger Exoskeleton With Semi-Wrapped Fixtures and Series Elastic ActuatorsمحمدNo ratings yet
- 10 1016@j JHT 2020 03 024Document10 pages10 1016@j JHT 2020 03 024eduar yecid duarte gomezNo ratings yet
- Gassert-Dietz2018 Article RehabilitationRobotsForTheTreaDocument15 pagesGassert-Dietz2018 Article RehabilitationRobotsForTheTreaMouyad SrNo ratings yet
- Automation of Upper Limb Prostheses Using Shape Memory AlloysDocument8 pagesAutomation of Upper Limb Prostheses Using Shape Memory AlloysÁSädKHänNo ratings yet
- RoboticSurgery An Evolution in PracticeDocument3 pagesRoboticSurgery An Evolution in PracticeJoão Lourenço0% (1)
- A Bimodal Detection-Based Tremor Suppression System For Vascular Interventional Surgery RobotsDocument13 pagesA Bimodal Detection-Based Tremor Suppression System For Vascular Interventional Surgery RobotsAbdulkareem 99No ratings yet
- Design and Testing of A Soft Parallel Robot Based On Pneumatic Artificial Muscles For Wrist RehabilitationDocument11 pagesDesign and Testing of A Soft Parallel Robot Based On Pneumatic Artificial Muscles For Wrist Rehabilitation王根萌No ratings yet
- Design and Implementation of Upper Limb Rehabilitation Exoskeleton For Post-Stroke Patients - FullDocument6 pagesDesign and Implementation of Upper Limb Rehabilitation Exoskeleton For Post-Stroke Patients - FullTu DuongNo ratings yet
- Cios 13 1Document9 pagesCios 13 1Sugumar NatarajanNo ratings yet
- Oscillator-Based Assistance of Cyclical Movements: Model-Based and Model-Free ApproachesDocument13 pagesOscillator-Based Assistance of Cyclical Movements: Model-Based and Model-Free Approaches李磊No ratings yet
- Conference PaperDocument10 pagesConference PaperYasya Khalif Perdana SalehNo ratings yet
- Anaesthesia For Robotic SurgeryDocument5 pagesAnaesthesia For Robotic Surgerysangamitraachu100% (1)
- Robotic SurgeryDocument11 pagesRobotic SurgerySam AlatawiNo ratings yet
- A Fairly Simple Mechatronic Device For Training Human Wrist MotionDocument15 pagesA Fairly Simple Mechatronic Device For Training Human Wrist Motionalamin khondakerNo ratings yet
- An Attachable Clothing Sensor System For Measuring Knee Joint AnglesDocument8 pagesAn Attachable Clothing Sensor System For Measuring Knee Joint AnglesRoman PopescuNo ratings yet
- The ZEUS Robotic System: Experimental and Clinical ApplicationsDocument11 pagesThe ZEUS Robotic System: Experimental and Clinical ApplicationsademargcjuniorNo ratings yet
- Bjs 9711Document15 pagesBjs 9711Bintang MuslimahNo ratings yet
- Current Techniques in Canine and Feline NeurosurgeryFrom EverandCurrent Techniques in Canine and Feline NeurosurgeryAndy ShoresNo ratings yet
- Liu - Ijos 2017Document11 pagesLiu - Ijos 2017Rohan BhagatNo ratings yet
- Needle Insertion Modelling and SimulationDocument8 pagesNeedle Insertion Modelling and Simulationmohammadreza hajialiNo ratings yet
- 01 Robotic Surgery and TelesurgeryDocument7 pages01 Robotic Surgery and Telesurgerykrishnachaitanya46No ratings yet
- Robotics in Colorectal Surgery: Telemonitoring and TeleroboticsDocument10 pagesRobotics in Colorectal Surgery: Telemonitoring and TeleroboticsprivedNo ratings yet
- A Method For Quantifying Interaction Forces in Wearable RobotsDocument6 pagesA Method For Quantifying Interaction Forces in Wearable RobotsSathvik BhatNo ratings yet
- Design, Development and Implementation of A Biomechanical Right-Hand Prosthesis - Second StageDocument6 pagesDesign, Development and Implementation of A Biomechanical Right-Hand Prosthesis - Second StageTatiana IngaNo ratings yet
- 2018 Article 642Document14 pages2018 Article 642Faqih FathurrozanNo ratings yet
- Active Elbow Orthosis: International Journal of Advanced Robotic Systems August 2014Document11 pagesActive Elbow Orthosis: International Journal of Advanced Robotic Systems August 2014Calugareanu MadalinaNo ratings yet
- Tele Chi Rur GieDocument5 pagesTele Chi Rur GieAlexandraNo ratings yet
- 19554185Document10 pages19554185luckytung07No ratings yet
- Telechirurgie PDFDocument5 pagesTelechirurgie PDFAlexandraNo ratings yet
- Design and Development of A Soft Robotic Gripper For Manipulation in Minimally Invasive Surgery: A Proof of ConceptDocument9 pagesDesign and Development of A Soft Robotic Gripper For Manipulation in Minimally Invasive Surgery: A Proof of ConceptPraveen BhardhwajNo ratings yet
- Touche Chi 2012Document10 pagesTouche Chi 2012Tran Cong HauNo ratings yet
- Haptic Devices Wearability Based Taxonomy and Literature ReviewDocument25 pagesHaptic Devices Wearability Based Taxonomy and Literature ReviewJohn SmithNo ratings yet
- Prosthesis 05 00084 v2Document26 pagesProsthesis 05 00084 v2A MohanNo ratings yet
- Inouye 2013 AnthropomorphicDocument12 pagesInouye 2013 AnthropomorphicAndres RodriguezNo ratings yet
- Bionic Limb ReconstructionFrom EverandBionic Limb ReconstructionOskar C. AszmannNo ratings yet
- Resume - Jonathan Ye 26Document2 pagesResume - Jonathan Ye 26api-576590803No ratings yet
- Using Fmincon As An Optimization Tool For CalibrationsDocument21 pagesUsing Fmincon As An Optimization Tool For Calibrationsapi-576590803No ratings yet
- Using The Global Optimization Toolbox As An Optimization Tool For CalibrationsDocument3 pagesUsing The Global Optimization Toolbox As An Optimization Tool For Calibrationsapi-576590803No ratings yet
- Final ReportDocument21 pagesFinal Reportapi-576590803No ratings yet
- Ec463 Fall 2022 First Semester Report - Group 9Document23 pagesEc463 Fall 2022 First Semester Report - Group 9api-576590803No ratings yet
- Suspension - Shock and Spring 1Document10 pagesSuspension - Shock and Spring 1api-576590803No ratings yet
- Suspension Control Arm Design Report 1Document12 pagesSuspension Control Arm Design Report 1api-576590803No ratings yet
- Me 360 Assignment 2 1Document6 pagesMe 360 Assignment 2 1api-576590803No ratings yet
- Fault Tree AnalysisDocument36 pagesFault Tree AnalysisAMOL RASTOGI 19BCM0012No ratings yet
- Strength Under Fire: Cat Fire Pump EnginesDocument4 pagesStrength Under Fire: Cat Fire Pump EnginesArgenis JimenezNo ratings yet
- 5-The Composite LinkDocument27 pages5-The Composite LinkDr-Ahmed AbdulridhaNo ratings yet
- SLC Twin Rt2 0,7.. 10 kVA: User ManualDocument48 pagesSLC Twin Rt2 0,7.. 10 kVA: User Manualsomae AbbasNo ratings yet
- Ad 114Document4 pagesAd 114Fadzilah NijiNo ratings yet
- Sri Ramakrishna Institute of Technology, Coimbatore-10: Mechatronics QUIZ-1Document4 pagesSri Ramakrishna Institute of Technology, Coimbatore-10: Mechatronics QUIZ-1Veerakumar SNo ratings yet
- General InformationDocument13 pagesGeneral InformationRamón Eduardo ColmenaresNo ratings yet
- Description of Compucut® GO Scope of SupplyDocument2 pagesDescription of Compucut® GO Scope of SupplyKanniyappan GounderNo ratings yet
- My Updated CVDocument5 pagesMy Updated CVSaleem UddinNo ratings yet
- LS Retail Training Manual Version 4.2Document170 pagesLS Retail Training Manual Version 4.2MOHAMMED AARIFNo ratings yet
- A Guide For Using PTM and The CIBANO 500 To Test Circuit Breakers in North AmericaDocument36 pagesA Guide For Using PTM and The CIBANO 500 To Test Circuit Breakers in North AmericaargaNo ratings yet
- IAY G05 C Part 2Document43 pagesIAY G05 C Part 2lokelooksNo ratings yet
- Geotechnical Big Fish Career StoriesDocument53 pagesGeotechnical Big Fish Career Storieskrainaoz2011No ratings yet
- ST Vid10523-St444Document65 pagesST Vid10523-St444Sistel HuanucoNo ratings yet
- Computer Education ModuleDocument22 pagesComputer Education ModuleJulia Melissa CzapNo ratings yet
- Joaquín Vélez: 1 HOTEL CENTRAL PARK - NYC - Construction EngineerDocument2 pagesJoaquín Vélez: 1 HOTEL CENTRAL PARK - NYC - Construction EngineerVaé RiberaNo ratings yet
- Parallel Port InterfacingDocument34 pagesParallel Port InterfacingKingsprincessNo ratings yet
- Panasonic Kx-ft982ls-984ls-988ls (Service Manual Repair)Document194 pagesPanasonic Kx-ft982ls-984ls-988ls (Service Manual Repair)servitecdj100% (2)
- Clark CTX40-70 A4 en 4576424Document8 pagesClark CTX40-70 A4 en 4576424RS TZNo ratings yet
- CV WiraDocument3 pagesCV WiraNi Komang Utari YulianingsihNo ratings yet
- 模型剪枝在2d3d卷积网络中的研究与应用-悉尼大学在读博士生郭晋阳 智东西公开课Document70 pages模型剪枝在2d3d卷积网络中的研究与应用-悉尼大学在读博士生郭晋阳 智东西公开课jiahao liNo ratings yet
- DesktopauditreportDocument15 pagesDesktopauditreportapi-385391462No ratings yet
- Paquete de Información de Producto: Motor 25 HP 1760 RPM Nema 284TDocument11 pagesPaquete de Información de Producto: Motor 25 HP 1760 RPM Nema 284TCarolina AlexandraNo ratings yet
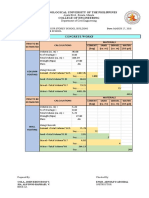
- 2 Concrete Works CompuDocument14 pages2 Concrete Works CompuALFONSO RAPHAEL SIANo ratings yet
- File Upload XSS - Hack 2 LearnDocument12 pagesFile Upload XSS - Hack 2 LearnTech HelpNo ratings yet
- SAP Product CostingDocument2 pagesSAP Product CostingRona RussellNo ratings yet
- Sihao Huang Resume 1Document2 pagesSihao Huang Resume 1api-528311148No ratings yet
- 5G Transport Network Requirements, Architecture and Key TechnologiesDocument27 pages5G Transport Network Requirements, Architecture and Key TechnologiesFreedomNo ratings yet
- Manual Teclado Ligthsys - RiscoDocument32 pagesManual Teclado Ligthsys - RiscoLuis Oliver Neciosup VasquezNo ratings yet
- Rishabh ResumeDocument4 pagesRishabh ResumeRishabh BhatiaNo ratings yet